Outcomes associated with asymptomatic bacteriuria management in elderly patients hospitalized with a ground-level fall
Katelin A. Everitt, Margaret Baldwin, Nick Tinker, Ku’ulei Stuhr, David S. Morris, John J. Veillette

TL;DR
Treating asymptomatic bacteriuria in elderly patients who fall does more harm than good and offers no benefits.
Contribution
Demonstrates clear harm from treating ASB in elderly fall patients, supporting current IDSA guidelines.
Findings
Antibiotic treatment for ASB in elderly fall patients caused harm.
No benefits were observed from treating ASB in this population.
Alternative causes of falls should be evaluated instead of treating ASB.
Abstract
Data are lacking to guide management of asymptomatic bacteriuria (ASB) in elderly patients with a fall. Comparing treated versus non-treated patients, we identified clear harm and no benefit from antibiotic treatment. Our data support IDSA recommendations to withhold antibiotics in elderly patients with ASB and evaluate alternative causes of falls.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
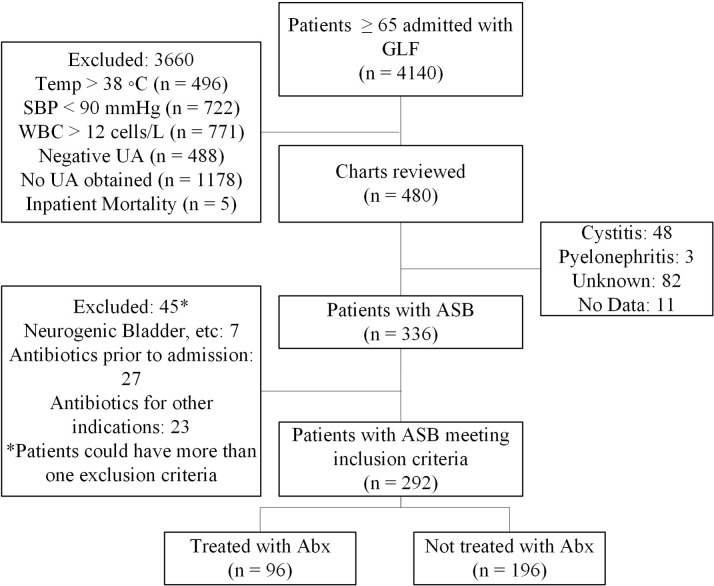 Figure 1
Figure 1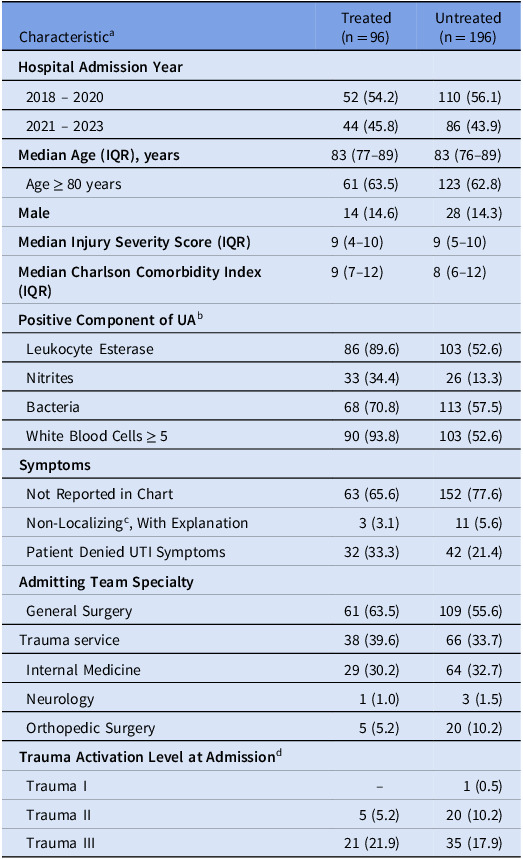 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Thermal Regulation in Medicine · Pelvic floor disorders treatments
Background
Asymptomatic bacteriuria (ASB), a positive urine culture (UC) without symptoms of a urinary tract infection (UTI), affects up to 50% of elderly adults.^ 1 ^ Randomized trial data support Infectious Disease Society of America (IDSA) recommendations against antibiotic treatment of ASB in numerous patient populations. However, data are lacking to support IDSA’s recommendation among elderly patients with a fall and ASB to observe and assess for other causes rather than treat with antibiotics. Overprescription of antibiotics for these patients leads to adverse events and delayed diagnosis of other conditions causing falls (e.g. dehydration, stroke, medication effects),^ 2,3 ^ while undertreatment might pose a theoretical risk of future UTI. Several studies have described ASB overtreatment in elderly patients, but comparative outcomes data are needed in elderly patients with a fall, which often prompts urine testing and treatment.^ 2–8 ^ Herein, we describe outcomes associated with ASB management in elderly patients hospitalized for a ground-level fall (GLF) at an urban 503-bed, level 1 trauma center.
Methods
Patients ≥ 65 years of age hospitalized for a GLF requiring trauma service consultation between 1/2018 and 8/2023 were identified for screening. We then excluded patients electronically who had systemic signs of infection (temperature >38^o^C, systolic blood pressure <90 mmHg, or white blood cell count >12,000/µL), no urinalysis (UA) obtained, negative UA (negative leukocyte esterase, nitrites, bacteria, and <5 white blood cells per high-powered field),^ 9 ^ or who died during admission. The UA, rather than UC, was used because antibiotics are often prescribed for UA results before the UC is available. Patients were then excluded during manual chart review if they had cystitis or pyelonephritis symptoms (dysuria, urgency, frequency, suprapubic pain, flank pain, costovertebral angle tenderness), received antibiotics prior to admission, or received antibiotics for non-UTI indications. Patients with only non-localizing symptoms (e.g. abdominal pain) were classified as ASB if a clear non-UTI diagnosis was documented as the cause. If no clear non-UTI diagnosis was recorded in patients with non-localizing symptoms, the patient was classified as unknown and excluded from the analysis. Finally, we excluded patients who might experience UTI without typical symptoms (e.g. dementia, chronic urinary catheter, anuria, urologic cancer, or neurogenic bladder) and those with possible UTI based on imaging (e.g. bladder wall thickening). The remaining patients with ASB were split into two cohorts: those treated (inpatient and/or prescription upon discharge) versus not treated with antibiotics.
Demographics, comorbidities, hospital course, antibiotic treatment, laboratory values, vital signs, trauma activation level, Injury Severity Score, Charlson Comorbidity Index, and all-cause mortality and readmissions were obtained electronically, whereas manual review was used to assess UTI symptoms and the most likely cause of any readmissions.
The primary outcome was 90-day all-cause readmission, with description of subcategories (e.g. readmissions from antibiotic effects or new or worsening UTI). Secondary outcomes included provider variability in antibiotic prescribing for ASB, antibiotic treatment days and associated costs, 90-day Clostridioides difficile infection (CDI), all-cause 90-day mortality, and 90-day incidence of bacteremia (with the same organism as index UC). We used a two-tailed Fisher’s Exact test for categorical data and descriptive statistics for continuous data. The Institutional Review Board exempted this study as quality improvement (1052544), and we adhered to the STROBE guidelines for reporting observational studies.^ 10 ^
Results
Of 4,140 patients screened, 480 (11.6%) were manually reviewed, and 292 (7.1%) met inclusion criteria: 96/292 (32.9%) were treated with antibiotics, and 196/292 (67.1%) were not (Fig. 1). Baseline characteristics were similar between groups, except the rates of abnormal UA findings and admission by the trauma service were numerically higher in the treated group (Table 1). All-cause readmission rates were not significantly different between the treated and untreated groups [14 (14.5%) versus 37 (18.9%), respectively, P = 0.36], nor were UTI-related readmission rates [4 (4.2%) versus 6 (3.1%), P = 0.43]. The treated group had 1 patient (1%) readmitted due to renal failure from trimethoprim-sulfamethoxazole and 1 patient (1%) who developed outpatient CDI following inpatient treatment with meropenem. There was no significant difference between the treated and untreated groups in 90-day all-cause mortality [13 (13.5%) versus 16 (8.2%), P = 0.16] or subsequent bacteremia with the index UC organism [1 (1%) versus 0 (0%), P = 0.33].
Figure 1.Inclusion/Exclusion Criteria. Abx, antibiotics, ASB, asymptomatic bacteriuria, GLF, ground-level fall, SBP, systolic blood pressure, Temp, temperature, UA, urinalysis, WBC, white blood cell count.
Table 1.Baseline characteristicsCharacteristic^ a ^ Treated (n = 96)Untreated (n = 196) Hospital Admission Year 2018 – 202052 (54.2)110 (56.1) 2021 – 202344 (45.8)86 (43.9) Median Age (IQR), years 83 (77–89)83 (76–89) Age ≥ 80 years61 (63.5)123 (62.8) Male 14 (14.6)28 (14.3) Median Injury Severity Score (IQR) 9 (4–10)9 (5–10) Median Charlson Comorbidity Index (IQR) 9 (7–12)8 (6–12) Positive Component of UA ^ b ^ Leukocyte Esterase86 (89.6)103 (52.6) Nitrites33 (34.4)26 (13.3) Bacteria68 (70.8)113 (57.5) White Blood Cells ≥ 590 (93.8)103 (52.6) Symptoms Not Reported in Chart63 (65.6)152 (77.6) Non-Localizing^ c ^, With Explanation3 (3.1)11 (5.6) Patient Denied UTI Symptoms32 (33.3)42 (21.4) Admitting Team Specialty General Surgery61 (63.5)109 (55.6)Trauma service38 (39.6)66 (33.7) Internal Medicine29 (30.2)64 (32.7) Neurology1 (1.0)3 (1.5) Orthopedic Surgery5 (5.2)20 (10.2) Trauma Activation Level at Admission ^ d ^ Trauma I--1 (0.5) Trauma II5 (5.2)20 (10.2) Trauma III21 (21.9)35 (17.9)Abx, Antibiotics; ADE, Adverse Event; SD, Standard Deviation; UA, Urinalysis; UTI, Urinary Tract Infection. a Represented as number (%) unless otherwise stated. b Patients could have more than one positive component of the UA. c Non-localizing symptoms included abdominal pain, nausea, vomiting, altered mental status, or weakness. Several patients had non-localizing symptoms (with clear non-UTI cause) and denied UTI symptoms (n = 2 in the treated group, n = 9 in the untreated group). d The remaining patients were admitted without meeting criteria for trauma activation, but the trauma service was still consulted.
Of the admitting providers for whom at least 5 patients were included [n = 11/77 (14%) of all providers in the study), the rate of antibiotic prescribing for ASB ranged from 14 to 58%. In the treated group, 379 days of antibiotics were given for ASB resulting in excess cost of USD 2.66 per day per patient in the treated group, the untreated group avoided 764 days of antibiotic therapy and saved approximately $2,033.30.
Discussion
Treating ASB with antibiotics did not benefit elderly patients hospitalized with a GLF, and there was clear evidence of harm. Our findings align with Boerckel et al.,^ 6 ^ who did not find antibiotic treatment to benefit hospitalized elderly patients with ASB and altered mental status (AMS). Notably in that study, patients for whom antibiotics were withheld had higher rates of alternative diagnoses explaining AMS. This treatment approach (i.e. avoiding anchoring on urine tests) should also be applied to GLFs, which have many causes besides UTI. Our findings support the IDSA recommendation in elderly patients with a fall to prioritize observation and investigation for other causes over antibiotic treatment of ASB.^ 1 ^
Our study was strengthened by detailed chart review and conservative exclusion criteria to identify elderly GLF patients with the highest likelihood of having ASB. These data identify low-hanging fruit for stewardship clinicians to intervene and educate providers (especially those with higher prescribing rates) to withhold antibiotics in this patient population. While most urine screening and treatment were driven by GLFs, we observed some overlap with surgeons treating ASB as peri-operative prophylaxis; hence, antibiotic review in this population might lead to multiple intervention and education opportunities.
Our study had numerous limitations. Only 7% of screened patients met inclusion criteria, which limits generalizability and implies more uncertainty in the excluded patients (some of whom might benefit from antibiotic treatment). Our retrospective data are limited by potential selection bias and reliance on documentation in the electronic medical record. Chart reviews were performed by a single clinical pharmacist, who was not blinded to the study objectives. Confounders that were not captured (e.g. undocumented UTI symptoms or pharmacist intervention to stop antibiotics) could have influenced treatment, and we could not account for readmissions to hospitals outside our healthcare system. We did not identify significant differences in readmissions, but larger studies with propensity weighted analysis could strengthen our findings. We could not capture other harms of antibiotics besides readmissions (e.g. development of antibiotic resistance). Finally, a 2021–2022 system initiative to educate providers on non-treatment of ASB could have introduced bias by altering provider documentation of UTI symptoms; however, this was likely addressed via our conservative exclusion criteria.
In summary, among elderly patients with ASB admitted for a GLF, we found evidence of harm and no clinical benefit from antibiotic treatment, which supports IDSA recommendations to observe, investigate other causes for falls, and withhold antibiotics.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nicolle LE , Gupta K , Bradley SF , et al. Clinical practice guideline for the management of asymptomatic bacteriuria: 2019 update by the Infectious Diseases Society of America. Clin Inf Dis 2019;68:e 83–e 110.10.1093/cid/ciy 112130895288 · doi ↗ · pubmed ↗
- 2Tudela P , Molinos S , Esquerrà A , Carreres A. Asymptomatic bacteriuria in emergency. A frequent cause of diagnostic error. Med Clín (English Edn) 2019;152:29–32.10.1016/j.medcli.2018.05.01829983161 · doi ↗ · pubmed ↗
- 3Long B , Koyfman A. The emergency department diagnosis and management of urinary tract infection. Emerg Med Clin North Am 2018;36:685–710.30296999 10.1016/j.emc.2018.06.003 · doi ↗ · pubmed ↗
- 4Gordon LB , Waxman MJ , Ragsdale L , Mermel LA. Overtreatment of presumed urinary tract infection in older women presenting to the emergency department. J Am Geriatr Soc 2013;61:788–792.23590846 10.1111/jgs.12203 · doi ↗ · pubmed ↗
- 5Petty LA , Vaughn VM , Flanders SA , et al. Risk factors and outcomes associated with treatment of asymptomatic bacteriuria in hospitalized patients. JAMA Inter Med 2019;179:1519–1527.10.1001/jamainternmed.2019.2871 PMC 671403931449295 · doi ↗ · pubmed ↗
- 6Boerckel HN , Worden LJ , Salvati LA , Jameson AP , Dumkow LE. Impact of altered mental status on antibiotic prescribing and outcomes in hospitalized patients presenting with pyuria. J Am Pharm Assoc 2024;64:102043.10.1016/j.japh.2024.10204338378100 · doi ↗ · pubmed ↗
- 7Caterino JM , Stephens JA , Camargo CA , et al. Asymptomatic bacteriuria vs symptom underreporting in older Emergency Department patients with suspected urinary tract infection. J Am Geriatr Soc 2020;68:2696–2699.33460062 10.1111/jgs.16775 PMC 8293680 · doi ↗ · pubmed ↗
- 8Veillette JJ , Waters CD , Olson J , et al. Outcomes of patients with bacteriuria/pyuria of clinically undetermined significance (BPCUS) treated with antibiotics in 23 community hospital emergency departments. Antimicrob Steward Healthc Epidemiol 2023;3:e 114.37502236 10.1017/ash.2023.204PMC 10369435 · doi ↗ · pubmed ↗