Lessons from a phenotypically normal infant with uniparental isodisomy of chromosome 21: a Case Report and review
Yuying Zhu, Ke Wu, Cuicui Jiang, Qiumin Zhu

TL;DR
A phenotypically normal infant was born with uniparental isodisomy of chromosome 21, highlighting the importance of genetic testing in prenatal screening.
Contribution
This case report provides new insights into the clinical outcomes of UPD of chromosome 21 in a phenotypically normal infant.
Findings
The infant had a normal phenotype despite uniparental isodisomy of chromosome 21.
No pathogenic variants were found in the homozygous region of chromosome 21.
The placental tissue showed mosaicism for trisomy 21.
Abstract
Uniparental disomy (UPD) occurs when both homologous chromosomes are inherited from a single parent. To date, the UPD of all autosomes and the X chromosome has been recorded. A few cases of UPD of chromosome 21 have been documented. At 15 weeks of gestation, a 25-year-old pregnant woman’s non-invasive prenatal screening revealed a high risk of trisomy 21. Although no anomalies were detected in the fetal ultrasonography, amniocentesis was performed, and the fetal karyotype analysis was found normal. A single-nucleotide polymorphism (SNP) array revealed that the fetus had the copy-neutral region of homozygosity (ROH) in the long arm of chromosome 21. Subsequently, single whole-exome sequencing was performed due to the risk of recessive gene variants in ROH, and no homozygous like pathogenic or pathogenic variants were found on the long arm of chromosome 21. After genetic counseling, the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
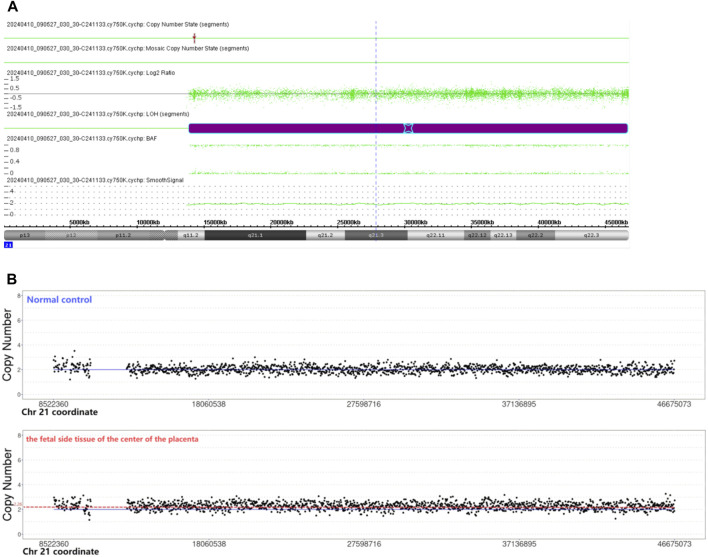 FIGURE 1
FIGURE 1| Cases | Results of molecular detection and chromosomal karyotype | Tested tissue | Clinical information |
|---|---|---|---|
|
| mUPD(21) | lymphocytes | The adult woman with normal phenotype had a newborn with trisomy 21 46,XY,t (21; 21) (q10; q10) |
|
| pUPiD (21), 45,XY,-21,-21,i (21q), | lymphocytes | The 40-year-old man with normal phenotype had a trisomy 21 son |
|
| pUPiD (21), 45,XX,-21,-21,i (21q), | NA | The adult woman with normal phenotype had a history of recurrent spontaneous abortion |
|
| mUPhD (21), 46,XX | product of conception | The mother was a 31 years old, the routine ultrasound at 8 weeks of gestation found no fetal pole |
|
| mUPhD (21) and mUPiD (21) were observed, 45,XY,-21,-21,der (21; 21) (q10; q10) | leukocytes | The one-year-old man was clinically and developmentally normal |
|
| pUPiD (21), 46,XX | product of conception (frozen fetal tissue) | The 40-year-old woman had spontaneous abortion, the focal hydrops and fibrosis of the placenta with chorionic villi showed decreased ramification and vascularization at 8 weeks of gestation |
|
| UPiD (21), 46,XX | the amniotic fluid | The 42-year-old woman received an amniocentesis at 16 weeks of gestation because of the abnormal biochemical profile and the positive result of NIPS. No fetal structure anomaly was detected on the ultrasound examination, the couple decided to terminate the pregnancy |
| This case | UPiD (21), 46,XY, | the amniotic fluid | The 6-month-old boy had normal phenotype |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPrenatal Screening and Diagnostics · Genetic Syndromes and Imprinting · Genomic variations and chromosomal abnormalities
Introduction
In uniparental disomy (UPD), both homologous chromosomes are inherited from a single parent. Based on whether both homologous chromosomes from one parent are identical, there are two subtypes of UPD: uniparental heterodisomy (UPhD) and uniparental isodisomy (UPiD). Mechanisms leading to UPD include trisomic/monosomic rescue, gamete complementation, and postfertilization errors (Liehr, 2022). Genomic imprinting depends on the parental origin of the imprinted genes, thereby resulting in the non-equivalent expression of maternal and paternal genomes (Eggermann, 2024). UPD could lead to imprinting disorders. To date, the UPD of all autosomes and the X chromosome has already been recorded. Studies have reported UPiD-caused autosomal recessive diseases detected by whole-exome sequencing. Few cases of UPD of chromosome 21 have been documented. Herein, we report a phenotypically normal infant with UPiD (21), explore previously published cases, and aim to provide useful lessons for clinical diagnosis in the future.
Materials and methods
A 25-year-old pregnant woman (gravida 0, para 0) was referred to the Center of Prenatal Diagnosis at Quzhou Maternal and Children Hospital for genetic counseling. At 15 weeks of gestation, the pregnant woman’s non-invasive prenatal screening (NIPS) showed a high risk of trisomy 21 (Z-score, 6). The patient signed an informed consent for her genetic analysis and amniocentesis. The fetal ultrasonography indicated no anomalies before the amniocentesis. Subsequently, the amniocentesis was performed at 18 weeks of gestation, and the fetal sample was detected by single-nucleotide polymorphism (SNP) array analysis, and G-banding karyotype analysis with the 400-band level.
Genetic tests of the placenta sampling
To examine the reason behind the false positive of NIPS, copy number variation sequencing (CNV-seq) was performed with low read-depth (3×) on placental tissues, umbilical cord, and cord blood for detecting the ploidy (number of sets of chromosomes in a cell or organism). Soybean-sized placental tissues symmetrically positioned at specific depths were obtained from the fetal and maternal sides of the placenta, respectively. Six samples were collected: two from the maternal side of the center of the placenta, two from the fetal side of the edge of the placenta, one umbilical cord, and one cord blood sample**.**
Results
G-banding and C-banding karyotype analysis
The G-banding karyotype analysis of 30 metaphases revealed a normal fetal amniotic fluid.
Chromosomal microarray analysis
The chromosomal microarray analysis (CMA) was done using an SNP array (Affymetrix CytoScan 750K Array, Santa Clara, California). It revealed that the fetus had the copy-neutral region of homozygosity (ROH) in the long arm of chromosome 21 (Figure 1A).
(A) Chromosomal microarray analysis indicated the copy-neutral region of homozygosity (ROH) in the long arm of chromosome 21. Smooth signal representing a normal copy number (green line) along the arm of chromosome 21. The B Allele Frequency (BAF) representing AA, and BB alleles (two green lines). (B) CNV-seq revealed the copy number of the fetal side tissue on the center of the placenta was 2.26. The copy number of the normal control was 2.
Whole-exome sequencing
Due to the risk of recessive gene variants in ROH, single WES was recommended, and WES found no homozygous likely pathogenic or pathogenic variants on the long arm of chromosome 21.
Pregnancy outcome
The pregnant woman was informed of these genetic results. There were no abnormal findings on the ultrasound throughout the entire pregnancy. After genetic counseling, this family decided to continue the pregnancy of the women. At 37 weeks of gestation, a live male infant was delivered by Cesarean section, with a length of 50 cm and a weight of 3,250 g. The 1-min and 5-min Apgar score were all 10. At the final follow-up evaluation, the 6-month-old male newborn demonstrated a normal phenotype.
Genetic results of the placenta sampling
CNV-seq revealed mosaic trisomy 21 in only the fetal side tissue on the center of the placenta, the percentage of trisomy 21 mosaicism was about 26% (Figure 1B). The other five samples were all euploid.
Discussion
Two copies of a single chromosome or chromosome segment are inherited from one parent, and no copy is inherited from the other parent, which is called UPiD (21). It was concluded that the positive result of NIPS was caused by the fetal side of the placenta of mosaic trisomy 21. It was presumed that ROH in the long arm of chromosome 21 is caused by a postzygotic trisomy 21 self-rescue event, the two remaining chromosomal 21 copies originated from the same parent, thereby resulting in UPiD (21). One in four placental samples was mosaic for trisomy 21; it suggests that postzygotic trisomy 21 trophectoderm does not rescue completely like inner cell mass, and collecting more than one placental sample is important to explore the mechanism of UPD.
There are two imprinted genes (MIR125B2, DSCAM) and one predicted imprinted gene (SIM2) found on chromosomal 21 according to the Geneimprint database (http://www.geneimprint.com/). The MIRN125B2 gene maps to chromosome 21q21.1. The paternal expression of MIR125B2 is ubiquitous in human tissues (Sonkoly et al., 2007). Chou et al. (2023) demonstrated that MIR125B2 was only imprinted in the human brain, and is associated with cognitive impairment and brain hypotrophy. Patients with Down syndrome (DS) displayed an increased level of miR-125b-2 (Farroni et al., 2018). The DSCAM gene which maps to chromosome 21q22.2-q22.3 is a paternally expressed imprinted gene in the human placenta, which would not be affected by the presence of the supernumerary chromosome 21 (Allach El Khattabi et al., 2019). DSCAM may be a candidate gene responsible for intellectual disability (Yamakawa et al., 1998), and cardiac and visceral malformations (Jannot et al., 2013).
To date, a few published cases of UPD(21) have been reported. We excluded UPD(21) cases with mosaic trisomy 21 (Bruyere et al., 2000; Chen et al., 2020; Chen et al., 2022; Chen et al., 2023), ring chromosome 21 (Bartsch et al., 1994) or a de novo mutation on the Y chromosome (Mansuet-Lupo et al., 2009). UPD(21) cases without available detailed clinical information were also excluded from the study (Nakka et al., 2019; Cavalheiro et al., 2020; Semikhodskii et al., 2023). So, only seven previously published cases of “pure” UPD(21) without mosaicism or other variations were assessed (Table 1).
Two cases were products of conception with normal karyotypes. Four cases were postnatal cases with normal phenotypes and abnormal karyotypes. Though one case had a prenatal fetus with a normal karyotype, the couple decided to terminate the pregnancy.
We reported one case with UPiD (21) that is attributed to the mechanism of trisomic rescue, and reviewed previously published cases of UPD(21). Some findings from these cases are documented as under:
-
These two imprinted genes on chromosomal 21 might not be associated with abnormal phenotype or human disease, so the presence of UPD(21) in prenatal diagnosis would be considered a favorable outcome, thereby potentially influencing the decision regarding termination of pregnancy.
-
UPiD-caused autosomal recessive diseases detected by WES have been reported previously (Zhou et al., 2024; Lopez-Garrido et al., 2022). Although UPiD (21)-caused autosomal recessive diseases have not been reported, the utilization of WES is recommended for detecting homozygous likely pathogenic or pathogenic variants on chromosome 21.
-
If the NIPS suggests a high risk of trisomy 21, the presence of confined placental mosaicism (CPM) should be considered. However, CPM involving trisomy 21 has not shown an unfavorable effect on pregnancy outcomes (Thomsen et al., 2024; Grati et al., 2020).
-
The possibility of considering the chromosome-balanced translocation should be taken into account. UPD (21) can coexist with chromosome-balanced translocations, typically der (21; 21) (q10; q10). It is likely that these carriers may encounter recurrent spontaneous abortion and have a high risk of pregnancy with trisomy 21. Therefore, chromosomal karyotype analysis is also recommended.
Overall, we also describe a phenotypically normal 6-month-old boy with UPiD (21). We also review previously published cases and sum up some useful lessons for clinical diagnosis and prenatal diagnosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Allach El Khattabi L.Backer S.Pinard A.DieudonnéM. N.Tsatsaris V.Vaiman D. (2019). A genome-wide search for new imprinted genes in the human placenta identifies DSCAM as the first imprinted gene on chromosome 21. Eur. J. Hum. Genet. 27 (1), 49–60. 10.1038/s 41431-018-0267-3 30206355 PMC 6303248 · doi ↗ · pubmed ↗
- 2Bartsch O.Petersen M. B.Stuhlmann I.Mau G.Frantzen M.Schwinger E. (1994). Compensatory uniparental disomy of chromosome 21 in two cases. J. Med. Genet. 31 (7), 534–540. 10.1136/jmg.31.7.534 7966190 PMC 1049975 · doi ↗ · pubmed ↗
- 3Blouin J. L.Avramopoulos D.Pangalos C.Antonarakis S. E. (1993). Normal phenotype with paternal uniparental isodisomy for chromosome 21. Am. J. Hum. Genet. 53 (5), 1074–1078.8213833 PMC 1682298 · pubmed ↗
- 4Bruyère H.Rupps R.Kuchinka B. D.Friedman J. M.Robinson W. P. (2000). Recurrent trisomy 21 in a couple with a child presenting trisomy 21 mosaicism and maternal uniparental disomy for chromosome 21 in the euploid cell line. Am. J. Med. Genet. 94 (1), 35–41. 10.1002/1096-8628(20000904)94:1<35::aid-ajmg 8>3.0.co;2-9 10982480 · doi ↗ · pubmed ↗
- 5Cavalheiro C. P.Avila E.Gastaldo A. Z.Graebin P.Motta C. H. A.Rodenbusch R. (2020). Uniparental disomy of chromosome 21: a statistical approach and application in paternity tests. Forensic Sci. Int. Genet. 49, 102368. 10.1016/j.fsigen.2020.102368 32911454 · doi ↗ · pubmed ↗
- 6Chen C. P.Hsu T. Y.Chern S. R.Wu P. S.Chen S. W.Wang L. K. (2023). Mosaic trisomy 21 at amniocentesis in a twin pregnancy associated with a favorable fetal outcome, maternal uniparental disomy 21 and postnatal decrease of the trisomy 21 cell line. Taiwan J. Obstet. Gynecol. 62 (1), 137–141. 10.1016/j.tjog.2022.01.012 36720527 · doi ↗ · pubmed ↗
- 7Chen C. P.Ko T. M.Chen Y. Y.Chern S. R.Wu P. S.Chen S. W. (2020). Prenatal diagnosis of low-level mosaicism for trisomy 21 by amniocentesis in a pregnancy associated with maternal uniparental disomy of chromosome 21 in the fetus and a favorable outcome. Taiwan J. Obstet. Gynecol. 59 (5), 754–757. 10.1016/j.tjog.2020.07.023 32917331 · doi ↗ · pubmed ↗
- 8Chen C. P.Liou J. D.Chern S. R.Wu P. S.Chen S. W.Wu F. T. (2022). Prenatal diagnosis of maternal uniparental disomy 21 in association with low-level mosaic trisomy 21 at amniocentesis in a pregnancy associated with intrauterine growth restriction and a favorable outcome. Taiwan J. Obstet. Gynecol. 61 (1), 146–149. 10.1016/j.tjog.2021.11.025 35181027 · doi ↗ · pubmed ↗