Unmasking Latent Primary Hyperparathyroidism in Guillain-Barré Syndrome: A Case Report and Literature Review
Masahiro Biyajima, Hirotaka Oide, Jun Tsuyuzaki, Yuko Kawai

TL;DR
A 79-year-old woman with Guillain-Barré syndrome revealed hidden primary hyperparathyroidism through hypercalcemia, highlighting the need for calcium and PTH monitoring in immobilized patients.
Contribution
This case highlights how immobilization in GBS can unmask latent PHPT, emphasizing the importance of PTH screening in high-risk patients.
Findings
Prolonged immobilization in GBS can enhance bone resorption and unmask latent PHPT.
Combination therapy with elcatonin, zoledronate, and cinacalcet normalized serum calcium and alleviated symptoms.
Routine calcium and PTH monitoring is crucial in immobilized or aging populations to prevent complications.
Abstract
Primary hyperparathyroidism (PHPT), a common endocrine disorder, is often diagnosed in its asymptomatic stage. We report the case of a 79-year-old woman with Guillain-Barré syndrome (GBS) who developed progressive hypercalcemia, initially suspected to be immobilization hypercalcemia (IH). However, the detection of elevated intact parathyroid hormone (PTH) confirmed that the hypercalcemia was not solely due to prolonged immobilization associated with GBS but rather due to previously latent PHPT becoming clinically apparent. Treatment with elcatonin and zoledronate inhibited bone resorption, while cinacalcet suppressed PTH secretion, collectively normalizing serum calcium levels and alleviating symptoms. This case illustrates how prolonged immobilization in GBS can enhance bone resorption, leading to IH and unmasking latent PHPT. Recognizing this mechanism underscores the importance of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
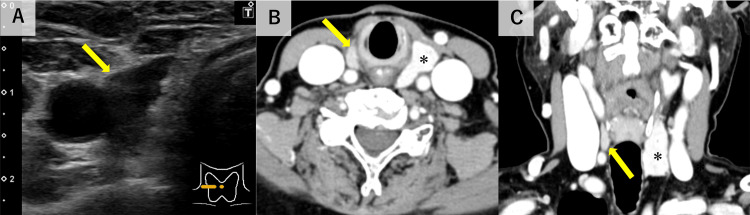 Figure 1
Figure 1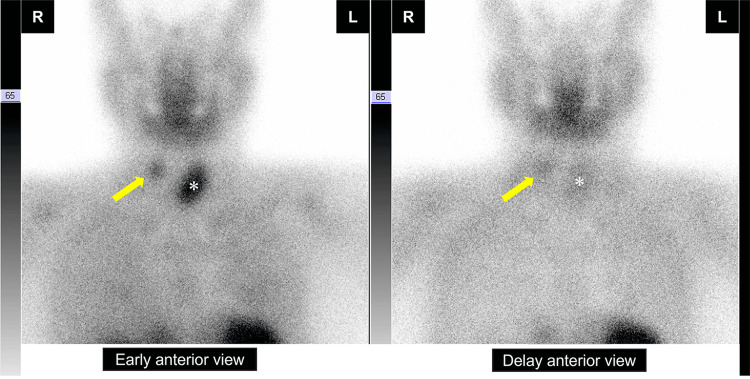 Figure 2
Figure 2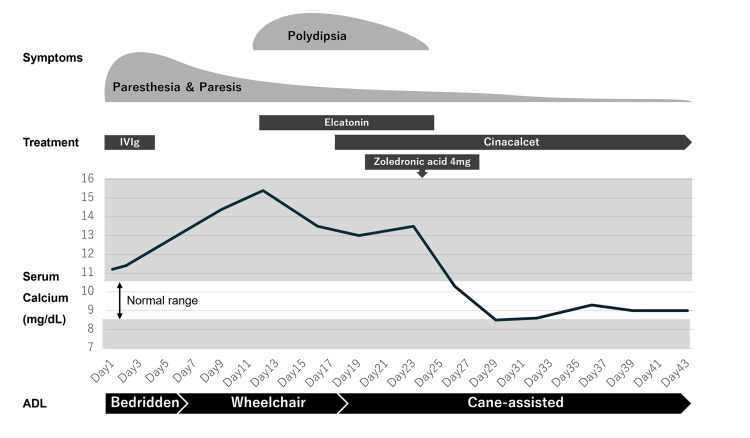 Figure 3
Figure 3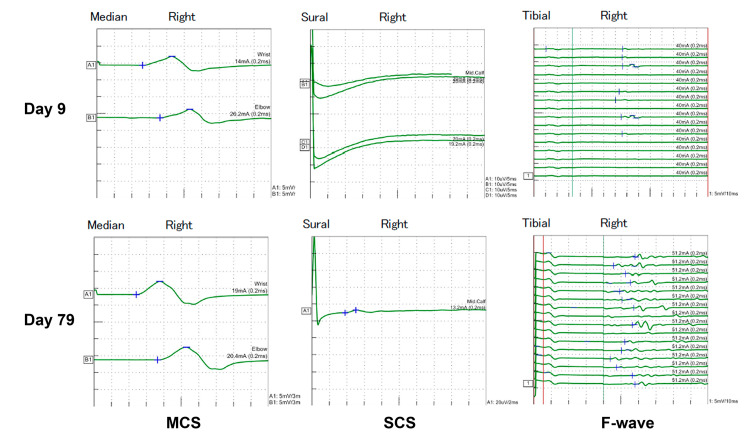 Figure 4
Figure 4| Blood count | Value | Reference range | |
| WBC | 10,900 | 3.300-8,600 | /µL |
| Neutrophil | 68.1 | 38.0-74.0 | % |
| Lymphocyte | 25.3 | 16.5-49.5 | % |
| Monocyte | 5.3 | 2.0-10.0 | % |
| Eosinophil | 0.7 | 1.0-9.0 | % |
| Basophil | 0.6 | <2.0 | % |
| RBC | 465 | 386-492×104 | /µL |
| Hb | 15.1 | 11.6-14.8 | g/dL |
| PLT | 62.9 | 15.8-34.8×104 | /µL |
| Blood coagulation test | |||
| PT (s) | 10.5 | 9.9-11.8 | s |
| PT (INR) | 1.01 | ||
| APTT (s) | 34.3 | 23-40 | s |
| D-dimer | 1.8 | <1.0 | μg/mL |
| Biochemistry | |||
| Alb | 4.3 | 4.1-5.1 | g/dL |
| Cre | 0.62 | 0.46-0.79 | mg/dL |
| BUN | 7.7 | 8-20 | mg/dL |
| AST | 26 | 13-30 | U/L |
| ALT | 16 | 7-23 | U/L |
| LDH | 198 | 124-222 | U/L |
| Na | 141 | 138-145 | mEq/L |
| K | 4.2 | 3.6-4.8 | mEq/L |
| Cl | 108 | 101-108 | mEq/L |
| Ca | 11.2 | 8.8-10.1 | mg/dL |
| P | 2.1 | 2.7-4.6 | mg/dL |
| UA | 5.9 | 2.6-5.5 | mg/dL |
| CRP | 0.12 | <0.14 | mg/dL |
| Intact PTH† | 139 | 10-65 | pg/mL |
| PTHrP† | <1.0 | <1.1 | pmol/L |
| Citation | Age/Sex | Trigger for Manifestation | Parathyroid Lesion |
| Eze et al. (2024) [ | 15/M | Ramadan fasting | Adenoma |
| Golbus et al. (2023) [ | 73/F | Amiloride (potassium-sparing diuretic) | Adenoma |
| Akhanlı et al. (2020) [ | 49/M | Dapagliflozin (SGLT-2 inhibitors) | Adenoma |
| Khan et al. (2017) [ | 17/M | Calcium and vitamin D replacement therapy | Adenoma |
| Yanamandra et al. (2016) [ | 35/F | ATRA therapy | Adenoma |
| Bala et al. (2015) [ | 38/F | Vitamin D replacement therapy | Adenoma |
| Asghar et al. (2012) [ | 55/F | Vitamin D replacement therapy | Adenoma |
| Hannan et al. (2004) [ | 43/ N/A | Vitamin D replacement therapy | Adenoma |
| Taylor et al. (1997) [ | 43/F | Vitamin D replacement therapy | Adenoma |
| Taylor et al. (1997) [ | 54/M | Vitamin D replacement therapy | N/A |
| Forbes et al. (1995) [ | 88/F | Etidronate and calcium carbonate | N/A |
| Monno et al. (1993) [ | 38/M | Guillain-Barré Syndrome | Adenoma |
| Peter et al. (1993) [ | 63/F | L-thyroxine | Adenoma |
| Hollands et al. (1983) [ | 43/F | Nephrectomy | Adenoma |
| Graze et al. (1981) [ | N/A | Lithium therapy | Adenoma |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Parkinson's Disease and Spinal Disorders · Neurological and metabolic disorders
Introduction
Primary hyperparathyroidism (PHPT) is a relatively common endocrine disorder with an estimated prevalence of 0.1% or higher [1]. It results from excessive secretion of parathyroid hormone (PTH), leading to hypercalcemia, which can cause a range of symptoms including fatigue, muscle weakness, neuropsychiatric disturbances, and nephrolithiasis. While many cases of asymptomatic or latent PHPT remain stable, certain conditions, medications, or physiological stressors can trigger overt disease [2]. However, the mechanisms by which latent PHPT transitions to a clinically apparent state remain incompletely understood.
Guillain-Barré syndrome (GBS) is an acute immune-mediated polyneuropathy characterized by progressive muscle weakness and areflexia due to peripheral nerve demyelination or axonal damage. Patients with GBS frequently experience immobilization, a known risk factor for hypercalcemia (immobilization hypercalcemia, IH) due to increased bone resorption. In this report, we describe a rare case in which GBS-associated immobilization led to IH, unmasking latent PHPT and resulting in the clinical manifestation of hypercalcemia. This case highlights the importance of recognizing prolonged immobilization as a potential trigger for the clinical onset of PHPT in patients with previously undiagnosed disease. Early biochemical assessment in immobilized patients may be crucial in identifying underlying endocrine disorders and preventing complications associated with IH and PHPT.
Case presentation
A 79-year-old woman was admitted to the hospital after a fall resulting in a left fibular fracture. She reported a two-day history of limb numbness and muscle weakness before the fall, which progressively led to difficulty walking. Upon arrival, she was alert, and her vital signs were stable. However, deep tendon reflexes in all limbs were absent, and muscle strength was reduced to a manual muscle test (MMT) grade of 3-4. Grip strength was 7/10 kg. Pathologic reflexes were absent, and glove-and-stocking-type sensory impairment was observed. Based on her clinical course and physical findings, she was diagnosed with GBS, characterized by progressive peripheral neuropathy. She was administered a five-day course of intravenous immunoglobulin (IVIg) therapy and continued rehabilitation.
Blood tests at admission revealed mild hypercalcemia with a corrected calcium level (Payne’s formula) of 11.2 mg/dL (reference range: 8.8-10.1 mg/dL), which worsened progressively during her hospitalization. The laboratory findings at admission are summarized in Table 1.
Renal function was normal. She had no history of supplementation with vitamin D or thiazide diuretics, ruling out drug-induced hypercalcemia. Additionally, her fractional excretion of calcium (FeCa) was 6.8% (≥1), excluding familial hypocalciuric hypercalcemia. IH due to immobilization associated with GBS was suspected, and hydration therapy was initiated. Her prolonged immobilization due to GBS was considered a contributing factor to the worsening hypercalcemia. However, her intact PTH level was elevated at 139 pg/mL (reference range: 10-65 pg/mL); parathyroid hormone-related peptide (PTHrP) was negative. The patient had a history of right thyroid lobectomy for a thyroid tumor at the age of 37. Neck ultrasound revealed an 11×5×11-mm mass to the right side of the trachea (Fig. 1A), which was confirmed on contrast-enhanced neck computed tomography (CT) as an enhancing mass in the same location (Fig. 1B, 1C).
Neck ultrasound and contrast-enhanced computed tomography(A) Neck ultrasound shows an 11×5×11-mm mass to the right side of the trachea (arrow). Contrast-enhanced computed tomography (B: axial view, C: coronal view) shows an enhanced mass on the right side of the trachea (arrows). The asterisk indicates the left lobe of the thyroid gland.
Technetium-99m sestamibi scintigraphy showed tracer accumulation in the right cervical region (Fig. 2), and we diagnosed her with PHPT.
Technetium-99m sestamibi scintigraphyTechnetium-99m sestamibi scintigraphy shows increased uptake in the right parathyroid gland (arrow). The asterisk indicates the left lobe of the thyroid gland.
As hypercalcemia worsened due to ongoing PTH overproduction, she developed polydipsia, which resolved following treatment with elcatonin, cinacalcet, and zoledronate (Fig. 3).
Summary of the clinical course of the patientParesthesia and paresis improved gradually following IVIg treatment, leading to improved ADL. After hospitalization, serum calcium levels increased gradually, and polydipsia appeared on Day 10. Treatment with elcatonin, cinacalcet, and zoledronate successfully normalized serum calcium levels, resulting in the resolution of polydipsia.
Her muscle strength improved, allowing her to increase mobility progressively, and rehabilitation was continued. Nerve conduction studies revealed improved amplitudes of compound muscle action potentials (CMAP) and sensory nerve action potentials (SNAP), as well as increased F-wave persistence, confirming objective improvement in her peripheral neuropathy (Fig. 4). She was discharged home on Day 62.
Nerve conduction studies in the acute and recovery phasesNerve conduction studies revealed improved amplitudes of CMAP and SNAP, as well as increased F-wave persistence. CMAP: compound muscle action potentials, MCS: motor conduction study, SCS: sensory conduction study, SNAP: sensory nerve action potentials.
Discussion
Immobilization hypercalcemia
IH was first described by Albright et al. in 1941 [3]. Since then, numerous cases and reviews have been reported, reflecting its clinical importance. While the pathophysiology of IH is incompletely understood, increased bone resorption due to the loss of mechanical stimulation to the skeleton is considered a key factor [4]. The causes of immobilization vary widely, including postoperative states such as abdominal surgery [5] and bariatric surgery [6], and conditions such as stroke [7], traumatic brain injury [8], spinal cord injury [9], burns [10], and COVID-19 [11]. Similar to the present case, two earlier reports have described IH triggered by GBS [12, 13].
In IH, PTH levels are typically reactively suppressed, with hypercalcemia resulting primarily from abnormalities in bone turnover. Hypercalcemia with normal or suppressed PTH levels is classified as parathyroid-independent hypercalcemia, a condition characterized by elevated calcium levels unrelated to primary hyperparathyroidism [14], of which IH is one example. Treatment during immobilization typically involves hydration and administration of elcatonin, bisphosphonates, or denosumab. Once mobility is restored, hypercalcemia often resolves without further intervention. However, in cases of irreversible immobilization, continued supportive therapy may be required.
In the present case, IH due to immobilization associated with GBS was initially suspected; however, elevated intact PTH levels confirmed the diagnosis of PHPT. The prolonged immobilization associated with GBS led to IH, which subsequently unmasked latent PHPT. This case adds to the growing evidence that prolonged immobilization, including that associated with GBS, can serve as a key trigger for unmasking latent PHPT. In such cases, resolution of immobilization alone is insufficient for fundamental improvement, and therapeutic intervention targeting PHPT is necessary.
Latent PHPT
PHPT is a relatively common endocrine disorder and, along with malignancies, is among the frequent causes of hypercalcemia [15]. Malignancy-associated hypercalcemia (MAH) occurs due to mechanisms such as PTHrP secretion, osteolytic bone metastases, or excess calcitriol production, and is a key differential diagnosis of PHPT. In countries with widespread multi-panel biochemical screening, PHPT is often detected early in its asymptomatic stage through routine testing [16]. However, insufficient PTH testing in hypercalcemic patients has been reported, suggesting underdiagnosis of PHPT [17]. Disturbances in calcium homeostasis can manifest several years before clinical diagnosis and latent PHPT is characterized as normocalcemic hyperparathyroidism or normoparathyroid hypercalcemia [18].
In latent PHPT, immobilization can exacerbate hypercalcemia, as observed in the present case. A similar case of PHPT identified following the onset of GBS has been previously reported. Key differentiating features between IH and PHPT include a consistently high PTH level, lack of PTH suppression during the calcium infusion test, and the ineffectiveness of oral etidronate for hypercalcemia management [19].
Latent PHPT cases, along with the triggers leading to their unmasking, are summarized in Table 2.
A literature search using PubMed was conducted to identify studies related to subclinical, asymptomatic, latent, unmasked, and masquerading hyperparathyroidism. Among the 100 search results, 15 studies were selected based on relevance and available information [16, 19-31]. Details of the search strategy are provided in the legend of Table 2. This review focuses specifically on cases where asymptomatic or latent PHPT became clinically evident due to specific triggers, excluding cases where PHPT was diagnosed incidentally without prior symptoms. The most common triggers for the unmasking of PHPT were medications, in particular, vitamin D supplementation. Lithium, a well-known cause of drug-induced hyperparathyroidism, can unmask cases of PHPT not caused by the drug itself [31]. Severe PHPT can present as a parathyroid crisis [25], highlighting the importance of PTH measurement and screening for parathyroid tumors, even in cases of mild hypercalcemia. In the reviewed cases, parathyroid adenomas were identified in all patients. While parathyroidectomy is the definitive treatment for PHPT, surgical indications for asymptomatic cases remain controversial. Most patients, including the present case, receive conservative management [32, 33].
With an aging global population, the prevalence of immobilization due to bedridden states is expected to rise. Additionally, the incidence of hip fractures is projected to nearly double between 2018 and 2050 [34], likely resulting in increased immobilization-related conditions. Consequently, cases of PHPT unmasked by immobilization, similar to the present case, are expected to become more frequent. Drug-induced hypercalcemia, serving as a trigger for PHPT diagnosis, will likely persist as a significant clinical concern. Regularly monitoring calcium levels and screening parathyroid function are crucial to prevent severe hypercalcemia. Early therapeutic intervention for patients requiring treatment is essential to ensure optimal outcomes.
Limitations
A limitation of this study is the potential omission of relevant cases due to deficiencies in the PubMed search strategy. The search query may not have captured all instances of unmasked PHPT, given the condition’s prevalence and variability in terminology across studies. Additional triggers beyond those identified in this review may also exist. Further case reports and studies are needed to better define the circumstances under which PHPT becomes unmasked.
Conclusions
This case illustrates how prolonged immobilization associated with GBS can unmask latent PHPT. Although IH due to prolonged immobilization was initially suspected, persistently elevated PTH levels confirmed the diagnosis of PHPT. The progression of hypercalcemia despite standard IH management necessitated targeted PHPT treatment, emphasizing the need for thorough biochemical evaluation in immobilization-related hypercalcemia. Asymptomatic PHPT is often underdiagnosed, with triggers such as immobilization and medications precipitating its clinical manifestation. Given the rising prevalence of immobilization-related conditions, recognizing latent PHPT and its potential triggers is essential. Routine calcium and PTH monitoring in immobilized patients may enable early detection and timely intervention, preventing complications associated with PHPT and IH.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence and prevalence of primary hyperparathyroidism in a racially mixed population J Clin Endocrinol Metab Yeh MW Ituarte PH Zhou HC 112211299820132341831510.1210/jc.2012-4022 PMC 3590475 · doi ↗ · pubmed ↗
- 2Subclinical and asymptomatic parathyroid disease: implications of emerging data Lancet Diabetes Endocrinol Macfarlane DP Yu N Leese GP 329340120132462241810.1016/S 2213-8587(13)70083-4 · doi ↗ · pubmed ↗
- 3Acute atrophy of bone (osteoporosis) simulating hyperparathyroidism J Clin Endocrinol Albright F Burnett CH Cope O Parson W 71171611941
- 4The response of bone to unloading J Bone Miner Metab Bikle DD Halloran BP 2332441719991057558710.1007/s 007740050090 · doi ↗ · pubmed ↗
- 5Immobilization-induced hypercalcemia in a patient with renal failure Endocrinol Diabetes Metab Case Rep Gandhi A Mortensen M Sunny S Techathaveewat P Targovnik J Alsayed M 2021202110.1530/EDM-21-0086 PMC 855887834612208 · doi ↗ · pubmed ↗
- 6Immobilization hypercalcemia in critical illness following bariatric surgery Obes Surg Alborzi F Leibowitz AB 8718731220021256819810.1381/096089202320995736 · doi ↗ · pubmed ↗
- 7The relationship between bone mineral density and immobilization duration in hemiplegic limbs Ann Nucl Med Demirbag D Ozdemir F Kokino S Berkarda S 6957001920051644499610.1007/BF 02985119 · doi ↗ · pubmed ↗
- 8Immobilization induced hypercalcemia Clin Cases Miner Bone Metab Cano-Torres EA González-CantúA Hinojosa-Garza G Castilleja-Leal F 46471320162725274510.11138/ccmbm/2016.13.1.046PMC 4869954 · doi ↗ · pubmed ↗