A riddle of culprit only vs multivessel or immediate vs staged revascularization in patients with non-ST elevation acute coronary syndrome: A meta-analysis
Yudi Her Oktaviono, Jannatin Nisa Arnindita, Pandit Bagus Tri Saputra, Nabilah Azzah Putri Wairooy, Arlia Ayu Damayanti, Suryo Ardi Hutomo, Nando Reza Pratama, Makhyan Jibril Al Farabi, Faisal Yusuf Ashari

TL;DR
This study compares different PCI strategies in patients with multivessel non-ST elevation acute coronary syndrome and finds that multivessel revascularization leads to better outcomes than culprit-only approaches.
Contribution
The study provides new evidence on optimal PCI strategies for multivessel non-ST elevation acute coronary syndrome patients through a meta-analysis.
Findings
Culprit-only revascularization increases the risk of non-fatal MI and repeat revascularization.
Multistage multivessel revascularization is linked to higher mortality and repeat events.
One-stage multivessel revascularization results in fewer adverse events compared to multistage.
Abstract
Percutaneous coronary intervention (PCI) is a revolutionary breakthrough in saving many lives from myocardial infarction. However, little is known about the PCI strategy in multivessel disease (MVD) Non-ST Elevation Acute Coronary Syndrome (NSTE-ACS) patients. Should complete revascularization be achieved or culprit-only is sufficient, then when the appropriate time of multivessel revascularization is, whether it is staged or immediate. Limited evidence is available on this matter compared to ST-elevation myocardial infarction (STEMI), even though NSTE-ACS patients carry poorer long-term prognoses compared to STEMI. A thorough search for appropriate studies was executed across PubMed, Embase, Medline, Science Direct, and Scopus databases until July 4th, 2023. The risk ratio (RR) underwent analysis through Review Manager 5.4. Twenty-six studies with 222,350 MVD NSTE-ACS patients were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
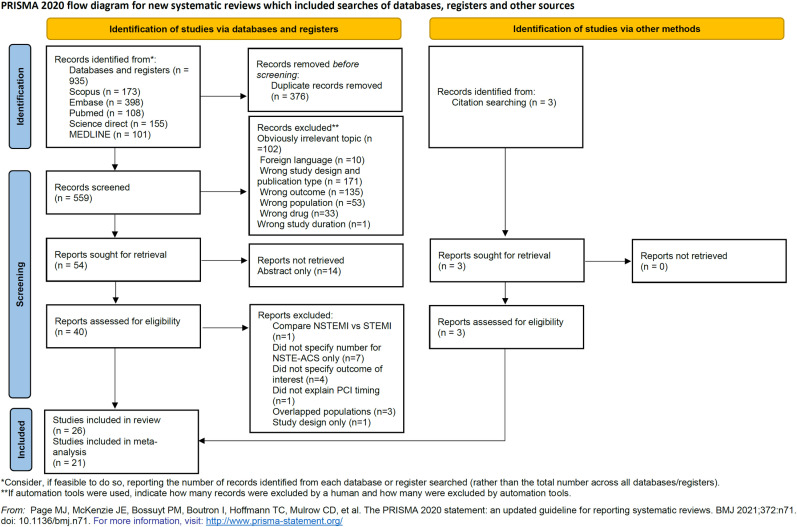 Fig 1
Fig 1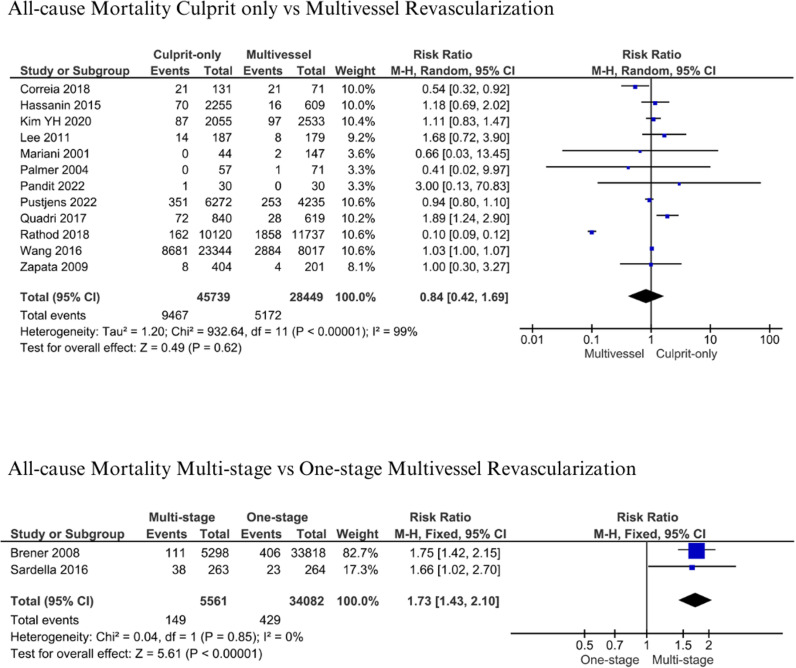 Fig 2
Fig 2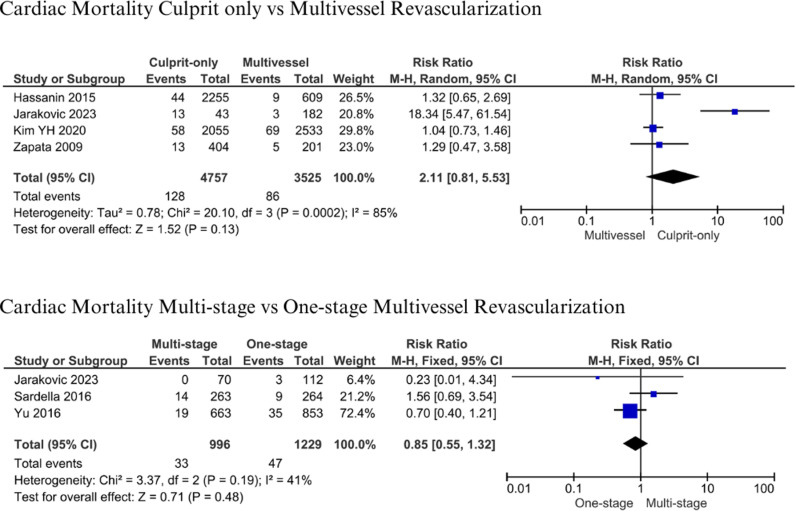 Fig 3
Fig 3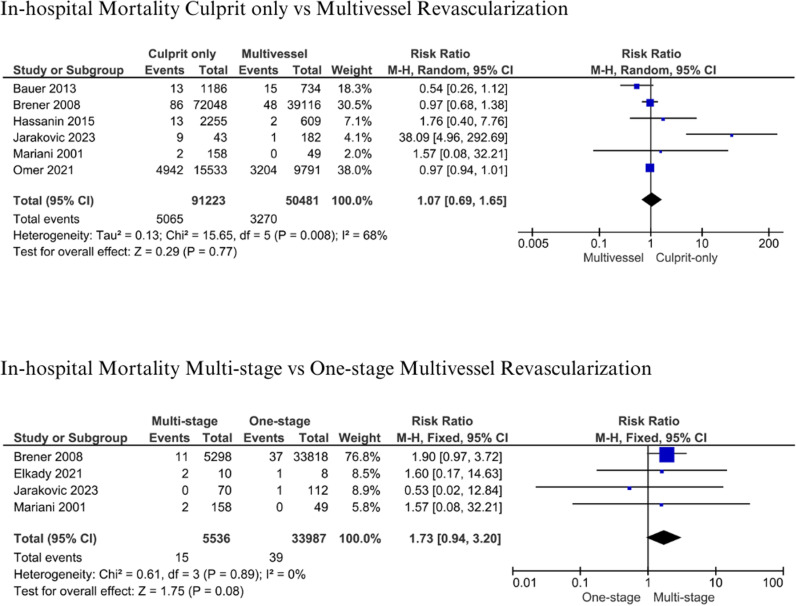 Fig 4
Fig 4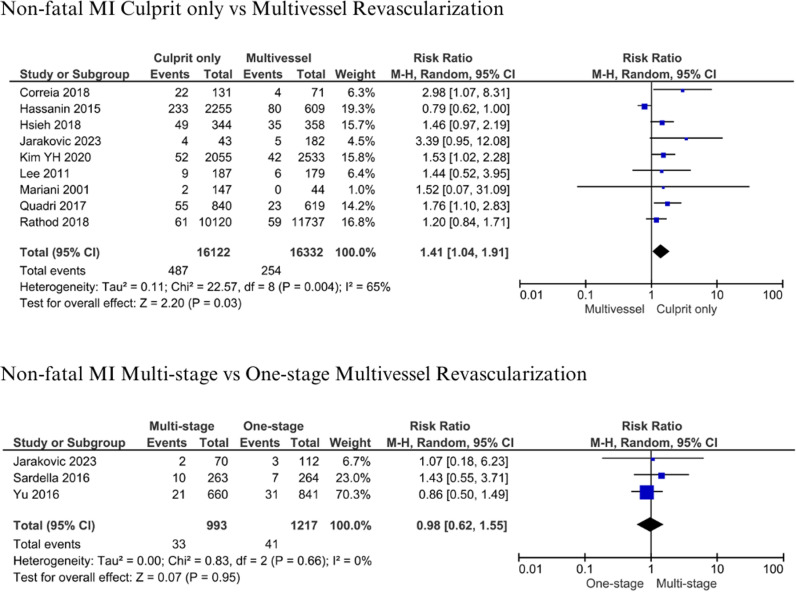 Fig 5
Fig 5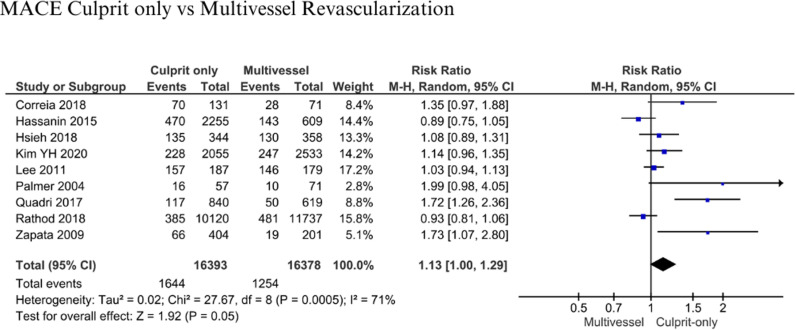 Fig 6
Fig 6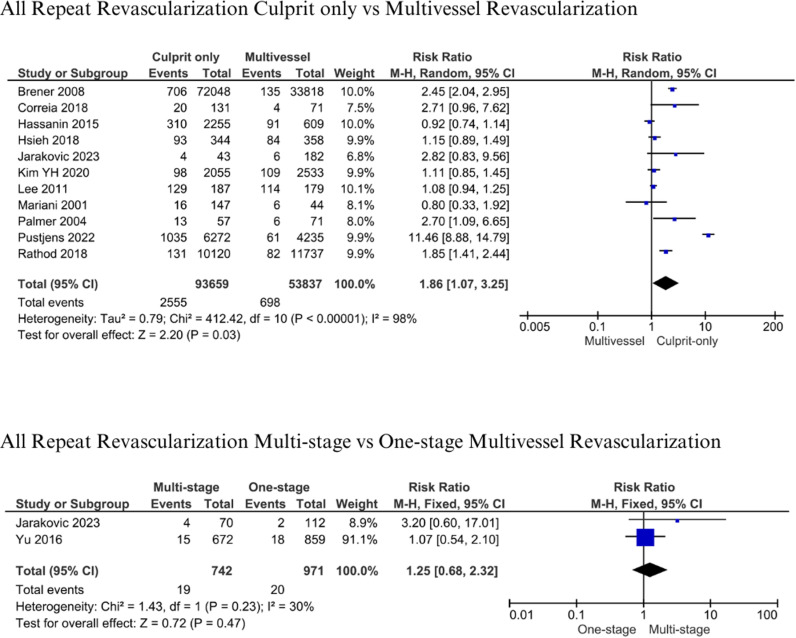 Fig 7
Fig 7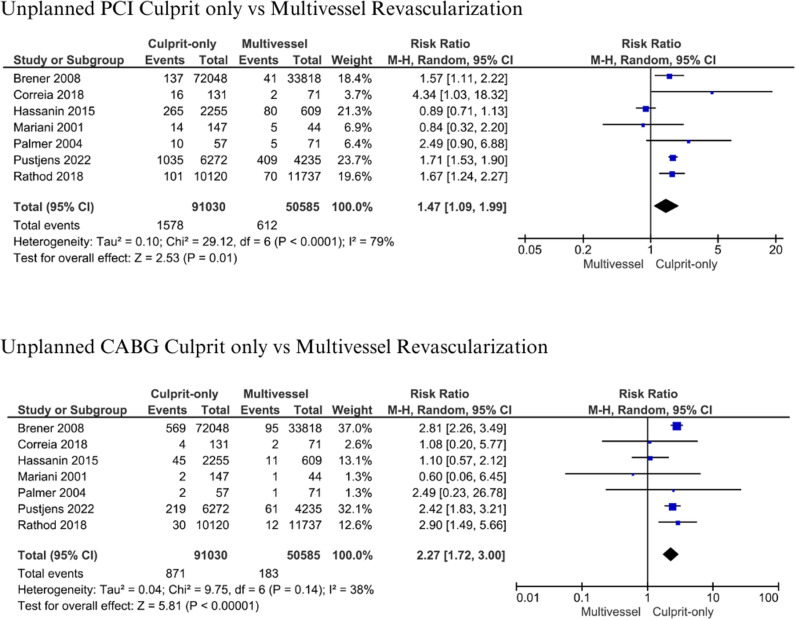 Fig 8
Fig 8 Fig 9
Fig 9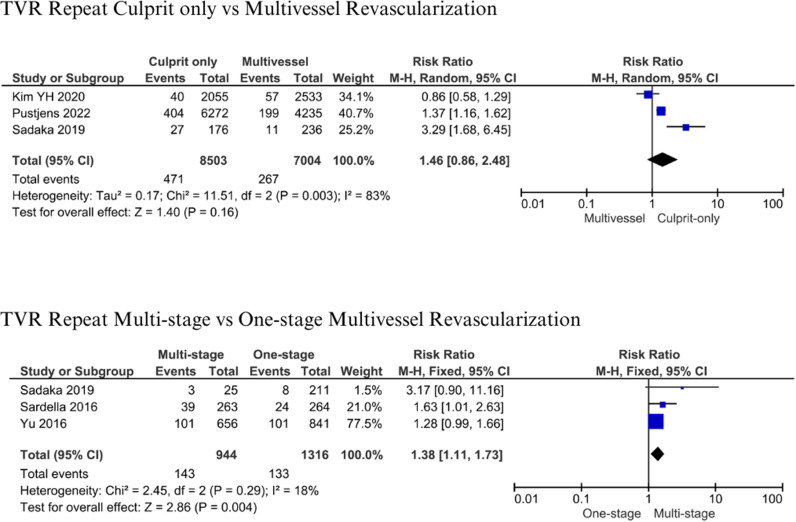 Fig 10
Fig 10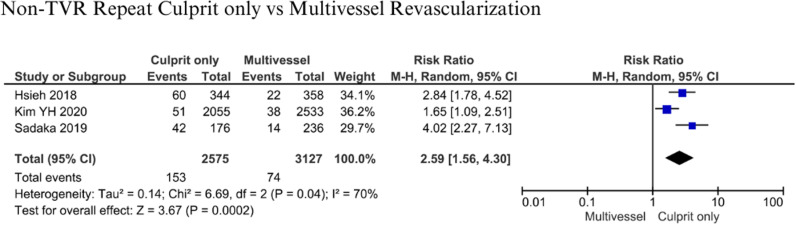 Fig 11
Fig 11Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Acute Myocardial Infarction Research · Cardiac Imaging and Diagnostics
Background
Coronary artery disease (CAD) remains the leading cause of death worldwide. In the US, CAD affects > 18.2 million adults and is a leading cause of death, accounting for > 365,000 deaths annually [1]. Based on the electrocardiogram (ECG), ACS is divided into ST-segment elevation ACS and non-ST-segment elevation ACS, where non-ST segment elevation ACS is divided into NSTEMI and unstable angina [2]. Among 1 million patients admitted to the emergency room due to ACS, 70% of them suggest NSTE-ACS presentation in their ECG examination [3]. Compared to STEMI, NSTEMI patients are exposed to a greater risk of dying after hospital discharge, with 33.2% death rates in two years post-discharge compared to 16.4% in STEMI patients [4].
Revascularization in multivessel NSTE-ACS patients could reduce 24 months of mortality and long-term adverse events compared with medical management only [5]. There is still ongoing debate on how revascularization in multivessel disease should be approached. Multivessel PCI was associated with higher in-hospital mortality rates (30.9 vs 28.4%, p < 0.001) and MACCE (39.9 vs 36.5%, p < 0.001) compared to single PCI [6]. However, complete revascularization in multivessel NSTEMI patients was superior compared to culprit-only in terms of reducing major adverse events and repeat revascularization [7]. The evidence on this topic in multivessel NSTE-ACS remained scarce. This study aims to analyze the outcome of different PCI approaches, between culprit-only and multivessel PCI, or single-stage versus multistage multivessel PCI in NSTE-ACS patients.
Methods
This meta-analysis was conducted in concordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [8] (Table S1**, Supplementary files**). This study was registered in PROSPERO with an identification number (CRD42023442175).
Search strategy
A systematic search was performed in Scopus, Medline, PubMed, ScienceDirect, and Embase on July 4th, 2023. The following search keywords were used: “((unstable angina) OR (non-ST segment acute coronary syndrome) OR (non-ST segment elevation myocardial infarction) OR (NSTEMI) OR (NSTE-ACS)) AND ((revascularization) OR (PCI) OR (percutaneous coronary intervention) OR (stenting) OR (CABG) OR (coronary artery bypass graft surgery)) AND ((MVD) OR (multivessel) OR (multivessel coronary artery disease) OR (multivessel disease)) AND ((culprit-only) OR (target vessel) OR (one-stage) OR (multistage) OR (complete)). Further details of the keyword search are explained in Table S2***, Supplementary files***.
Study selection and inclusion criteria
Studies were searched on databases, compiled, de-duplicated, and screened by three reviewers (JA, AD, and NW). Another reviewer (PS) confirmed the propriety of screened studies in case there was a discrepancy between the first three reviewers. Inclusion criteria are studies in the English language, available in full-text, involving human subjects only, and reporting the mortality of multivessel disease (MVD) NSTE-ACS patients treated with either culprit-only vs multivessel revascularization or one-stage vs multistage multivessel revascularization. Studies involving patients with diagnoses other than NSTEMI and unstable angina were excluded.
Studies were screened by the abstracts and then retrieved for their full text. PRISMA studies selection flowchart is displayed in Fig 1 [8]. Included studies were assessed for their bias risk using The Newcastle-Ottawa Quality Assessment Scale (NOS) for Cohort and Cross-sectional studies and the Cochrane risk-of-bias tool for randomized trials accordingly [9,10].
PRISMA study selection flowchart.
Terms definition
a. Multivessel revascularization is defined as interventions performed on other lesions with different coronary artery territory in addition to culprit lesions [11].b. Culprit-only revascularization is defined as interventions performed only on the culprit lesion, which was identified by Electrocardiography, Angiography, and regional motion abnormality on Echocardiography [12,13].c. One-stage multivessel revascularization is defined as multivessel interventions performed in the same PCI procedure for a culprit lesion during one hospitalization, without additional PCI procedure [14].d. Multistage multivessel revascularization is defined as multivessel interventions performed in different settings with culprit lesions [14–16].e. Non-fatal myocardial infarction is defined as symptoms of cardiac ischemia, elevated troponin above the 99th percentile, elevated creatine kinase-MB, ECG changes such as ST segment changes, new Q waves or new left bundle branch block [14–16].f. All repeat revascularization is defined as any repeat revascularization comprised of TLR, TVR, and non-TVR [7,16–18].g. Target vessel revascularization (TVR) repeat is defined as any repeat revascularization performed on the same previously treated vessel [15,16,18,19].h. Non-TVR repeat is defined as any repeat revascularization performed in different vessels from the target vessel [18].i. Target lesion revascularization (TLR) repeat is defined as any repeat revascularization performed in the same previously treated lesion due to restenosis or re-occlusion [18].
Data extraction and statistical analysis
Data from included studies were extracted, including authors’ names, year of publication, study designs, period of study, study center location, number of patients, age, gender, comorbidities, number of NSTE-ACS, NSTEMI and unstable angina patients, diseased and treated vessel, intervention type, in-hospital mortality, all-cause mortality, cardiac mortality, MACE, non-fatal MI, all-repeat revascularization, TVR repeat, non-TVR repeat, TLR repeat, and follow-up period. Data extraction was performed by JA, AD, and NW, then reviewed by PS in case there was a discrepancy. No missing data was encountered in the primary studies we obtained.
Statistical analysis was performed using Review Manager (version 5.4.1) by author JA. Binary outcomes were analyzed using risk ratio (RR). The pooled RR was assessed using the Mantel-Haenszel method. The heterogeneity of studies was expressed in I^2^. Random effect was used when the heterogeneity was remarkable (I^2^ = 50 – 90%) [20]. Leave-one-out sensitivity analysis was performed to evaluate the impact of each study on the heterogeneity results.
Results
Study selection and quality assessment
A total of 935 articles from five databases were retrieved. After excluding 376 duplicate articles, 505 articles were removed during titles and abstract screening for various reasons in Fig 1. Several studies were excluded after full-text retrieval because they did not specify the outcome of interest [21–24], did not specify the number of NSTE-ACS patients only [25–31], and overlapped populations [32–34]. Three studies were obtained from citation search [35–37]. After a full-text review, 26 studies [7,11–19,35–50] were included in the systematic review. Risk of bias assessment showed that the studies were categorized as good [7,11,12,18,19,35,36,38,45–48,50] and fair [13–17,37,39–44,49] (Table S3 Risk of Bias (Newcastle Ottawa Scale) and Table S4 Risk of Bias (Cochrane Risk of Bias Tools, Supplementary files).
Study characteristics
This study gathered 222,350 NSTE-ACS patients from 26 included studies [7,11–19,35–50]. There were 21 studies included in the meta-analysis [7,11–13,15–19,35–38,41,42,44,45,47–50]. The included studies were conducted from 1979 – 2020. Included studies were comprised of randomized control trials [7,15,37] and cohort studies [11–14,16–19,35,36,38–50].
Most studies took place in the United States (6 studies) [11,14,42,43,46,50], followed by South Korea (2 studies) [18,35], Egypt (2 studies) [12,38], Italy (2 studies) [13,15], and the United Kingdom (2 studies) [45,48]. There were two studies involving multi-centers from several countries [36,37,49]. The characteristics of the included studies were summarized in (Table 1). NSTEMI were found in 132,550 (64.49%) and unstable angina in 72,993 patients (35.51%). Patients presented with variable comorbidities, described in (Table 2). There were 3252 and 1228 patients who received unplanned PCI and CABG, respectively [13,14,19,37,45,47,48]. Types of stents received were bare metal stent (BMS) in 17,891 patients [11,12,15,17,39,41,43,45,50], drug-eluting stents (DES) in 42,227 patients [7,11,12,15,17,39,41,43–45], and both BMS and DES in 6 patients [17] (Table 3). Balloon angioplasty was done in 31 patients [15,41]. The FFR-based approach was conducted on 30 patients [38]. Patients were followed up during their hospital stay up to 4 years post-index procedure.
Table 1: Characteristics of the studies.
Table 2: Patients’ comorbidities.
Table 3: Characteristics of revascularization.
All-Cause Mortality.
The analysis of all-cause mortality between culprit-only and multivessel revascularization included 12 studies [11,13,18,19,35,37,41,44,45,47–49], while multistage and one-stage multivessel revascularization involved two studies [14,15]. Patients were followed up six months – 4 years after the index procedure. Pooled studies gathered 45,739 with culprit-only and 28,449 patients with multivessel intervention. Our analysis yielded insignificant results and high heterogeneity (RR: 0.84; 95% CI: 0.42-1.69; p = 0.62; I^2^: 99%) (Fig 2). There were 9,467 (20.7%) vs 5,172 (18.18%) patients who died with culprit-only compared to multivessel revascularization, respectively. Therefore, there was a relatively 2.52% mortality reduction between both groups. On the other hand, analysis of all-cause mortality comparing multistage and one-stage multivessel revascularization yielded significantly higher mortality in multistage multivessel revascularization compared to one-stage with low heterogeneity (RR: 1.73; 95% CI 1.43-2.10; p < 0.01; I^2^: 0%) (Fig 2). There were 5,561 patients who had multistage and 34,082 others who had one-stage multivessel intervention. Among patients who were multivessel revascularized, 2.68% vs 1.26% of patients died with multistage vs one-stage revascularization.
All-cause mortality for culprit-only vs. multivessel and one-stage vs multistage revascularization.
Cardiac Mortality.
The analysis of cardiac cause mortality of culprit only vs. multivessel revascularization included four studies [17,18,37,41]. Patients were followed up for 1 – 3 years. Included studies pooled 4,757 with culprit-only and 3,525 patients with multivessel revascularization. Studies by Zapata et al., Hassanin et al., and Jarakovic et al. showed higher cardiac mortality in culprit-only compared to multivessel revascularization [17,37,41]. Our analysis yielded no significant differences in cardiac mortality between culprit-only and multivessel revascularization (RR: 2.11; 95% CI: 0.81-5.53; p = 0.13; I^2^: 85%) (Fig 3). There were 996 patients with multistage vs 1,229 patients with one-stage multivessel revascularization. Pooled results demonstrated 128 (2.69%) vs 86 (2.44%) mortality in patients with culprit-only vs multivessel revascularization. Comparison of multistage and one-stage revascularization [15–17] revealed insignificant results (RR: 0.85; 95% CI: 0.55-1.32; p = 0.48; I^2^: 41%) during 1-year follow-up (Fig 3). Patients with one stage died 47 (3.82%) vs 33 (3.31%) compared to multistage revascularization.
Cardiac mortality for culprit-only vs. multivessel and one-stage vs multistage revascularization.
In-hospital Mortality.
A comparison of in-hospital mortality between culprit-only vs. multivessel revascularization [13,14,17,36,37,42] and multistage vs one-stage multivessel revascularization [13,14,17,38] was made. This analysis involved 91,223 patients from culprit-only vs 50,481 patients from multivessel revascularization. Culprit-only and multivessel revascularization demonstrated insignificant in-hospital mortality (RR: 1.07; 95% CI: 0.69-1.65; p = 0.77; I^2^: 68%) (Fig 4). Patients died in the culprit-only group at 5.55% vs 6.48% in the multivessel revascularization group. Analysis of multistage vs. one-stage multivessel revascularization involved 5,536 patients with multistage vs. 33,987 patients with one-stage multivessel intervention. It obtained higher mortality in the multistage group, although the difference is insignificant (RR: 1.73; 95% CI: 0.94-3.20; p = 0.08; I^2^: 0%) (Fig 4). There were 0.27% vs 0.11% patients who died in multistage vs one-stage multivessel revascularization, respectively.
In-hospital mortality for culprit-only vs. multivessel and one-stage vs multistage revascularization.
Non-fatal myocardial infarction.
A total of 16,122 patients with culprit-only and 16,332 patients with multivessel revascularization from 9 studies were evaluated for non-fatal spontaneous MI [7,13,17,18,35,37,45,47,49]. Four additional studies reported non-fatal MI [19,36,44,48]. However, we did not include them in the meta-analysis due to discrepancies in the follow-up period. There were 993 patients with multistage and 1,217 with one-stage multivessel revascularization from 3 studies analyzed and evaluated for non-fatal spontaneous MI [15–17]. Patients were followed up for one year to 4 years. Culprit-only revascularization had significantly higher non-fatal spontaneous MI 487 (3.02%) vs 254 (1.56%), compared to multivessel revascularization (RR: 1.41, 95% CI: 1.04-1.91, p = 0.03, I^2^: 65%) (Fig 5). The analysis of non-fatal spontaneous MI between multistage and one-stage multivessel revascularization showed that there was no significant risk (RR 0.98, 95% CI 0.62-1.55, p = 0.95, I^2^: 99%) (Fig 5). A total of 33 (3.32%) vs 41 (3.37%) patients with multistage vs one-stage multivessel revascularization experienced non-fatal MI.
Non-fatal myocardial infarction for culprit-only vs. multivessel and one-stage vs multistage revascularization.
Major adverse cardiac events (MACE).
There were 16,393 patients with culprit-only and 16,378 patients with multivessel revascularization from 9 studies. Analysis was performed for MACE difference [7,18,35,37,41,45,47–49]. Follow-up period was 1 – 3 years. The analysis showed that there was no significant risk of MACE between culprit only and multivessel revascularization (RR: 1.13, 95% CI: 1.00-1.29, p = 0.05, I^2^: 71%) (Fig 6). Patients with MACE in culprit-only were 1,644 (10.03%) compared to 1,254 (7.66%) in multivessel revascularization.
MACE for culprit-only vs multivessel revascularization.
All Repeat Revascularization.
A total of 93,659 patients with culprit-only and 53,837 with multivessel revascularization from 11 studies were evaluated in the analysis of all repeat revascularization [7,13,14,17–19,35,37,45,47,48]. In comparison, two studies were analyzed for multistage vs one-stage multivessel revascularization with 742 and 971 patients, respectively [16,17]. Follow-up period ranged from hospital stays up to 4 years. The analysis showed that there was a significant risk of all repeat revascularization between culprit only and multivessel revascularization (RR 1.86, 95% CI 1.07-3.25, p = 0.03) (Fig 7). Patients who had culprit-only revascularization had more prevalence in repeat revascularization compared to multivessel revascularization (2.73% vs 1.30%). No statistical differences were found when comparing multistage with one-stage revascularization (RR: 1.25; 95% CI: 0.68-2.32, p = 0.47, I^2^ = 30%) (Fig 7). Multistage patients had more repeat revascularization compared to one-stage multivessel revascularization (2.56% vs 2.06%).
All repeat revascularization for culprit-only vs. multivessel and one-stage vs multistage revascularization.
A total of 1,578 patients (1.73%) with culprit-only vs 612 patients (1.21%) with multivessel revascularization underwent unplanned/emergency PCI, while 871 (0.96%) vs 183 patients (0.36%) underwent unplanned/emergency CABG, in both groups, respectively [13,14,19,37,45,47,48]. Both unplanned PCI and CABG in the culprit-only group were significantly higher (RR: 1.47; 95% CI: 1.09-1.99, p = 0.01, I^2^ = 79%) and (RR: 2.27; 95% CI: 1.72-3.00, p < 0.001, I^2^ = 38%) (Fig 8).
Unplanned PCI and CABG for culprit-only vs multivessel revascularization.
TLR Repeat.
Three studies involved 5,702 patients in the analysis of TLR repeat [7,12,18]. Patients were followed up for six months to 3 years. Statistical analysis (RR: 2.04; 95% CI 1.21-3.43, p = 0.008; I^2^: 64%) (Fig 9) indicated that patients who had culprit-only revascularization were at about two times higher risk for TLR repeat compared to patients with multivessel revascularization.
Target lesion revascularization repeat for culprit-only vs multivessel revascularization.
TVR Repeat.
A total of 15,507 patients from 3 studies were evaluated in the analysis of TVR Repeat between culprit-only and multivessel revascularization [12,18,19]. No difference was found between culprit-only and multivessel revascularization about TVR repeat (RR: 1.46; 95% CI 0.86-2.48, p = 0.16; I^2^: 83%) (Fig 10). Three studies involving 2,260 patients were evaluated between multistage and one-stage multivessel revascularization [12,15,16]. TLR repeat was significantly 1.3 times increased by multistage revascularization compared with one-stage revascularization (RR 1.38; 95% CI 1.11-1.73; p = 0.004, I^2^: 18%) (Fig 10).
Target vessel revascularization repeat for culprit-only vs multivessel and one-stage vs multistage revascularization.
Non-TVR Repeat.
Three studies involving 5,702 patients were analyzed for non-TVR repeat [7,12,18]. The statistical analysis indicated that the patients who received culprit-only revascularization had about 2.59 times the risk for having non-TVR repeat compared to patients who received Multivessel revascularization (RR 2.59; 95% CI 1,56-4.30; p = 0.0002; I^2^: 70%) (Fig 11).
Non-target vessel revascularization repeat for culprit-only vs multivessel revascularization.
Discussion
There was still an ongoing debate on whether lesions in MVD NSTE-ACS should be treated immediately or staged, culprit lesion only or complete, as the evidence from previous studies remained scarce. It is surprising, as half of the acute coronary syndrome patients have MVD [51,52], but the evidence is limited.
Our study indicated an insignificant difference in mortality between culprit-only and multivessel revascularization, based on all-cause, cardiac, and in-hospital mortality. It is similar to the study by Atti et al. in a meta-analysis of multivessel disease (MVD) STEMI patients comparing culprit-only and multivessel revascularization [20]. Additionally, culprit-only revascularization has significantly higher non-fatal spontaneous MI compared to multivessel revascularization. There was a 41% increase in non-fatal MI in CO compared to the MV group, in line with previous studies which reported that multivessel revascularization decreased the risk of non-fatal myocardial infarction complications [53]. Another meta-analysis also stated that the incidence of non-fatal myocardial infarction was less frequent with multivessel PCI (HR 0.64, 95% CI 0.52-0.79; p = 0.001) [54]. This occurrence is perhaps due to a pre-existing non-culprit lesion that did not undergo intervention, then progressed and caused re-infarction later after index PCI [55]. This process could be prevented by multivessel revascularization. Data from SWEDEHEART revealed that previously unstented lesions bear twice the risk of re-infarction than stented lesions [55]. Non-culprit lesions may be unstable and have similar morphology as culprit lesions [56,57]. Thus, it may benefit from stenting.
On the other hand, a significant increase in all-cause mortality was found in multistage (MS) compared to one-stage (OS) multivessel revascularization. There was a 58% increase in mortality of MS compared to OS revascularization. MS revascularization showed less favorable outcomes, probably due to prolonged procedure duration, higher contrast volume used, and longer myocardial ischemia duration [18]. Additionally, a higher incidence of MACE was also found in multistage multivessel revascularization [18], which supports the complications and contributes to the all-cause mortality incidence.
Our study showed a significant difference in the incidence of repeat revascularization between the MV and CO groups. There was an 86% increase in all repeat revascularization, 47% increase in unplanned PCI, 127% increase in unplanned CABG, 104% increase in TLR repeat, and 159% increase in non-TVR repeat with CO compared to the MV group. A study by Lee et al. revealed that MV reduced the incidence of revascularization after three years of follow-up compared to CO [35]. A study by Pustjens revealed that there was a reduced incidence of re-intervention in patients undergoing MV. These results were persistent when all revascularization electives within three months were excluded (10.2% in the MV-PCI vs. 16.2% in the CO-PCI group; p < 0.001) [19]. These results are in line with those reported in studies such as SMILE Trial by Sardella et al. (2016) [15] and by Tamburino et al. (2008) [58], van den Brand et al. (2002) [59], Bourassa (1998) [29], Ijsselmuiden et al. (2004) [60] and Nikolsky et al., (2004) [61]. Potential advantages of MV compared to CO are reduction of the myocardial area at risk and improvement of myocardial function by increasing blood flow to the peri-infarction area [47]. While culprit-only intervention could improve blood flow on the culprit lesion, other lesions remained intact and progressed over time. Residual coronary plaque lesions create a turbulent flow and reduce shear stress in the surrounding area, which induces plaque formation [62] and leads to repeat revascularization. Therefore, multivessel revascularization offers more benefits than culprit-only.
The limitation of our study is the lack of a trial study as a reference because the currently available studies remain scarce. Differences in the follow-up time between studies were present. Patients with cardiogenic shock were included in the studies. The first and second generations of drug-eluting stents were used in several studies, while the other only used newer generations. Inherent bias is commonly found in the meta-analysis.
NSTEMI patients dominated the population of this study and this is in line with data from large registry [63]. More importantly, whether NSTE-ACS presents with unstable angina or NSTEMI, they prompt similar management based on the current European Society of Cardiology (ESC) guidelines [64]. Therefore, the outcomes of our study are considered representative and relevant with entire NSTE-ACS population. Although BMS were still used in several studies despite the advancement of DES, real-world data demonstrated that BMS remained as the main modality in the intervention [65,66], especially in the developing countries [12,17,39,41]. Thus, the outcomes of this study are relevant with current practice of revascularization.
Conclusion
This study found a more favorable outcome of multivessel compared to culprit-only revascularization. Single-staged multivessel intervention may be more beneficial than multi-staged. Careful considerations in deciding which interventions to use are important in ensuring the optimal outcome for the patients. Further studies on the current topic are encouraged.
Supporting information
S1 tablePRISMA checklist.(DOCX)
S2 tablesearch strategy.(DOCX)
S3 tableRisk of Bias (Newcastle Ottawa Scale).(DOCX)
S4 tableRisk of Bias (Cochrane Risk of Bias Tools).(DOCX)
S5 tableRaw data.(XLSX)
S6Funnel plot of the analysis.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;144(22):e 368–454. doi: 10.1161/CIR.0000000000001029 34709879 · doi ↗ · pubmed ↗
- 2Collet J-P, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289–367. doi: 10.1093/eurheartj/ehaa 575 32860058 · doi ↗ · pubmed ↗
- 3Bob-Manuel T, Ifedili I, Reed G, Ibebuogu U, Khouzam R. Non-ST elevation acute coronary syndromes: A comprehensive review. Current Problems in Cardiology. 2017;42(9):266–305.28764841 10.1016/j.cpcardiol.2017.04.006 · doi ↗ · pubmed ↗
- 4Darling CE, Fisher KA, Mc Manus DD, Coles AH, Spencer FA, Gore JM, et al. Survival after hospital discharge for ST-segment elevation and non-ST-segment elevation acute myocardial infarction: a population-based study. Clin Epidemiol. 2013;5229–36. doi: 10.2147/CLEP.S 45646 23901296 PMC 3724561 · doi ↗ · pubmed ↗
- 5Desperak P, Hawranek M, Gąsior P, Desperak A, Lekston A, Gąsior M. Long-term outcomes of patients with multivessel coronary artery disease presenting non-ST-segment elevation acute coronary syndromes. Cardiol J. 2019;26(2):157–68. doi: 10.5603/CJ.a 2017.0110 28980282 PMC 8086658 · doi ↗ · pubmed ↗
- 6Wu J, Wang Y, Li C, Ji H, Zhao W, Tong Q, et al. Multivessel vs. culprit vessel-only percutaneous coronary intervention in ST-segment elevation myocardial infarction with and without cardiogenic shock. Front Cardiovasc Med. 2022;9:992456. doi: 10.3389/fcvm.2022.992456 36505378 PMC 9731335 · doi ↗ · pubmed ↗
- 7Hsieh M, Chen C, Lee C, Wang C, Chang S, Chen D. Complete and incomplete revascularization in non-ST segment myocardial infarction with multivessel disease: long-term outcomes of first- and second-generation drug-eluting stents. Heart and Vessels. 2019;34(2):251–8.30159655 10.1007/s 00380-018-1252-z · doi ↗ · pubmed ↗
- 8Page M, Mc Kenzie J, Bossuyt P, Boutron I, Hoffmann T, Mulrow C. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372(n 71):.10.1136/bmj.n 71PMC 800592433782057 · doi ↗ · pubmed ↗