Evaluation of serial erythrocyte sedimentation rate and C-reactive protein monitoring in infectious disease outpatient parenteral antimicrobial therapy patients
Katarina Jackson, John J. Veillette, Jared Olson, Allan M. Seibert, Brandon J. Webb

TL;DR
A study found that blood tests like ESR and CRP rarely influenced treatment decisions for outpatient antibiotic therapy and may add unnecessary costs.
Contribution
The study identifies a potential for cost savings by reducing unnecessary ESR and CRP monitoring in infectious disease outpatient care.
Findings
Only 12.5% of patients had clinical decisions influenced by ESR or CRP.
Unnecessary ESR/CRP monitoring added $530 per treatment course.
The average treatment duration was 5.1 weeks.
Abstract
Of 313 patients whose outpatient parenteral antimicrobial therapy was managed by an ID physician, only 39 [12.5%, 95% CI (8.8%–16.1%)] had clinical decisions influenced by erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), or both. ESR/CRP ordering was associated with $530 in excess cost per treatment course (average duration 5.1 weeks) representing a diagnostic stewardship opportunity.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
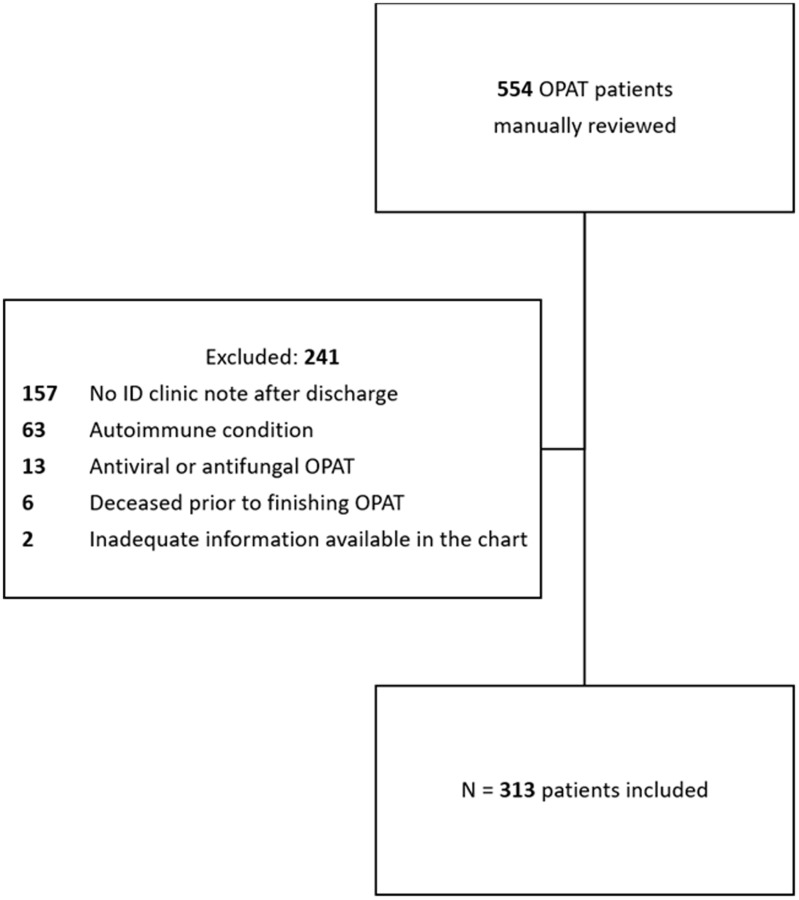 Figure 1
Figure 1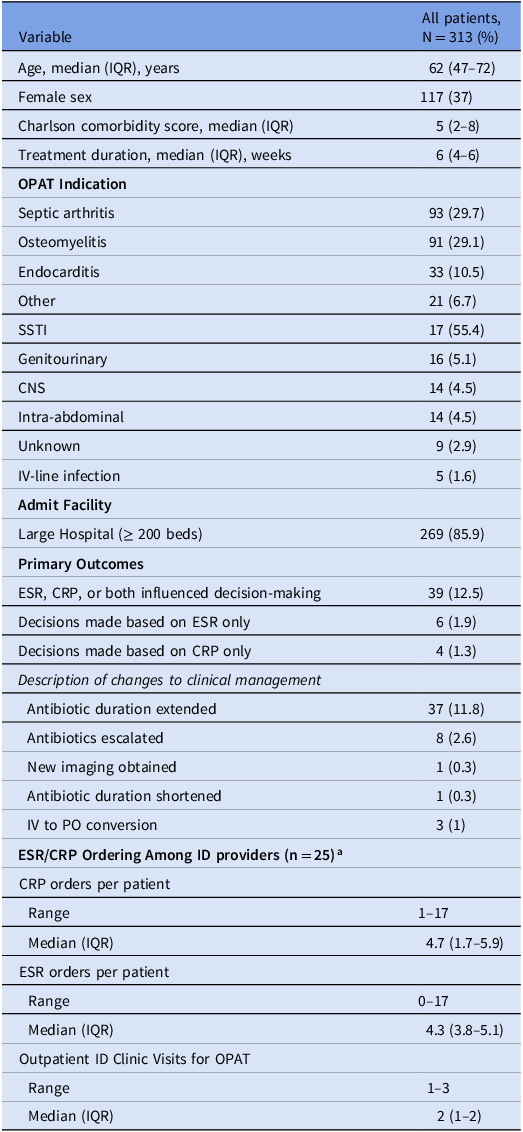 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Orthopedic Infections and Treatments · Bacterial Identification and Susceptibility Testing
Introduction
Outpatient parenteral antimicrobial therapy (OPAT) is often used as an effective, less costly alternative to inpatient treatment of severe infections.^ 1 ^ To ensure OPAT safety, both the Infectious Disease Society of America (IDSA) and UK Good Practice Recommendations endorse serial monitoring of complete blood cell counts, renal panels, and liver function tests.^ 1,2 ^ However, these guidelines lack recommendations for monitoring of inflammatory markers for efficacy [e.g. erythrocyte sedimentation rate (ESR), C-reactive protein (CRP)]. While ESR and CRP assist in the initial diagnosis of several infectious conditions,^ 3–5 ^ the utility of serial monitoring is unknown. To our knowledge, repeat ordering of ESR/CRP is only recommended in two IDSA guidelines: prosthetic joint infections (at the end of treatment prior to 2^nd^ stage revision), and vertebral osteomyelitis (after 4 weeks of antimicrobial therapy).^ 3,4 ^ IDSA’s diabetic foot infection guideline neither recommends for nor against serial ESR/CRP monitoring, citing only one study that found that CRP failed to predict treatment failures.^ 5,6 ^ In our own healthcare system (in the absence of standardized OPAT monitoring guidelines), we have observed the ordering of weekly ESR/CRP for various indications, which might represent a diagnostic stewardship opportunity. Herein, we evaluate the utility of serial ESR/CRP monitoring for clinical decision-making in OPAT management.
Methods
We identified unique patients (any age) who were discharged on OPAT between 11/2022–4/2023 from one of 23 Intermountain Health (IH) hospitals, followed by an IH infectious diseases (ID) physician and had at least 2 ESRs or 2 CRPs ordered by the same ID physician within 6 weeks of discharge. Patients were then excluded for the following reasons: no ID clinic note after discharge, autoimmune condition (identified by ICD-10 code), antiviral or antifungal OPAT, deceased prior to finishing OPAT, or inadequate information in the ID clinic note to determine clinical management. Hospital course, comorbidities, demographics, laboratory values, and microbiology data were extracted electronically, whereas OPAT indication (selected from a standardized list) and aspects of clinical management were abstracted manually from the electronic medical record (EMR).
The primary outcome was the percentage of patients for whom an ID physician documented in the chart that ESR and/or CRP influenced decision-making, defined as a change in antibiotics (duration, dose, route, or regimen) or any other aspect of clinical management (e.g. ordering repeat imaging or labs, or arranging future visits). Subgroup analyses were performed to assess provider ordering variability and to stratify decision-making by OPAT indication. Lastly, we described the percentage of ESR/CRPs that were within normal limits, and direct lab costs (cost of lab test plus labor) associated with monitoring that did not appear to influence clinical decisions within 2 weeks following the test result (i.e. excess lab orders). Descriptive statistics were utilized in all analyses. This study was exempted by the IH Institutional Review Board as a quality improvement project.
Results
Of 554 patients reviewed, 313 (56.5%) met inclusion criteria (Figure 1). Most patients were male (196 [62.6%]) with a median age of 62 (IQR 47–72). The most common indications for OPAT were septic arthritis (93 [29.7%]), osteomyelitis (91 [29.1%]), and endocarditis (33 [10.5%]). Demographics, baseline characteristics, lab ordering, clinical decision-making, and ID Clinic visit details are included in Table 1. Based on EMR documentation, 39/313 patients (12.5%, [95% CI 8.8%–16%]) had a clinical decision influenced by ESR, CRP, or both at any time during their OPAT course. Notably, inflammatory markers were most often used in combination with other clinical factors to decide on management: few patients had decisions made based on ESR only (6 [1.9%]) or CRP only (4 [1.3%]). Most clinical decisions based on ESR only (5/6, 83%) or CRP only (3/4, 75%) were in bone and joint infections (osteomyelitis or septic arthritis).
Figure 1.Inclusion/exclusion criteria. Abbreviations: CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; ID, infectious diseases; OPAT, outpatient parenteral antimicrobial therapy.
Table 1.Demographics, antibiotic treatment, and outcomesVariableAll patients, N = 313 (%)Age, median (IQR), years62 (47–72)Female sex117 (37)Charlson comorbidity score, median (IQR)5 (2–8)Treatment duration, median (IQR), weeks6 (4–6) OPAT Indication Septic arthritis93 (29.7)Osteomyelitis91 (29.1)Endocarditis33 (10.5)Other21 (6.7)SSTI17 (55.4)Genitourinary16 (5.1)CNS14 (4.5)Intra-abdominal14 (4.5)Unknown9 (2.9)IV-line infection5 (1.6) Admit Facility Large Hospital (≥ 200 beds)269 (85.9) Primary Outcomes ESR, CRP, or both influenced decision-making39 (12.5)Decisions made based on ESR only6 (1.9)Decisions made based on CRP only4 (1.3) Description of changes to clinical management Antibiotic duration extended37 (11.8) Antibiotics escalated8 (2.6) New imaging obtained1 (0.3) Antibiotic duration shortened1 (0.3) IV to PO conversion3 (1) **ESR/CRP Ordering Among ID providers (n = 25)^a^**CRP orders per patient Range1–17 Median (IQR)4.7 (1.7–5.9)ESR orders per patient Range0–17 Median (IQR)4.3 (3.8–5.1)Outpatient ID Clinic Visits for OPAT Range1–3 Median (IQR)2 (1–2)CRP, C-Reactive Protein; ESR, Erythrocyte Sedimentation Rate; IQR, interquartile range; IV, intravenous; OPAT, outpatient parenteral antimicrobial therapy; PO, by mouth. a All 25 ID providers, all OPAT indications.
There was notable variability in inflammatory marker ordering among the 25 included ID providers (Table 1, all OPAT indications). This variability persisted when limiting the evaluation to bone and joint infections only (n = 20 ID providers): CRP – range 1–17 orders per OPAT course, median 5.7 (IQR 4.5–6.1); ESR – range 0–17 orders per OPAT course, median 4.9 (IQR 4.2–5.7).
Of 1,336 ESRs obtained, 434 (32.4%) were within normal limits (≤ 20 mm/hr) and of 1,575 CRPs obtained, 811 (51.5%) were within normal limits (≤ 1 mg/dL). Evaluating specific OPAT indications, 10.5% (52/493), 20.1% (96/478), and 5.5% (5/91) of ESRs versus 10.1% (54/535), 22% (117/533), and 5.6% (8/143) of CRPs contributed to decision-making for septic arthritis, osteomyelitis, and endocarditis, respectively. There was no evidence that ESR/CRP-related decisions were made for any other OPAT indication. Across all infection types, an average of 5 excess CRPs and 4 excess ESRs per OPAT course (average 5.1 weeks) were ordered (estimated average excess cost 165,890 for 313 patients in 6 months, or $331,780 per year).
Discussion
Only 12.5% of serial ESR and CRP orders appeared to influence clinical decision-making in our ID OPAT patients. Several factors likely contributed to these findings, and we offer the following suggestions to optimize ESR/CRP ordering based on our data: First, ESR and CRP were ordered weekly, but clinic visits with the ID physician occurred less often (generally 1–2 visits per OPAT course). In conditions where ESR/CRP trending is indicated, clinicians should consider decreasing monitoring frequency to preceding a clinical visit or at the start and end of therapy (although this may represent operational challenges). Second, up to 30% of ESRs and 50% of CRPs were within normal limits. Discontinuing ESR/CRP after normalization is likely low-hanging fruit for diagnostic stewardship. Third, ESR/CRP values did not appear to influence decision-making outside of bone and joint infections or endocarditis, and perhaps these labs should be avoided for other OPAT indications. Lastly, ESR did not appear to add value to CRP when both were ordered. Because ESR takes longer to normalize and CRP is a better measure of acute-phase response,^ 7 ^ we intend to remove ESR from our OPAT note template.
While our study uniquely evaluated the utility of serial ESR/CRP ordering in ID OPAT patients, it had many limitations. We relied on EMR documentation to provide the rationale behind clinical decisions, and it is possible that decisions were made without chart documentation. Furthermore, while these data reflect our healthcare system’s practices, it is possible that ID physicians elsewhere rely more on ESR/CRP when making decisions. We did not separate orthopedic hardware-related infections from native bone and joint infections, a distinction that is needed in future studies on this topic. We also did not identify malignancies that might influence ESR/CRP values. We did not evaluate appropriateness of clinical decisions, and it is possible that some decisions (e.g. extending antibiotics based on ESR only) might have been unnecessary; thus, limiting OPAT ESR/CRP surveillance might also have potential as an antibiotic stewardship intervention. Chart review was completed by one independent reviewer, who was not blinded to the study objectives. Finally, we did not correlate lab monitoring or decision-making with clinical outcomes, which is an important area of future study. Such studies are needed so OPAT guidelines can recommend specific frequencies of lab monitoring based on safety and efficacy data.
In summary, ESR and CRP rarely influenced clinical decision-making in our ID OPAT patients and were associated with substantial costs. This likely represents a diagnostic stewardship opportunity to decrease excess monitoring and costs for patients and healthcare systems.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Norris AH , Shrestha NK , Allison GM , et al. 2018 Infectious diseases society of America clinical practice guideline for the management of outpatient parenteral antimicrobial therapy. Clin Infect Dis 2019;68:1–4.30551156 10.1093/cid/ciy 867 · doi ↗ · pubmed ↗
- 2Chapman ALN , Patel S , Horner C , et al. Updated good practice recommendations for outpatient parenteral antimicrobial therapy (OPAT) in adults and children in the UK. JAC Antimicrob Resist 2019;1:dlz 026.34222901 10.1093/jacamr/dlz 026PMC 8209972 · doi ↗ · pubmed ↗
- 3Osmon DR , Berbari EF , Berendt AR , et al. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the infectious diseases society of America. Clin Infect Dis 2013;56:e 1–e 25.23223583 10.1093/cid/cis 803 · doi ↗ · pubmed ↗
- 4Berbari EF , Kanj SS , Kowalski TJ , et al. 2015 Infectious diseases society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adults. Clin Infect Dis 2015;61:e 26–46.26229122 10.1093/cid/civ 482 · doi ↗ · pubmed ↗
- 5Senneville É , Albalawi Z , van Asten SA , et al. IWGDF/IDSA guidelines on the diagnosis and treatment of diabetes-related foot infections (IWGDF/IDSA 2023). Clin Infect Dis 2023;79:ciad 527.10.1093/cid/ciad 52737779457 · doi ↗ · pubmed ↗
- 6Pham TT , Wetzel O , Gariani K , et al. Is routine measurement of the serum C-reactive protein level helpful during antibiotic therapy for diabetic foot infection? Diab Obes Metab 2021;23:637–641.10.1111/dom.1422233026129 · doi ↗ · pubmed ↗
- 7Markanday A. Acute phase reactants in infections: evidence-based review and a guide for clinicians. Open Forum Infect Dis 2015;2:ofv 098.26258155 10.1093/ofid/ofv 098PMC 4525013 · doi ↗ · pubmed ↗