Is work burden associated with postmenopausal breast cancer? A population-based 25-year follow-up
Maria Kalliosaari, T. Rikkonen, R. Sund, M. Tuppurainen

TL;DR
Women with low work burden had a higher risk of developing postmenopausal breast cancer over 25 years compared to those with high work burden.
Contribution
This study identifies a novel association between low work burden and increased postmenopausal breast cancer risk over a long-term follow-up.
Findings
Women with low work burden had a 1.3-fold higher incidence of breast cancer compared to those with high work burden.
The association remained significant after adjusting for factors like BMI, MHT, and alcohol consumption.
The study followed participants for up to 25 years, providing long-term insights into work burden and breast cancer risk.
Abstract
To study the association between breast cancer and work burden over 25 years. The study was based on the Kuopio Osteoporosis Risk Factor and Prevention (OSTPRE) cohort (n = 14,220) and included women who had answered the questionnaire from the year 1994 and had no previous breast cancer. Breast cancer cases were recorded from the Finnish Cancer Registry during the study period: from 1st June 1994 till December 31, 2019. Using questionnaires, we collected information on work burden, body mass index (BMI), menopausal hormone therapy (MHT), alcohol consumption, parity, and family history of breast cancer. Work burden was categorized as low or high. Variables were used both in the univariate and multivariate Cox regression analyses to explore their associations with breast cancer. Altogether 825 women (6.9%) were diagnosed with breast cancer during the study period with a mean follow-up…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
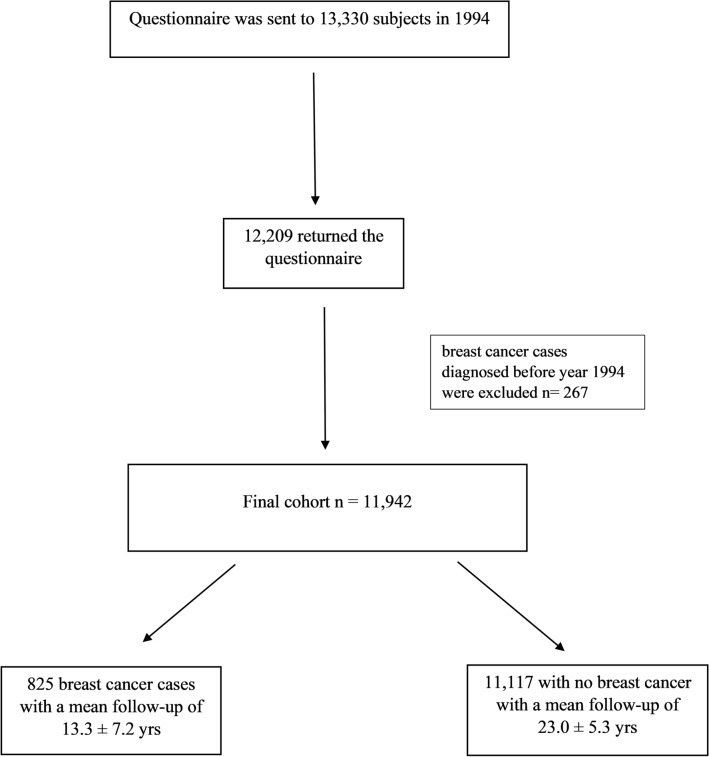 Figure 1
Figure 1- —Finnish Menopause Society
- —University of Eastern Finland (including Kuopio University Hospital)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Risks and Factors · Global Cancer Incidence and Screening · Nutrition and Health in Aging
What does this study add to the clinical work
Low self-rated work burden is related to the elevated risk of breast cancer in a 25-year follow-up study. Simultaneously, the strongest association with breast cancer was a positive family history of breast cancer and menopausal hormone therapy for 5–10 years in a population-based cohort of Finnish postmenopausal women
Introduction
Breast cancer (BC) is the most common cancer among women occurring worldwide [1] and the global cancer burden is increasing [2]. Simultaneously, mortality rates attributable to BC have decreased by nearly one-third in the past quarter century, the survival rate for BC has reached over 90% [1]. As the survival rate of BC is high, cancer affects the lives of hundreds of thousands of women worldwide. Possible modifiable risk and protective factors should be studied carefully to influence the growing incidence of BC.
There are several known risk factors for postmenopausal BC, including parity, family history, obesity, and nutritional factors such as alcohol consumption [3–7]. Recently, the possibility has been investigated that sedentary work might increase the risk of BC [8] or has no effect on it [9]. In contrast, nighttime work appears to increase the risk of BC [10, 11]. Because the findings of work burden and BC risk are conflicting and retirement age is rising worldwide while careers are longer [12, 13], it is important to further study the work burden regarding postmenopausal BC risk in a long-term follow-up.
The incidence of postmenopausal BC increases with age [1]. Because the role of work and the working environment in one’s life is growing, we wanted to investigate whether the role of work burden alters postmenopausal BC risk. The present study aimed to evaluate the role of self-rated work burden and other known risk factors for postmenopausal BC in a population-based 25-year prospective study among Finnish postmenopausal women.
Materials and Methods
This cohort study was based on the Kuopio Osteoporosis Risk Factors and Prevention (OSTPRE) cohort. The OSTPRE is a population-based ongoing follow-up study, consisting of 14 220 women born in 1932–41, aged 47–56 years in the year 1989, living in Kuopio Province, Eastern Finland. The first questionnaire was mailed to these women in spring 1989. Follow-up questionnaires were sent at 5-year intervals (in 1994, 1999, 2004, 2009, 2014, and 2019) to women who responded to the baseline questionnaire. The response rates varied between 93% (baseline) and 75% (25 years).
The BC data were obtained from the Finnish Cancer Registry (FCR). Under Finnish legislation, all cancer cases are reported to the FCR by hospitals, physicians, and pathology laboratories. Also, the death certificates with the mention of cancer are combined with the FCR. The coverage of the FCR is almost 100% in solid tumors [14].
In 1994, the 5th year OSTPRE follow-up questionnaire was sent to 13,330 women, of whom 12,209 responded. Patients with past history of breast cancer were excluded (n = 267) from the study population. Among the responders, 825 BC cases in 11,942 women were registered during the follow-up period from June 1, 1994, to December 31, 2019. Follow-up was terminated at the first occurrence of BC, emigration, death, or the end of follow-up (31st December 2019), whichever occurred first (Fig. 1).Fig. 1. Flow chart of final cohort
Questionnaires and variables
In this study, the 5-year postal inquiry from 1994 was regarded as the baseline because at this time, the work burden and family history (FH) of the BC history of the subject’s mother were inquired.
Work burden, occupation, and work history were recorded through self-reports. Initially, there were four (sedentary, low, intermediate, and high) options. Groups were recategorized by combining sedentary work and low work burden as “low work burden” while the “high work burden” group included intermediate and hard work. The low work burden category consisted of office workers, teachers, and secretaries. The high work burden category included occupations such as farmers, childminders/nursemaids, cleaners, housewives, and bakers. No information on shift work or possible night shifts was available.
The baseline health questionnaire also included additional information such as current weight (kg) and monthly alcohol consumption. Alcohol intake consisting of beer, wine, and spirits was converted into absolute ethanol consumption (g/week), with one dose equaling 12 g of absolute alcohol. Alcohol consumption (AC) groups were created according to moderate- to high-risk alcohol use in Finland [15].
The amount of smoking (cigarettes per day) and smoking history (smoking years) were converted to pack-years (years of smoking 20 cigarettes per day).
Combining variables from the 1989 inquiry, pregnancy, parity, and duration of past and present menopausal hormone therapy (MHT) use were registered and considered in the duration of MHT. Body mass index (BMI; kg/m^2^) was calculated using the current weights from the 1994 questionnaire. The date of the last menstruation was used to calculate the age at menopause for women who had intact ovaries and uteri. If the age at menopause was unknown because of removal of the ovaries or uterus, it was replaced with the mean menopausal age of the entire cohort.
Statistical analysis
The statistical analyses were performed with the Statistical Package for Social Sciences program (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp). The chi-square test and one-way ANOVA were used to compare the differences between groups. The risk ratios in terms of hazard ratios (HR) were calculated with 95% confidence intervals (CIs) with uni- and multivariable Cox regression. Continuous variables are presented as means with standard deviations.
Self-rated work burden was used as a categorical variable, with low and high work burdens. The association between work burden and BC was adjusted for covariates, including age, BMI, FH of BC, and duration of MHT and AC at baseline in the multivariable analysis. Age and BMI were used as continuous variables in the model. Parity (none vs. any), FH (no vs. yes), duration of MHT (none, under 5 years, 5–10 years and over 10 years), and AC (none, 0.1–100 g, over 100 g/week) were treated as categorical variables. P values < 0.05 were considered statistically significant.
Results
The study population consisted of 11,942 women aged 57.3 (± 2.9) years at baseline. The average age at menopause was 49.8 (± 4.3) years for women with intact uterus and ovaries. The mean follow-up for the whole cohort was 22.3 (± 6.0) years.
A total of 825 BC cases were reported in the 25-year follow-up period with the mean age at diagnosis being 70.2 (± 7.6) years. The mean follow-up of women with BC was 13.3 (± 7.2) years. In Overall, 288 (34.9%) women with BC died during the study period.
Table 1 shows the baseline characteristics of the women with BC and the entire cohort. Women with BC reported a lower work burden and more positive FH of BC than those in the reference group. Women with BC had fewer parities and used MHT for longer durations. Women with BC reported using slightly more alcohol than those without BC. Although there were more current smokers in the BC group, the pack-years smoked were lower. It had no statistical difference. (Table 1).Table 1. Baseline characteristics of the study populationVariableBreast cancerNo breast cancerP valuen = 825n = 11,117Age at baseline 1994 (years)56.9 ± 2.857.3 ± 2.9 < 0.001Age at menopause (years)50.7 ± 4.049.8 ± 4.3 < 0.001BMI (kg/m^2^)27.5 ± 4.527.3 ± 4.20.257Weight (kg)72.0 ± 12.970.5 ± 12.20.001Height (cm)162.3 ± 5.2161.1 ± 5.3 < 0.001Pregnancy (n)2.6 ± 1.82.9 ± 1.9 < 0.001No pregnancies (%)9.2%8.4%0.446Parity (n)2.4 ± 1.32.7 ± 1.4 < 0.001BC family history (%)5.6%2.6% < 0.001Smoking (never) (%)77.3%81.1%0.008Current smokers (%)15.3%14.8%0.759Pack years (years)8.3 ± 8.49.9 ± 10.20.039work burden—low (%)31.5%24.9% < 0.001work burden—high (%)68.3%63.2% < 0.001Work career (years)25.5 ± 11.024.6 ± 11.50.047Alcohol consumption (g/week)18.4 ± 30.915.8 ± 32.40.042MHT use (yrs)2.4 ± 3.91.9 ± 3.5 < 0.001MHT* menopausal hormone therapy*Differences (one-way ANOVA and chi-square test)
AC was greater in the low work burden group than in the high burden group in both the reference and BC groups, although the difference was not statistically significant (Appendix 1).
Overall, 23.6% reported no occupational education in the BC group compared to 30.2% of women without BC. Women with BC reported higher educational levels than the non-BC group (Appendix 2).
Cox regression analyses
Univariate
On univariate Cox regression analysis, low work burden was associated with a 1.3-fold higher risk for BC (95% confidence interval [CI] 1.2–1.6) than high work burden (Table 2).Table 2. Breast cancer risk factors at baselineVariableUnivariable^a^VariableMultivariable^b^Cox regressionCox regressionHR (95% CI)P valueHR (95% CI)P valueSelf-rated work burden High (n = 8108)1.0High (n = 8005)1.0 Low (n = 3023)1.3 (1.2–1.6) < 0.001Low (n = 2998)1.3 (1.1–1.5)0.003Parity None (n = 1247)1.0None (n = 1224)1.0 Any (n = 10,411)0.9 (0.7–1.1)0.385Any (n = 10,253)0.9 (0.7–1.1)0.382MHT use Non-users (n = 7116)1.0Non-users (n = 6929)1.0 Under 5 years (n = 2745)0.9 (0.8–1.1)0.333Under 5 years (n = 2692)0.9 (0.8–1.1)0.430 5–10 years (n = 1407)1.5 (1.2–1.8) < 0.0015–10 years (n = 1388)1.5 (1.2–1.8) < 0.001 Over 10 years (n = 476)1.4 (1.0–1.9)0.026Over 10 years (n = 468)1.4 (1.0–1.9)0.060Alcohol consumption Abstainers (n = 4440)1.0Abstainers (n = 4386)1.0 0–100 g/week (n = 5542)1.3 (1.1–1.5) < 0.0010–100 g/week (n = 5486)1.2 (1.0–1.4)0.014 Over 100 g/week (n = 203)1.8 (1.2–2.9)0.009Over 100 g/week (n = 200)1.6 (1.0–2.6)0.038Family history of breast cancer Negative (n = 10,241)1.0Negative (n = 10,070)1.0 Positive (n = 338)2.0 (1.5–2.7) < 0.001Positive (n = 334)1.9 (1.4–2.6) < 0.001HR hazard ratio, 95% CI 95% confidence interval, MHT menopausal hormone therapy^a^Univariate Cox regression analysis^b^Multivariable Cox regression analysis adjusted with age and BMI (kg/m^2^)
The role of positive FH was associated with a 2.0-fold higher risk for BC (95% CI 1.5–2.7) compared to those with no maternal BC history.
Higher alcohol consumption at baseline was associated with BC. A strong association was within the weekly AC of 0–100 g (HR 1.3; 95% CI 1.1–1.5). In addition, the BC risk was elevated 1.8 -fold (95% CI 1.2–2.9) if the AC was over 100 g per week compared to abstainers.
Prolonged use of MHT was associated with an elevated risk of BC. Especially in MHT users for 5–10 years and over 10 years, with an HR of 1.5 (95% CI 1.2–1.8) and 1.4 (95% CI 1.0–2.0) compared to nonusers, respectively. MHT usage for < 5 years did not play a significant role in BC risk.
Parity (none vs. any) did not play a significant role in the univariate analysis of BC risk.
Multivariable Cox regression
Self-rated work burden, MHT usage, alcohol consumption, FH of BC, parity, age, and BMI at baseline were used in the multivariable Cox regression analysis model. Low work burden was also associated with increased BC risk with HR 1.3 (95% CI 1.1–1.5) in the multivariable analysis. The strongest association with BC risk was positive FH (HR 1.9 95% CI 1.4–2.6) and MHT use of 5–10 years (HR 1.5-fold 95% CI 1.2–1.8). Moderate AC under 100 g/week was associated with a 1.2-fold (95% CI 1.0–1.4) and heavy AC over 100 g/week with a 1.6-fold (95% CI 1.0–2.6) higher risk of BC. (Table 2).
Discussion
We observed that a low work burden was associated with a higher risk of BC in a large 25-year prospective, population-based study. In addition, positive FH and prolonged MHT seemed to be the most remarkable risk factors for BC among our cohort of 11,942 Finnish postmenopausal women.
Retirement age is increasing worldwide [12]. In particular, in the 53–62 years age group, working careers are longer than in the past [13]. Studies on the effects of self-rated work burden on BC risk are limited. Our study is one of the few long-term studies exploring the relationship between work burden and BC risk over a 25-year follow-up. In addition, we adjusted for several potentially confounding factors.
A sedentary lifestyle is known to be associated with several types of cancer, including BC [4]. Obesity is associated with increased BC and mortality [3, 4]. In contrast, physical activity (PA) contributes to risk reduction in several cancers, including postmenopausal BC [3–5]. Sedentary behavior is defined as any waking behavior characterized by an energy expenditure of less than 1.5 metabolic equivalents (METs), while in a sitting, reclining, or lying posture [16]. Occupational sedentary behavior comprises approximately 60% of daily sedentary behavior [17]. The role of sedentary work in BC has been conflicting, either increasing [8] or having no association with the risk [9]. According to the World Health Organization (WHO), in 2016, globally 28% of adults were not active enough [18]. It seems that the incidence of BC is lower in occupations involving higher levels of physical activity [19]. PA contributes a greater BC risk reduction among postmenopausal women who are normal weight or overweight compared to obese women (BMI ≥ 30 kg/m^2^) [5]. PA is thought to have anti-inflammatory effects while helping to maintain normal weight and reduce the levels of sex hormones such as estradiol [4, 20]. Controversially, in our study, BMI was not associated with breast cancer, which might be due to the similarity of the mean BMI between the two groups.
Night shift work has been shown to increase the BC risk in women [10, 21]. For postmenopausal women, the BC risk was not evident, suggesting that night shift work increases the risk of BC in premenopausal women [22]. Among long-term night shift workers, a greater risk was not observed among those with over 5 years of work experience in the study by Sweeney et al. [23] or over 10 years of work experience in the meta-analyses of Manouchehri et al. [24]. In a Finnish cohort study by Härmä et al., the BC risk was increased among women aged 50 years or older, in shift workers with and without night shifts, after 10 years or more [11]. In our study population, the working careers were approximately 25 years. However, our data did not consider shift work or the possible night shifts of women, which can be considered a weakness of this study. These factors may have changed during the long study period. Work exposure was recorded only at the baseline. However, the women in the present study were near retirement age, so expectedly quite a few of them had changed work burdens.
Dong et al. suggested that a higher educational level might be associated with an increased BC risk [25]. Recently, it has been shown that higher socioeconomic status is associated with a higher incidence of BC [26]. In our study, higher educational levels and occupations with higher socioeconomic status were represented more frequently in the BC group, which points in a similar direction.
BC risk is associated with several reproductive factors such as early age at menarche, late age at first pregnancy, late menopause, and low parity [6]. Among other lifestyle factors, AC and MHT usage are associated with elevated BC risk [3, 27]. It has been shown that MHT usage for 5 years increases BC risk, with the risk being twice as high with an MHT of 10 years or more [28]. Our results point in a similar direction; however, the effect is no longer significant with the use of MHT for more than 10 years with other confounding factors. Our results did not consider MHT regimens or the route of administration and were based on self-reported use, which can introduce some bias into the results. However, a previous validation study using the same cohort showed that postal inquiry is a reliable method for recording long-term MHT use in Finnish postmenopausal women [29].
A positive association between AC and the risk of BC has been observed for decades [30]. Park et al. showed that light to moderate AC increases the risk of BC in several ethnic groups [31]. A positive dose-risk relationship was observed between AC and BC [32]. The mechanisms linking alcohol intake and a higher risk of BC are thought to involve alcohol-induced elevated estrogen levels, oxidative stress, or epigenetic changes with an altered cell cycle [32]. Our findings are consistent with those of previous studies. We did not observe a significant relationship between BC and heavy AC, which might be due to the small sample size (n = 203), as well as the possible unwillingness of heavy alcohol users to report their actual consumption.
Positive FH was associated with the highest risk of BC risk among the factors. An elevated risk is associated with a positive FH, especially in younger women [33]. This risk appears to be elevated in postmenopausal women as well [34]. Our findings outlined the impact of positive FH on BC risk.
Although occupations were widely represented in our study population, they all originated from the same geographical district and same age range in Finland. This makes the study population homogenous but may limit the generalization of the results to the entire population.
In conclusion, low work burden is associated with postmenopausal BC after adjusting for other confounding factors such as MHT, maternal history of breast cancer, and alcohol use. Further long-term studies are needed to investigate the influence of work burden on the risk of postmenopausal BC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization—WHO. International Agency for Research on Cancer 2020. https://gco.iarc.fr. Accessed 15 Jan 2021
- 2Global Burden of Disease 2019 Cancer Collaboration (2022) Cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life years for 29 cancer groups from 2010 to 2019: a systematic analysis for the global burden of disease study 2019. JAMA Oncol 8(3):420–444. 10.1001/jamaoncol.2021.698710.1001/jamaoncol.2021.6987 PMC 871927634967848 · doi ↗ · pubmed ↗
- 3Nivalainen S. Socio-economic differences: retirement and working lives in 2006, 2011 and 2017. Finnish Centre for Pensions, Studies. https://urn.fi/URN:ISBN:978-951-691-347-9
- 4Alcohol abuse. Current Care Guidelines. Working group set up by the Finnish Medical Society Duodecim and the Finnish Society of Addiction Medicine. Helsinki: The Finnish Medical Society Duodecim, 2015 (referred December 19, 2022). www.kaypahoito.fi
- 5World Health Organization (2020) Physical inactivity: a global public health problem. World Health Organization, Geneva. https://www.who.int/dietphysicalactivity/factsheet_inactivity/en/. Accessed 13 Sept 2022