Effects of Clinical Education on Occupational Therapy Students’ Professional Identity: A Cross-Sectional Study in Japan
Atsushi Niwa, Yuki Hiraga, Ryuji Matsuda

TL;DR
This study found that clinical training influences occupational therapy students' professional identity, particularly in personal growth and societal contribution.
Contribution
The study empirically examines how clinical education affects professional identity in occupational therapy students in Japan.
Findings
Clinical education increased 'confidence in personal growth' among students.
Students with clinical training showed higher 'desire to contribute to society'.
No significant difference was found in 'professional pride' or 'view of the medical profession'.
Abstract
Introduction: Occupational therapy students may form professional identities during clinical training, but this is yet to be verified. This study aimed to clarify the influence of clinical training instructors on the formation of professional identity among occupational therapy students during clinical training. Specifically, we compared the professional identities of occupational therapy students who had not received clinical training with those who had. Methods: Seventy-five occupational therapy students participated in this cross-sectional study. Of these, 41 were classified into the clinical education group and 34 into the inexperienced group. This study measured professional identity in the clinical education and inexperienced groups. Student’s t-test was conducted for statistical analysis to compare professional identity outcomes in four subcategories: “confidence in personal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
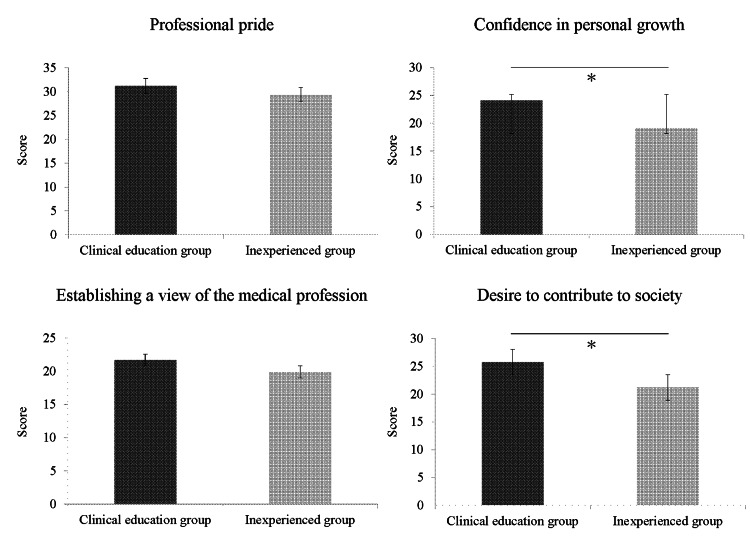 Figure 1
Figure 1| Clinical education group (n = 41) | Inexperienced group (n = 34) | t or χ2 | p | |
| Age (years) | 21.1 ± 0.1 | 20.7 ± 0.9 | 3.96 | 0.135 |
| Male, n (%) | 9 (22.0) | 13 (38.2) | 2.37 | 0.126 |
| Female, n (%) | 32 (78.0) | 21 (61.8) |
| Clinical education group (n=41) | Inexperienced group (n=34) | t | p | Mean (95% CI) | Effect size | |
| Professional pride | 31.2 ± 8.7 | 29.4 ± 9.2 | 0.86 | 0.39 | 1.8 (-2.3 to 5.9) | 0.20 |
| Confidence in personal growth | 24.1 ± 5.7 | 19.1 ± 5.9 | 3.70 | 0.01 | 4.9 (2.03 to 7.6) | 0.88 |
| Establishing a view of the medical profession | 21.6 ± 4.1 | 19.8 ± 6.1 | 1.52 | 0.13 | 1.8 (-0.5 to 4.1) | 0.36 |
| Desire to contribute to society | 25.7 ± 6.3 | 21.2 ± 7.1 | 2.92 | 0.01 | 4.5 (1.4 to 7.6) | 0.68 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOccupational Therapy Practice and Research
Introduction
In recent years, clinical training involving clinical participation has attracted attention, and clinical experience has become more important than traditional training styles [1]. Participatory clinical training is a format in which students participate as part of a medical team and acquire the knowledge, skills, and basic attitudes required by occupational therapists through modeling with a clinical training instructor [2].
Theoretical and clinical processes constitute the framework for occupational therapy education, and clinical education has been considered an important part of the traditional occupational therapy curriculum [3]. Occupational therapy clinical education aims to provide occupational therapy students with the professional skills required to apply theoretical concepts to practical situations under the supervision of occupational therapists [4]. The American Occupational Therapy Association has placed clinical education at the core of the occupational therapy curriculum to enable occupational therapy students to integrate knowledge, professional reasoning, and professional practice content and to develop the knowledge, skills, and motivation necessary to become competent occupational therapists [5].
However, in recent years, a decline in motivation to learn among university students has been noted; research has been conducted on the issue of motivation to learn [6]. In psychology, motivation is broadly divided into extrinsic motivation, which avoids shame or punishment for learning (e.g., not being able to earn credit), and intrinsic motivation, which is driven by one’s own interests and curiosity. Intrinsic motivation leads to more effective learning [7]. Identity formation directly promotes independent learning among university students and indirectly through motivation [8]. Furthermore, a study on the relationship between identity as a form of extrinsic motivation and intrinsic motivation reported a positive correlation between the two variables [9]. For these reasons, the effects of occupational therapy clinical training are expected to be felt by students modeling on a professional model (training instructor) during clinical training involving clinical participation. This contributes to the formation of professional identity, leads to intrinsic motivation, and increases motivation to learn; however, these points have not been clarified in detail. Thus, the research question established for this study was whether the professional identity of occupational therapy students is influenced by their clinical training. Specifically, the study aimed to clarify whether clinical education of occupational therapy students at our university influences their professional identity.
Materials and methods
Study design
This was a cross-sectional study. The participants were occupational therapy students from the Department of Occupational Therapy at Fukuoka International University of Health and Welfare, Faculty of Medical Sciences, Japan. Fukuoka International University of Health and Welfare is an international training institution accredited by the World Federation of Occupational Therapists (WFOT).
Ethical considerations
All patients involved in this study provided informed consent, and the study was approved by the Ethics Review Board of Fukuoka International University of Health and Welfare (approval number: 23-fiuhw-002).
Participants
This study included 34 third- and 41 fourth-year occupational therapy students. The 34 third-year students were assessed before their clinical education, and the 41 fourth-year students were assessed after their second clinical education. Therefore, the third-year occupational therapy students were classified into the inexperienced group (n = 34), and the fourth-year occupational therapy students into the clinical education group (n= 41).
Sample size calculation
In this study, sample size estimation was performed using the G*Power 3 analysis program [10]. The power was set at 0.95, and the significance level (α) was set at 0.01 [11]. In a previous study, the effect size of the clinical education score for occupational therapy was 0.50 [12]. The appropriate sample size for comparing the two groups, the clinical education group and the naive group, was 28 patients per group (n = 56).
Clinical education
The study period for this cross-sectional study was from September 2023 to October 2024. The students attended university lectures according to the curriculum of the Department of Occupational Therapy from the third to the final year and from the first to the final year of university for four years (university curriculum).
According to the curriculum of Fukuoka International University of Health and Welfare or the Department of Occupational Therapy, occupational therapy students are required to attend lectures from the first to fourth years [12]. The curriculum gradually progresses from basic fields in the first year to specialized fields tailored to occupational therapy evaluation in the second year. In the third year, students receive clinical education based on occupational therapy practice at medical institutions [12].
In the occupational therapy evaluation training, students are assigned to actual patients in hospitals or facilities across areas such as physical, mental, developmental, and geriatric disabilities. They conduct occupational therapy evaluations and then consider the necessary occupational therapy practice over 20 days [12]. In the comprehensive occupational therapy training, students are assigned to patients in hospitals and facilities in the same areas and gain experience in assessment, planning, and implementation of occupational therapy over 80 days. This training equips them with the knowledge, skills, and motivation required to become occupational therapists [12]. The clinical education provided to the students in the present study comprised both occupational therapy assessment and comprehensive occupational therapy training [12].
Assessment
The clinical education group (n = 41) and the inexperienced group (n = 34) were administered measures of professional identity.
Professional identity
Professional identity was assessed using survey items on professional identity among medical students conducted by Iwata et al. [13]. The participants were asked to respond to 32 questions on a five-point scale from 1 “not at all” to 5 “a great deal.” The 32 questions were classified into four subcategories: “confidence in personal growth,” “professional pride,” “establishing a view of the medical profession,” and “desire to contribute to society” [13]. A higher score on the professional identity scale indicated a more established professional identity.
Statistical analysis
The Shapiro-Wilk test was conducted for the distribution of normality. Student’s t-test was conducted to analyze age differences, while chi-square tests were conducted to examine sex disparities, both at a significance level of 5%. Student’s t-test was also performed with a risk level of 5% to compare the interpretations of professional identity, namely, “confidence in personal growth,” “professional pride,” “establishing a view of the medical profession,” and “desire to contribute to society,” before and after the clinical education among the occupational therapy students. The effect size indicators and standards were set as follows: small: 0.20; medium: 0.50; and large: 0.80. Statistical analyses were performed using JMP version 14.0 (JMP, Cary, USA).
Results
Participant characteristics
Table 1 presents the participants’ basic attributes. The participants were 75 occupational therapy students who were divided into two groups: the clinical education group (n = 41) and the inexperienced group (n = 34). The results of the baseline analysis indicated no significant differences in sex or age between the two groups.
Table 1: Participant characteristicsValues are expressed as means ± standard deviation Age differences were assessed by conducting Student’s t-test, while sex disparities were assessed using chi-square tests.
Analysis of the professional identity results
Table 2 summarizes the clinical education and inexperienced groups’ outcomes. A comparison between the clinical education group and the inexperienced group is also shown in Figure 1. Differences in professional identity between the two groups were analyzed by conducting Student’s t-test, revealing significant results for “confidence in personal growth” and “desire to contribute to society” (all p < 0.01) for both groups. These results suggest that receiving approximately 100 days of clinical education from occupational therapist instructors promoted the students’ “confidence in personal growth” and “desire to contribute to society.” However, as we could not analyze the specific progression of clinical education for each student, the exact process leading to these developments remains unclear.
Comparison of the clinical education group and the inexperienced group Significant differences were observed between the clinical education group and the inexperienced group (p < 0.01)*
In contrast, “professional pride” and “establishing a view of the medical profession” did not differ significantly between the two groups (all p > 0.05). These results suggest that even with the approximately 100 days of clinical education under the guidance of the occupational therapists, the students were not affected in terms of “professional pride” or “establishing a view of the medical profession.” Given the scarcity of an occupational therapy system in Japan that accounts for the country’s cultural and social backgrounds, ensuring “professional pride” and “establishing a view of the medical profession” may be difficult.
Furthermore, the effect size for “professional pride” was small at 0.20, for “confidence in personal growth”, it was large at 0.88, for “establishing a view of the medical profession”, it was small at 0.36, and for “desire to contribute to society” was medium at 0.68. These results suggest that the impact of clinical education on professional integrity primarily stems from its effects on “confidence in personal growth” and “desire to contribute to society.” However, based on the effect sizes, the effect of clinical education on “professional pride” and “establishing a view of the medical profession” appears to be limited.
In addition, the differences in each outcome between the clinical education group and the inexperienced group were as follows: 1.8 (-2.3 to 5.9) for “professional pride,” 4.9 (2.0 to 7.6) for “confidence in personal growth,” 1.8 (-0.5 to 4.1) for “establishing a view of the medical profession,” and 4.5 (1.4 to 7.6) for “desire to contribute to society.” The differences for “professional pride” and “establishing a view of the medical profession” were approximately 1.8, while the differences for “confidence in personal growth” and “desire to contribute to society” were approximately 5, highlighting a numerical disparity. However, since minimal clinically important differences have not been reported for measures of professional identity [13], the clinical significance of these differences remains unclear.
Discussion
This study aimed to clarify the influence of clinical training instructors on the formation of professional identity among occupational therapy students during clinical education in our department. To this end, participants were classified into two groups, namely, the clinical education group and the inexperienced group, and their professional identities were compared. The results showed that the occupational identity dimensions of “confidence in personal growth” and “desire to contribute to society” were significantly higher in the clinical education group than in the inexperienced group. However, “professional pride” and “establishing a view of the medical profession” did not reach significance. Therefore, by receiving clinical education from clinical training instructors, occupational therapy students can develop a professional identity, such as “confidence in personal growth” and “desire to contribute to society,” which is a novel aspect of this study.
Previous research has shown that students’ professional identities are formed through active communication with faculty [14]. Furthermore, professional identity formation includes entering into clinical roles, enriching clinical work, and personal growth [15]. Therefore, we believe that the clinical education provided in this study was thorough and students were given proactive roles, which may explain why “confidence in personal growth” and “desire to contribute to society” showed higher values in the clinical education group.
However, “professional pride” and “establishing a view of the medical profession” did not reach significance in the clinical education or the inexperienced group. Previous studies have reported that time spent in professional roles also influences professional identity [16]. The duration of the clinical education in this study was 100 days, with some participants receiving 20 and others receiving 80 days. It is possible that professional identity such as “professional pride” and “establishing a view of the medical profession” was not formed. Occupational therapists’ professional identity formation involves occupation-centered practice, ontological reflexivity, theory-practice alignment, and professional socialization [17]. Professional pride and social contribution associated with this identity require long-term practice, both as a student and as a professional [18]. Therefore, we believe that gaining extensive practical experience in one’s specialty is essential for developing a professional identity characterized by “professional pride” and for “establishing a view of the medical profession.” In other words, in this study, the clinical education group also showed high scores for the professional identity items “confidence in personal growth” and “desire to contribute to society,” while no significance was observed in either the clinical education group or the inexperienced group for “professional pride” and “establishing a view of the medical profession.” Therefore, although the clinical education conducted in this study did not lead to the formation of “professional pride” and “establishing a view of the medical profession,” it may be possible to encourage the formation of “confidence in personal growth” and “desire to contribute to society.” Based on these findings, enhancing clinical education and university education is necessary to promote the formation of professional identity in occupational therapy education [19].
Regarding the clinical usefulness of the findings, we believe that incorporating approximately 100 days of clinical education into the university curriculum can help foster a professional identity rooted in “confidence in personal growth” and a “desire to contribute to society.” Furthermore, by working long-term as occupational therapists, individuals can develop “professional pride” and “establish a view of the medical profession.” To achieve this, establishing a system that ensures a consistent connection between university education and post-graduate education (career development) is necessary.
Although this study offers valuable insights, it also has some limitations. First, the study was cross-sectional and conducted at a single university, which makes it difficult to generalize the findings. Second, the participants were divided into a clinical education group and a non-clinical education group based on their clinical education, so inferring a causal relationship between the two groups is not possible. Third, the clinical education group received clinical education in hospitals, elderly care facilities, developmental support centers, and psychiatric rehabilitation facilities, but the specific characteristics of each facility were not examined thoroughly. Consequently, we could not analyze in detail how “confidence in personal growth” and “desire to contribute to society” evolved during the clinical education process, while “professional pride” and “establishing a view of the medical profession” did not. Fourth, the content of the clinical education likely varied between institutions, making it challenging to explore all aspects in detail. To address this situation, it may be possible to first select a training field that corresponds to the students’ interests. Thus, in the future, a more detailed analysis could be possible by investigating the specific training fields that students are interested in. Finally, the study only considered age and sex as participant attributes, disregarding other potential confounding factors such as work experience, personality traits, and motivation. Future studies should consider these limitations.
Conclusions
This study aimed to clarify whether the clinical education of occupational therapy students at our university influences their professional identity. The results showed that the occupational identity dimensions of “confidence in personal growth” and “desire to contribute to society” were significantly higher in the clinical education group than in the inexperienced group. However, “professional pride” and “establishing a view of the medical profession” did not reach significance. These results suggest that clinical education can promote the formation of professional identities among occupational therapy students.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Economic evaluation of simulated and traditional clinical placements in occupational therapy education Aust Occup Ther J Gospodarevskaya E Carter R Imms C 3693796620193068073810.1111/1440-1630.12563 · doi ↗ · pubmed ↗
- 2Simulated versus traditional occupational therapy placements: a randomised controlled trial Aust Occup Ther J Imms C Froude E Chu EM 5565646520183016858110.1111/1440-1630.12513 · doi ↗ · pubmed ↗
- 3Which models can be used as a clinical education model in occupational therapy? Introduction of the models: a scoping review study Med J Islam Repub Iran Pashmdarfard M Soltani Arabshahi K Shafaroodi N Hassani Mehraban A Parvizi S Haracz K 76342020 https://pubmed.ncbi.nlm.nih.gov/33306054/3330605410.34171/mjiri.34.76PMC 7711038 · doi ↗ · pubmed ↗
- 4Factors affecting the clinical education of rehabilitation students in Iran: a systematic review Med J Islam Repub Iran Pashmdarfard M Shafarood N 1143220183081540910.14196/mjiri.32.114PMC 6387815 · doi ↗ · pubmed ↗
- 5Continuing education requirements among State Occupational Therapy Regulatory Boards in the United States of America J Educ Eval Health Prof Hall SR Crifasi KA Marinelli CM Yuen HK 371320162778035110.3352/jeehp.2016.13.37PMC 5121188 · doi ↗ · pubmed ↗
- 6Modelling the factors that affect medical students’ occupational identity in long COVID: an integrated perspective of motivation, opportunity and ability Humanit Soc Sci Commun Yan J Wu M Liao Y 258112024
- 7Intrinsic motivation, curiosity, and learning: theory and applications in educational technologies Prog Brain Res Oudeyer PY Gottlieb J Lopes M 25728422920162792644210.1016/bs.pbr.2016.05.005 · doi ↗ · pubmed ↗
- 8Students’ achievement values, goal orientations, and interest: definitions, development, and relations to achievement outcomes Dev Rev Wigfield A Cambria J 135302010