Cloacal Exstrophy Associated with a Hindgut Duplication Anomaly: A Case Report of Challenges in Hindgut Preservation
Suliaman Alaqeel, Jamila Almaary, Fatmah Alrabodh, Fayez AlModhen

TL;DR
A rare case of cloacal exstrophy with hindgut duplication in an infant highlights the challenges of preserving both hindguts during surgical repair.
Contribution
This case report presents a unique approach to managing hindgut preservation in cloacal exstrophy with a hindgut duplication anomaly.
Findings
Hindgut duplication was identified during the initial repair of cloacal exstrophy in a preterm infant.
Reconstructing both hindguts into a single lumen was successfully achieved after a colo-cutaneous fistula developed.
Preservation of both hindgut ends is crucial but poses challenges due to anatomical complexities.
Abstract
Cloacal exstrophy (CE) is a rare condition, and the preservation of a short hindgut is crucial for growth, fluid-electrolyte balance, and bowel management. Herein, we present the case of an infant with concurrent anomalies and the challenges faced during the preservation of both hindguts. A preterm male infant, born at 34 weeks weighing 2 kg, was diagnosed with CE. The first stage of CE repair was performed at 3 months of age, involving the separation and tubularization of the cecal plate and the joining of the two hemi-bladders. During the procedure, hindgut duplication was noted. Each hindgut had a short mesentery with far-separated, tiny blind ends (7 and 10 cm in length), each directed toward opposite sides of the pelvis and measuring 8 Fr in caliber. Due to the risk of compromising the blood supply during rotation and mobilization of one hindgut, the decision was made to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
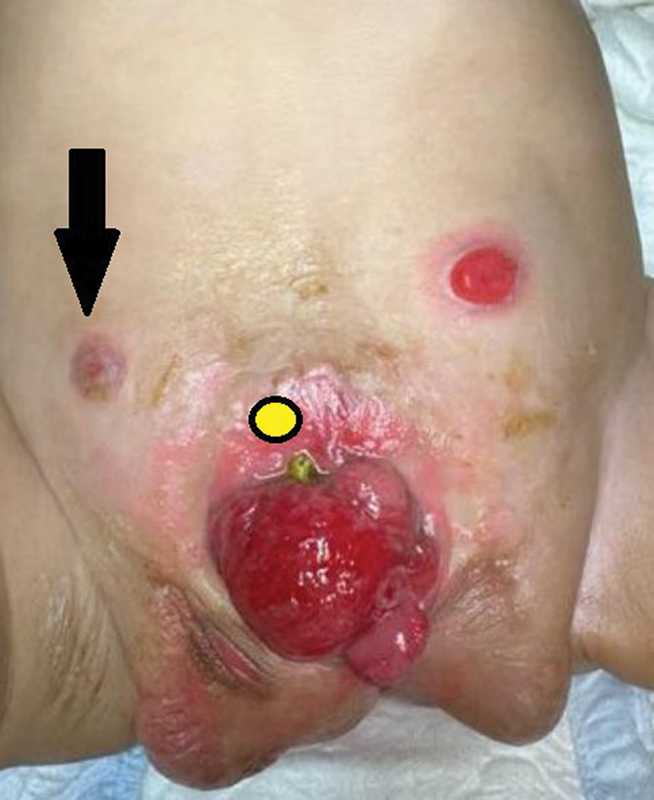 Fig. 1
Fig. 1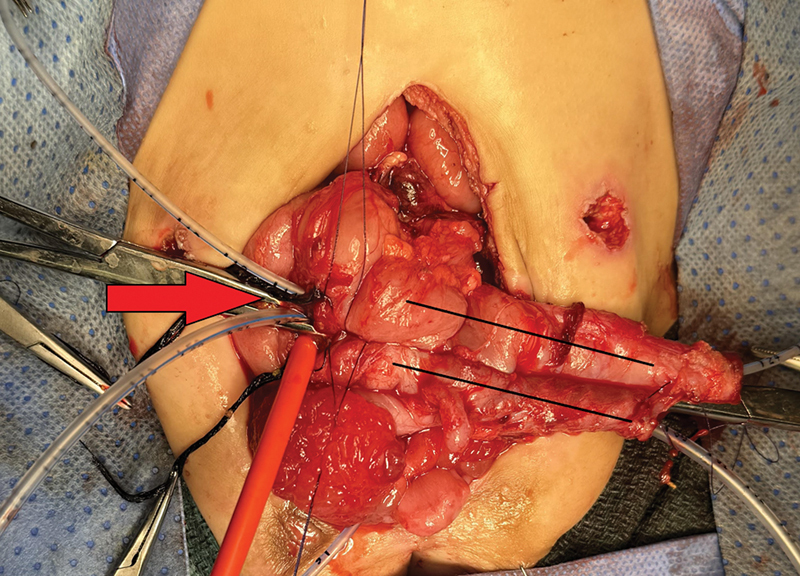 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrological Disorders and Treatments · Congenital Anomalies and Fetal Surgery · Cleft Lip and Palate Research
Introduction
Cloacal exstrophy (CE) is a rare complex anomaly with an incidence rate of 1:300,000. 1 2 Historically, management goals have focused on survival due to high mortality secondary to sepsis, electrolyte imbalance, and malnutrition. 1 3 With current advances in care and multidisciplinary approaches, the survival rate is 83 to 100%. 1 3 Consequently, the emphasis of care has evolved toward enhancing the quality of life and optimizing the functional outcomes for patients. 4 Shifting the surgical management of gastrointestinal initial reconstruction from intestinal diversion (ileostomy) to hindgut preservation with end colostomy placement has dramatically improved survival, bowel growth, and adaptation; moreover, future options include pull-through procedures and genitourinary reconstruction utilizing the intestine. 5
CE is associated with gastrointestinal, genitourinary, spine, and limb anomalies. 3 Common associations include short hindgut, appendix duplication, bladder duplication, and uterine duplication. 3 Variable hindgut lengths ranging from 2 to 20 cm and slightly longer have been reported and described. 4 6 In the general population, colon and rectal duplications represent 16% and 4% of total enteric duplications, respectively. 7 To the best of our knowledge, hindgut duplication in CE patients has been described previously in only two patients. Herein, we present an infant with similar concurrent anomalies and the challenges faced in preserving both hindguts.
Case Presentation
In a preterm 34-week-old, 2 kg, male (chromosomal analysis: XY) born with CE and the OEIS complex consisting of omphalocele, bladder exstrophy, imperforate anus, closed spinal dysraphism with lumbosacral lipomyelomeningiocele and low-lying tethered cord. First-stage CE repair was performed at 3 months of life, with separation and tubulization of the cecal plate, followed by adjoining the two hemi-bladders. Hindgut duplication was noted intraoperatively, and each blind end measured 7 and 10 cm long, with a width of 8 Fr caliber feeding tube. Each hindgut had a separate short mesentery directed separately to the pelvis sides, making a 180-degree angle between them. A trial of rotating and mobilizing one hindgut (right) was not possible, as it would jeopardize its blood supply. Thus, a decision was made to exteriorize each hindgut separately as a stoma. Both stomas started functioning as anticipated; however, a colo-cutaneous fistula developed (cecum to midline surgical wound) and was managed conservatively for 8 weeks. During this waiting time, despite the function of the left stoma, the right stoma stenosed, and the colo-cutaneous fistula persisted ( Fig. 1 ). The patient underwent a second laparotomy for fistula repair as well as reconstruction of the hindgut. During the second laparotomy, the hindgut was wider in caliber and easier to manipulate compared with the first procedure. Both hindguts were adjoined together, and side-to-side anastomosis was performed ( Fig. 2 ). A single left-end colostomy was then created. The patient was scheduled for long-term follow-up with a multidisciplinary team, including pediatric surgery, urology, neurosurgery, general pediatrics, and a clinical dietitian.
Black arrow: stenosed right stoma. Yellow circle: colo-cutaneous fistula site.
Two black lines: hindguts adjoined together with side-to-side anastomosis. Red arrow: site of the colo-cutaneous repair.
Discussion
The quality of life, growth, and hospitalization of patients with CE, especially in the first year of life, are affected by the type of gastrointestinal reconstruction, which includes ileostomy or hindgut preservation, cecal tabularization, and colostomy. 6 8 9 Saving the hindgut and avoiding ileostomy has prevented medical morbidities and mortalities secondary to metabolic derangement, dehydration, frequent hospitalizations, TPN dependence, and sepsis. 9 The surgical principles of preserving and preserving the hindgut regardless of its length and maintaining its continuity with the gastrointestinal system through cecal tuberization are well emphasized. 5 However, when facing duplication of the hindgut, new technical challenges can be encountered.
Rickham reported the first patient with hindgut duplication; both were removed, and the ileum was pulled through the perineum. 10 The patient died in 2 months of dehydration and failure to thrive. A better option is to preserve both hindguts and unify them together with side-to-side anastomosis and create a single-end stoma, as reported by Tirell et al. 7 In the report, the patient had duplicated hindguts, each with its own mesenteric blood supply. Specifically, one is directed toward the pelvis at the midline, and the other is directed toward the left paracolic gutter. Thus, 90-degree angle separation was performed, which was technically feasible at the initial surgery, to join them, and the patient survived. However, in our case, technically, both hindguts were in opposite directions, resulting in a 180-degree angle between them. An attempt to mobilize one side to join the other side was not possible, as it compromised the blood supply. Both hindguts were preserved, and two end stomas were created. Stenosis of the right end stoma secondary to decreased blood supply was a consequence of that attempt at the initial surgery.
When faced with duplicated hindguts in CE patients, one option is to resect one of the hindguts while preserving the other. If resection is deemed easier and safer, it can still be challenging to decide which hindgut to keep and which hindgut to remove, especially given uncertainties about which hindgut will function properly. Preserving both hindguts allows the fecal stream to flow through their lumens, giving each hindgut an equal opportunity for growth. Interestingly, this was observed during the second surgery in our patient. Sixty days after the initial procedure, we successfully performed an anastomosis of the two hindguts, facilitated by their increased caliber and extended mesentery. Afterward, the patient did very well, gained weight, and underwent bladder closure with bilateral osteotomy at the age of 12 months. The risk of malignancy in cases of gut duplication has been primarily documented in instances where the duplicated segment is isolated from the fecal stream and lacks continuity with the rest of the bowel. This isolation can lead to chronic inflammation and an increased potential for neoplastic changes, which was not the case in our reported case. 7
In conclusion, complex CE cases are rare, and unusual operative findings should always be anticipated. Reconstructing both hindgut ends to one end in the first setting can be challenging but possible with time, and an attempt to preserve both ends should be made. Long-term outcomes cannot be determined due to the rarity of such a presentation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Woo L L Thomas J C Brock J W Cloacal exstrophy: a comprehensive review of an uncommon problem J Pediatr Urol 201060210211119854104 10.1016/j.jpurol.2009.09.011 · doi ↗ · pubmed ↗
- 2National Birth Defects Prevention Study Keppler-Noreuil K M Conway K M Shen D Rhoads A J Carey J C Romitti P A Clinical and risk factor analysis of cloacal defects in the national birth defects prevention study Am J Med Genet A 2017173112873288528960693 10.1002/ajmg.a.38469 PMC 5650529 · doi ↗ · pubmed ↗
- 3Phillips T M Spectrum of cloacal exstrophy Semin Pediatr Surg 2011200211311821453856 10.1053/j.sempedsurg.2010.12.007 · doi ↗ · pubmed ↗
- 4Sawaya D Gearhart J P Gastrointestinal reconstruction and outcomes for patients with the OEIS complex Semin Pediatr Surg 2011200212312521453858 10.1053/j.sempedsurg.2010.12.008 · doi ↗ · pubmed ↗
- 5Bischoff A Brisighelli G Levitt M A Peña A The “rescue operation” for patients with cloacal exstrophy and its variants Pediatr Surg Int 2014300772372724817509 10.1007/s 00383-014-3512-z · doi ↗ · pubmed ↗
- 6Sawaya D Goldstein S Seetharamaiah R Gastrointestinal ramifications of the cloacal exstrophy complex: a 44-year experience J Pediatr Surg 20104501171175, discussion 175–17620105600 10.1016/j.jpedsurg.2009.10.030 · doi ↗ · pubmed ↗
- 7Tirrell T F Demehri F R Lillehei C W Borer J G Warf B C Dickie B H Hindgut duplication in an infant with omphalocele-exstrophy-imperforate anus-spinal defects (OEIS) Complex European J Pediatr Surg Rep 20221001 e 45e 4810.1055/s-0041-1742154 PMC 891317335282303 · doi ↗ · pubmed ↗
- 8Musleh L Privitera L Paraboschi I Polymeropoulos A Mushtaq I Giuliani S Long-term active problems in patients with cloacal exstrophy: a systematic review J Pediatr Surg 2022570333934734563362 10.1016/j.jpedsurg.2021.08.020 · doi ↗ · pubmed ↗