The Role of Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists in Acute Cholecystitis After a Routine Colonoscopy: A Case Report
Ahmad Abdulraheem, Dania Shukri, Nadera Altork, Usman Afzal, Mohammed Abu-Rumaileh, Alireza Meighani

TL;DR
A 66-year-old woman on semaglutide developed acute cholecystitis after a colonoscopy, suggesting a possible link between GLP-1 receptor agonists and this rare complication.
Contribution
This case report highlights a potential association between GLP-1 receptor agonists and acute cholecystitis following colonoscopy.
Findings
A patient on semaglutide developed acute cholecystitis within 72 hours of a colonoscopy.
GLP-1 receptor agonists may affect gallbladder motility, potentially increasing the risk of acute cholecystitis.
Further research is needed to determine if a washout period for GLP-1 agonists before colonoscopy is necessary.
Abstract
Colonoscopy (CLN) is a common procedure for colon cancer screening and diagnosing various conditions. Acute cholecystitis (AC), though rare, has been reported as a complication. We present a 66-year-old female on semaglutide for obesity who developed AC within 72 hours post-CLN. Considering the increasing use of glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and their impact on gallbladder motility, these medications may contribute to this complication. Future research is crucial to investigate whether a washout period for GLP-1 agonists before CLN is needed to reduce the risk of AC, if such a risk exists.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
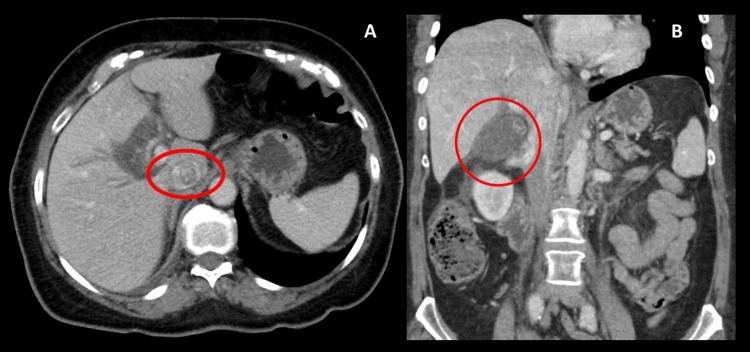 Figure 1
Figure 1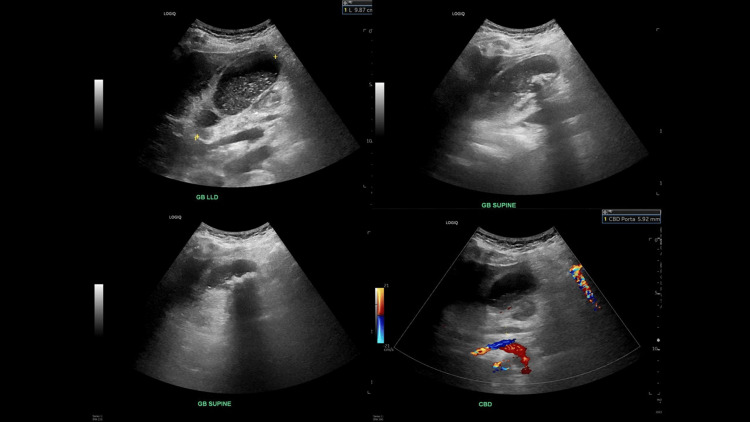 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Gallbladder and Bile Duct Disorders · Gastroesophageal reflux and treatments
Introduction
Colonoscopy (CLN) is a common procedure performed to investigate or treat various gastrointestinal (GI) conditions. Around 2.5-11% of patients may experience mild discomfort afterward, often due to endoscopic looping and the application of manual pressure [1]. Severe complications are rare, with bowel perforation being the most common, occurring in less than 0.3% of cases [2]. Other rare complications include bleeding, splenic rupture, acute appendicitis, diverticulitis, and acute cholecystitis (AC) [2,3]. Only a few cases worldwide have been reported AC following a CLN.
Notably, Milman and Goldenberg reported the first two instances of AC following a CLN [4]. In most reported cases, these complications manifested within 72 hours, with imaging studies revealing the presence of gallstones [2].
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have been widely used for glycemic control in patients with type 2 diabetes, cardiovascular mortality benefit, and weight loss. However, they have adverse effects on the GI tract motility. Woronow et al. and He et al. studied the increased risk of gallbladder and biliary system disease in patients on GLP-1 RA, especially with greater duration and higher doses [5,6].
Recently, the American Society of Anesthesiologists published consensus-based guidance, due to the absence of strong clinical data, on the pre-operative management of patients treated with GLP-1 RAs. The guidance recommends holding GLP-1 for one day in patients on daily-dosed medications and for one week in those on weekly-dosed medications prior to an elective procedure, given the potentially high risk of aspiration and anesthesia-related complications [7]. On the other hand, the American Gastroenterological Association (AGA) recommended an individualized approach for managing patients on GLP-1 RAs before endoscopy considering beforehand the reason for GLP-1 RA use, as discontinuation may pose more risk than benefit [8].
This case highlights a case report having AC after a routine CLN while taking semaglutide for obesity, and she stopped it one week before the CLN.
Case presentation
A 66-year-old female with a history of hypertension on amlodipine 5 mg daily and obesity, on the maximum dose of semaglutide (2.4 mg subcutaneous injection weekly), presented to the hospital complaining of periumbilical, sharp, non-radiating pain associated with vomiting that started one day after undergoing a screening CLN at an outside hospital. She consumed a small amount of food post-CLN, after which she began experiencing symptoms. Based on the procedure note, the CLN was uneventful and revealed only a small white patch in the rectum, and biopsy results showed normal tissue. The patient had a history of an uneventful screening CLN more than five years ago, and had been advised to withhold her semaglutide dose one week before the CLN due to its potential to cause delayed gastric emptying. She was not on any other medications, including opioids.
The patient initially presented to an urgent clinic, where an abdominal X-ray was unremarkable. As her pain continued to worsen, she sought evaluation in the emergency department. She had elevated blood pressure, tachycardia, and tenderness in the right upper quadrant on examination. Labs revealed leukocytosis (17.7k) with a neutrophilic shift, aspartate aminotransferase (AST) 26 IU/L, alanine aminotransferase (ALT) 18 IU/L, total bilirubin 1.0 mg/dl and alkaline phosphatase 57 IU/L.
Liver function tests and urinalysis were normal. CT abdomen showed mild intrahepatic biliary ductal dilatation, a distended gallbladder with gallstones, and pericholecystic fat stranding, consistent with AC (Figure 1).
CT Abdomen showing distended GB, GS in the GB and extensive pericholecystic fat stranding. A- Cross sectional view. B- Coronal sectional view. CT: Computed tomography. GB: Gallbladder. GS: Gallstones
An abdominal ultrasound showed no biliary ductal dilatation, common bile duct (CBD) diameter 0.6 cm, however, the gallbladder was moderately distended with stones and sludge, and diffuse gallbladder wall edema with trace pericholecystic fluid and positive sonographic Murphy sign (Figure 2). General surgery was planned for laparoscopic cholecystectomy, but given CT findings, an interventional radiologist was consulted for cholecystostomy tube placement.
Abdominal ultrasound showing gallbladder stones and thickened gallbladder walls.
The patient showed clinical improvement in abdominal pain and leukocytosis with conservative treatment, including IV fluids and IV antibiotics. Consequently, cholecystostomy tube placement was deferred. The patient was discharged on semaglutide and later underwent laparoscopic cholecystectomy.
Discussion
AC is commonly linked to biliary sludge or stones obstructing the CBD, particularly in patients with risk factors like obesity, pregnancy, or hemolytic anemia, leading to bile stasis and infection. However, its occurrence post-CLN remains unclear. Proposed mechanisms include dehydration from bowel preparation causing biliary stasis and gallbladder distension, especially in asymptomatic gallstone patients [3,9], bacterial translocation due to abdominal pressure during challenging procedures [9,10], and gallstone displacement into the biliary system by scope movement [9].
Fernandez-Martinez et al. and Campbell et al. reported extracolonic bacterial proliferation, including Clostridium spp., Enterococcus faecalis, and beta-lactamase-producing Escherichia coli, in pericholecystic fluid post-CLN, supporting bacterial translocation [10,11]. Warfe et al. highlighted excessive organ manipulation during CLN as a factor in cholecystitis, describing gallbladder twisting due to navigating a tortuous colon [12]. Additionally, case reports suggest that dehydration from bowel preparation may increase bile lithogenicity, potentially triggering AC.
A systematic review and meta-analysis by Liyun et al. found an increased risk of gallbladder and biliary diseases with GLP-1 RAs, particularly at higher doses, longer durations, and for weight loss [5,6]. Since higher doses are often prescribed for weight loss rather than type 2 diabetes as in our case, the risk may vary with dosage [5].
The World Health Organization-Uppsala Monitoring Centre (WHO-UMC) causality assessment classifies the reaction as "Possible," based on its temporal association (occurrence within a 72-hour timeframe) with the drug [13]. However, other contributing factors, such as dehydration, fasting, and procedural stress, along with the known effects of GLP-1 receptor agonists on gallbladder motility, could also explain the event. Similarly, the Naranjo Scale assessment resulted in a "Possible" classification (Score: 2-4), as the reaction occurred after drug administration, but alternative explanations exist [13]. Rechallenge and dechallenge data were unavailable to further assess causality, as the gallbladder was surgically removed. This rationale underscores the likelihood of this unusual adverse event pattern, suggesting that it might be more than mere coincidence.
AC following CLN is a notable concern in patients with abdominal pain and vomiting, particularly among GLP-1 RA users, given the medications' association with gastrointestinal side effects. With the increasing use of GLP-1 RAs, the potential for post-CLN cholecystitis warrants attention. An abdominal X-ray is recommended to rule out bowel perforation, and a low threshold for abdominal ultrasound is advised to assess for possible AC in the appropriate clinical context.
Conclusions
In the context of the increasing use of GLP-1 agonists for various indications, it is crucial to monitor potential side effects to prevent life-threatening complications, particularly during pre-operative evaluations. Although our patient stopped taking semaglutide (a long-acting GLP-1 RA) one week before the procedure, she unfortunately developed AC. This suggests that while AC after a CLN is typically rare, the risk may be elevated in the presence of recent high-dose GLP-1 RA use. Further research and documentation of similar cases are necessary to assess the need for a washout period for GLP-1 RAs before CLN. In the meantime, ensuring adequate patient hydration to reduce biliary stasis is essential. Additionally, risk stratification should be considered for patients with a history of gallbladder stones.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute cholecystitis, a rare complication following routine colonoscopy: case series and literature review Cureus Shaikh DH Kumar K Patel H Mehershanhi S Makker J 012202010.7759/cureus.10877 PMC 765455933194458 · doi ↗ · pubmed ↗
- 2Acute cholecystitis after a colonoscopy Ann Coloproctol Park TI Lee SY Lee JH Kim MC Kim BG Cha DH 2132152920132427886110.3393/ac.2013.29.5.213PMC 3837088 · doi ↗ · pubmed ↗
- 3Acute cholecystitis as a complication after colonoscopy: a case report and literature review Eur J Case Rep Intern Med Gorgan MM Grigorescu I Dumitrascu DL 4723201610.12890/2016_000472 PMC 634683830755891 · doi ↗ · pubmed ↗
- 4Colonoscopy cholecystitis Am J Gastroenterol Milman PJ Goldenberg SP 166696200110.1111/j.1572-0241.2001.03837.x 11374738 · doi ↗ · pubmed ↗
- 5Association of glucagon-like peptide-1 receptor agonist use with risk of gallbladder and biliary diseases: a systematic review and meta-analysis of randomized clinical trials JAMA Intern Med He L Wang J Ping F 51351918220223534400110.1001/jamainternmed.2022.0338 PMC 8961394 · doi ↗ · pubmed ↗
- 6Acute cholecystitis associated with the use of glucagon-like peptide-1 receptor agonists reported to the US Food and Drug Administration JAMA Intern Med Woronow D Chamberlain C Niak A Avigan M Houstoun M Kortepeter C 1104110618220223603693910.1001/jamainternmed.2022.3810 PMC 9425280 · doi ↗ · pubmed ↗
- 7ASA consensus-based guidance on preoperative management of patients on glucagon-like peptide-1 receptor agonists Anesthesiology Ushakumari DS Sladen RN 34634814020243798217010.1097/ALN.0000000000004776 · doi ↗ · pubmed ↗
- 8Aga rapid clinical practice update on the management of patients taking GLP-1 receptor agonists prior to endoscopy: communication Clin Gastroenterol Hepatol Hashash JG Thompson CC Wang AY 7057072220243794457310.1016/j.cgh.2023.11.002 · doi ↗ · pubmed ↗