Health before pregnancy and eligibility for parental leave benefits: a Swedish total population cohort study
Amy Heshmati, Andrea Dunlavy, Eleonora Mussino, Sara Fritzell, Sol P. Juárez

TL;DR
This study finds that mothers with poor health before pregnancy are less likely to qualify for generous parental leave benefits in Sweden due to strict work requirements.
Contribution
The study empirically shows how work requirements for parental leave benefits may worsen health inequalities among mothers.
Findings
Mothers with prior health issues, especially mental disorders, are significantly less likely to be eligible for earnings-related parental leave benefits.
The association is stronger for those with chronic health conditions and for Swedish-born mothers.
Strict work requirements for parental leave benefits may exacerbate socioeconomic inequalities in maternal mental health.
Abstract
Parental leave generosity is protective for mothers’ mental health in the postpartum period and beyond. Strong work requirements exist for parents in Sweden to receive more generous benefits which might penalise individuals who, due to poor health, have a weak labour market attachment. The aim of the study was to examine whether mothers with poor health prior to pregnancy are less likely to be eligible for more generous benefits in Sweden. We used total population registers to study first-time mothers, aged 25–45 years, who were resident in Sweden and gave birth between 1 January 2009 and 30 September 2013 (n = 151,452). We used logistic regression to examine the association between health one and two consecutive years prior to pregnancy (to assess chronicity) and eligibility for earnings-related parental leave benefits. Mothers who were admitted to hospital or received specialist…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1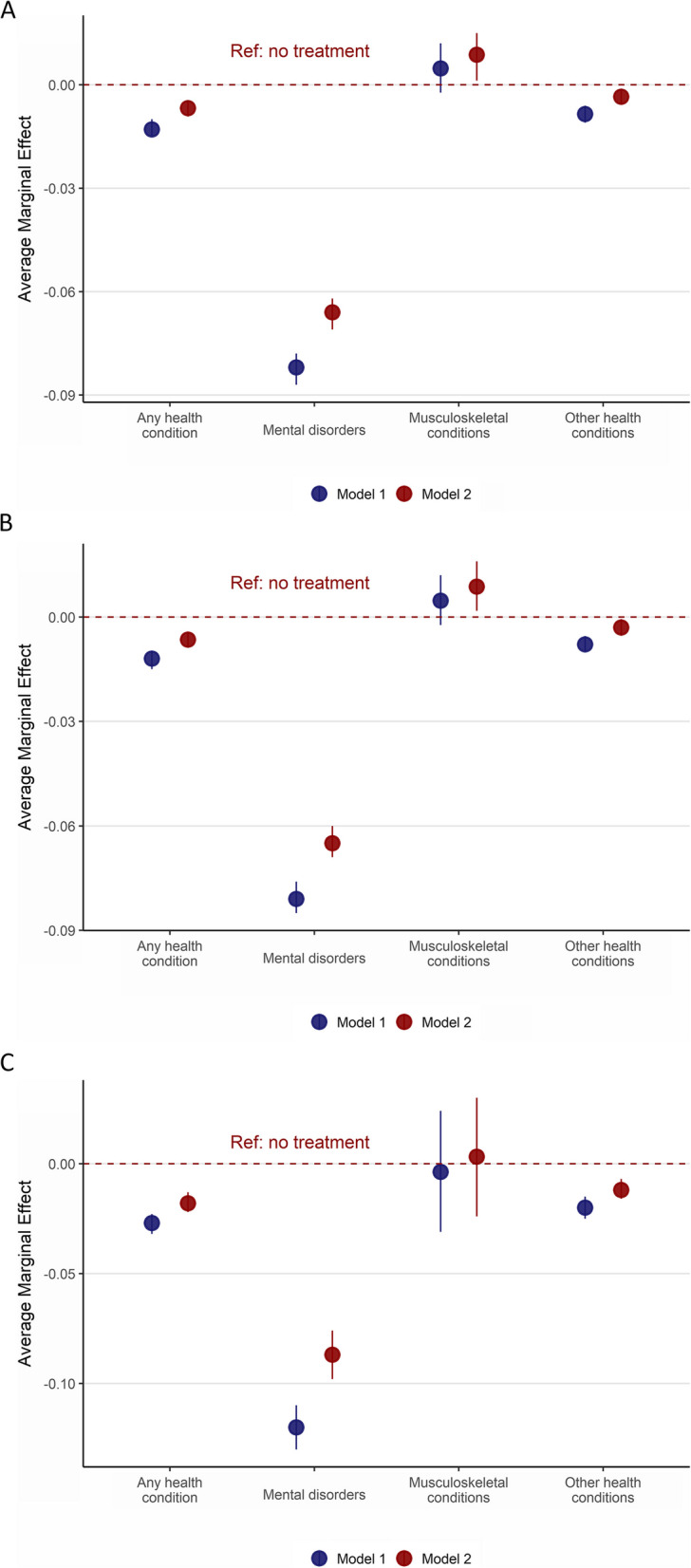 Figure 2
Figure 2- —The Swedish Research Council for Health, Working Life and Welfare (FORTE)
- —Stockholm University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEmployment and Welfare Studies · Global Health Care Issues · Health disparities and outcomes
Introduction
The parental leave scheme in Sweden is considered one of the most generous and flexible in the world, where all registered residents have access to 480 days of paid parental leave per child until the child turns twelve years old or has completed grade five of compulsory education (Table 1 displays an overview of Sweden’s parental leave scheme) [1]. However, remuneration amounts are dependent on the individual’s income and participation in the labour market. Today, to obtain the most generous earnings-related parental leave benefit, a person must be employed for at least 240 consecutive days prior to the estimated delivery date and have a minimum annual income of 85 000 SEK (GBP 6330). Parents who meet this criterion receive almost 80% of their salary for 390 days with the remaining 90 days compensated at a minimum level (180 SEK/day; GBP 13·40/day) [1]. Many employees receive an additional ten percent supplement from their employers via collective agreement [2]. In contrast, parents who are outside the labour market or who have an income below the threshold for earnings-related parental leave benefits receive a basic pre-tax benefit of 7500 SEK (GBP 560) per month for 390 days and then the minimum level benefit thereafter [1]. Table 1. Overview of the paid parental leave in Sweden [1]Parental leave(Swedish: föraldraledighet)Parents in employment are entitled to job-protected leave of absence until the child reaches 18 months of ageParental allowance(Swedish: föraldrapenning)Parental allowance is paid for 480 days for a child. For 390 days, the compensation is based on the parent’s income (earnings-related benefit) and for the other 90 days, the compensation is a minimum-level benefit (180 SEK per day)The first 180 days taken out for the child must be days at earnings-related level. When you have taken out 180 days at the earnings-related level, you can start taking out days at the minimum-level as wellParents with joint custody are automatically assigned half of the parental leave benefit period (i.e., 240 days each), but days can be transferred to the other parent. From 2002, 60 days were reserved for each parent (often referred to as the ‘mother’ or ‘fathers’ quota). From 2016 until present, 90 days are reserved for each parent which cannot be transferredEligibility to parental allowanceAll parents who are resident in Sweden are entitled to receive parental allowance if:• Taking care of a child• Not working, looking for employment or studying• The child lives in Sweden, in another country within the EU/EEA, or in Switzerland• The parent is insured in SwedenRemunerationThe parental leave allowance is dependent on the parent’s income and length of employment prior to expected delivery dateCompensation based on income (390 days)• If you have worked for at least 240 consecutive days prior to the expected birth and met an annual income threshold, then parents receive 77.6% of their salary for 390 days (earnings-related benefits)• If parents have not worked for at least 240 consecutive days before the expected birth, then they receive a basic flat-rate benefit for 390 days (basic benefit). From 2004, the basic benefit was set at 180 SEK per day, this was increased in 2013 to 225 SEK per day, and in 2016 it was further increased to 250 SEK per day where it currently standsMinimum level benefit (Swedish: lägstanivå) (90 days)From 2006, the minimum-level benefit is 180 SEK per day and has remained at this rate sinceFlexibilityFor children born before 1 January 2014, parents could withdraw parental allowance until the child turned 8 years of age or completed Grade 1 of primary educationFor children born from 1 January 2014, parents can withdraw parental allowance up to and including the day the child turns 12 years of age or until they have completed grade 5 of primary education. However, from the child’s fourth birthday only 96 days can be usedResponsibilityThe Ministry of Social Affairs has the responsibility over the parental benefit, and the Ministry of Employment has the responsibility over the legislated right to leave from workFunderThe Swedish Social Insurance Agency (Swedish: Försäkringskassan)Formal childcare outside the homeIn Sweden, children are entitled to attend preschool (Swedish: förskola) once they have turned one year old. As a result, the responsibility for childcare during the child’s first year falls on the parents. The flexibility of the parental leave policy allows parents to use their leave as best suited to their family needsAbbreviations: EEA European Economic Area, EU European Union
A recent systematic review of the international literature concluded that parental leave generosity, in terms of remuneration and duration, is protective for mothers’ mental health in the postpartum period and beyond, including mothers with mental health conditions prior to pregnancy [3]. However, the review also suggested that work requirements (e.g., continuous employment for a fixed period of time prior to childbirth, meeting an annual income threshold) as a pre-requisite for more generous parental leave entitlements could be inadvertently responsible for increasing health inequalities in society, yet there is a lack of empirical evidence. Postpartum health inequalities can arise because certain groups, including those with ill-health [4] and migrants [5, 6], may also have weaker labour market attachment, and thus are less likely to benefit from the protective health effects of parental leave.
Although any health issue can potentially affect an individual’s capacity for employment, mental disorders and musculoskeletal conditions are the most common reasons for sickness absence in Sweden and elsewhere [7, 8]. In Sweden, among women of childbearing age, mental disorders account for approximately 60% of all work absenteeism cases, while the prevalence of absenteeism due to musculoskeletal conditions ranges from eight percent among women under 40 years of age to 13% in those aged 40–49 years [9]. Therefore, it is postulated that women who have suffered from these conditions may, in turn, be less likely to qualify for more generous parental leave entitlements due to weaker labour market attachment.
The aim of this study was to investigate the association between poor health in mothers prior to pregnancy and their eligibility for earnings-related parental leave benefits in Sweden in order to shed light on the extent to which the qualifying work requirement may act as a barrier for more generous parental leave benefits for mothers with pre-existing or chronic health conditions.
Methods
This total population cohort study was performed as part of a larger project on the Unintended consequences of the Swedish Parental Leave Policy (ParLeHealth): A health equity perspectivewith a published peer-reviewed protocol [10].
Data sources and study population
We used data from Swedish national registers that were linked using pseudonymised unique identification numbers. These registers included the Total Population Register, the Multi-Generation Register, and the Medical Birth Register, to construct our study population and identify first-time mothers; the National Patient Register, for information on hospitalisation and specialist outpatient care; the Swedish Social Insurance Agency (Försäkringskassan), for data on compensation level for parental leave remuneration benefits; the Longitudinal Integrated Database for Health Insurance and Labour Market Studies (LISA), for socioeconomic information, and the Geography Database for data on urbanicity.
The study population included all first-time mothers who gave birth in Sweden between 2009 and 2013, and who were resident in the country three years prior to pregnancy (n = 225 906). We restricted our population to mothers aged between 25 and 45 years to ensure adequate time in the labour market (n = 172 687), and excluded mothers whose child(ren) were born between October and December 2013 due to a reporting system change at the Swedish Social Insurance Agency (n = 11 135). We also excluded 10 100 mothers because of missing data. The final analytic sample consisted of 151 452 mothers (Fig. 1).Fig. 1. Study selection
The study was approved by the Swedish Ethical Review Authority (2019–04913).
Exposures
Using the 10th edition of the International Classification of Diseases (ICD) codes, our exposures included assessment of four health categories: any health condition (all ICD chapters excluding external causes for morbidity and mortality: V01-Y98); mental disorders (F00-F99); musculoskeletal conditions (M00-M99); and other health conditions (excluding mental disorders and musculoskeletal conditions). These health categories were assessed across two levels of healthcare use representing different levels of severity: hospitalisation; and specialist outpatient care (hereinafter outpatient care) as well as a combined category: hospitalisation or specialist outpatient care (hereinafter any healthcare treatment). A complete list of all ICD-10 codes and their definition are in Table A1 (Appendix 1). Exposures were dichotomous (e.g., any health condition versus none) and measured in the year (365 days) prior to pregnancy. In separate analyses, a proxy measure was used to assess the presence of chronic conditions by examining healthcare utilisation for two consecutive years before pregnancy. Health conditions were identified by primary diagnosis to focus on the principal health issue, thereby avoiding confounding with secondary conditions. Using primary diagnoses ensures that the population is selected based on consistent criteria, enhancing comparability across studies and improving replicability.
Outcome
We assessed eligibility for earnings-related parental leave benefits using the compensation level variable for parental leave remuneration determined by the Swedish Social Insurance Agency when the mother applied for parental level benefits for the first time after childbirth. Eligibility was categorised into two groups: recipients of earnings-related benefit payments (generous) and recipients of basic flat-rate payments (basic), i.e., those who were not eligible for earnings-related benefits.
Socio-demographic variables
We obtained birth year of the child and mother’s age at the time of birth, measured continuously in completed years, from the Medical Birth Register. Using data from the Total Population Register, we classified mothers based on their region of birth into three groups: 1) from Sweden, 2) from regions primarily composed of Organisation for Economic Cooperation and Development (OECD) member countries including the Nordic region (excluding Sweden), Europe, North America and Oceania, and 3) from non-OECD regions primarily comprising of mothers from Africa, Middle East, Asia, South America, or stateless/unspecified regions [11]. Our socio-economic measure was highest level of education attained by the mother at approximately two years prior to pregnancy. Mother’s educational level was categorised as low (compulsory schooling: up to nine years of education), medium (upper-secondary schooling: up to 12 years of education), and high (any tertiary education).
Statistical analysis
All analyses were performed using Stata v17 [12]. Logistic regression models were used to calculate odd ratios (OR) and 95% Confidence Intervals (95% CI). Health prior to pregnancy was assessed in separate analyses, and were specific for each health complaint, whereby those without that specific health issue were included in the comparison group. All analyses adjusted for birth year of the child to account for cohort effects, and mother’s age at birth (Model 1). We further adjusted for mother’s education (Model 2), in order to ascertain if potential differences in the main association were explained by education. Furthermore, we performed stratified subgroup analyses by mother’s region of birth to ascertain if potential differences in the main effect were driven by birthplace. In addition to odds ratios, we also estimated average marginal effects (AME) for these analyses. In Sweden, the health care system is universal, primarily government funded, decentralised, and managed by regions, local authorities or municipalities. Therefore, we do not expect area of residence (urbanicity) to substantially influence access to healthcare. However, we conducted sensitivity analyses to test this assumption (see Appendix 2 for description and operationalisation of this variable). As hospitalisation and outpatient care variables were not mutually exclusive, and may have overlapped, we also performed sensitivity analyses excluding mothers who were hospitalised i.e., those with more severe illness, from the outpatient care variable.
Results
The mean age of mothers at the time of birth was 30·5 years (SD 3·9) (Table 2). The majority (94·2%) were eligible for earnings-related parental leave benefits, born in Sweden (88·2%) and highly educated (62·6%). Mothers with low level of education attainment (74·4%) had lower eligibility for earnings-related benefits. The proportion of mothers eligible for earnings-related benefits was highest among Swedish-born mothers (95%), and lowest among mothers from non-OECD regions (80%). The prevalence of any health conditions was lowest among Swedish-born mothers (41%), and ranged from 43% for mothers from OECD regions to 47% for mothers from non-OECD regions. Table 2. Characteristics of the study population (N = 151 452)Eligible for earning’s-related parental leave benefits****N (SD)Range/%N%p-valueMother’s age at birth (years)30·5 (3·94)25–45Birth year of the child 200931 83421·0230 03694·35 201032 90921·7330 96194·08 201131 58120·8529 71594·09 201231 90321·0630 07994·28 201323 22515·3321 85494·10p = 0·45Educational level Low6 7424·455 01574·38 Medium49 98433·0046 44492·92 High94 72662·5591 18696·26p < 0·001Region of birth Sweden133 52788·16127 49495·48 Migrant from OECD8 4515·587 59289·84 Migrant from Non-OECD9 4746·267 55979·79p < 0·001Eligible for earnings related benefits Eligible to earnings-related benefits142 64594·18 Not eligible to earnings-related benefits8 8075·83Health in year prior to pregnancyAny health condition Any healthcare treatment63 39841·8659 34393·60 No healthcare treatment88 05458·1483 30294·60p < 0·001 Specialist outpatient care62 21641·0858 24893·62 No specialist outpatient care89 23658·9284 39794·58p < 0·001 Hospitalisation8 0955·347 38491·22 No hospitalisation143 35794·6135 26194·35p < 0·001Mental disorder Any healthcare treatment3 8282·533 02979·13 No healthcare treatment147 6297·47139 61694·58p < 0·001 Specialist outpatient care3 6872·432 93879·69 No specialist outpatient care147 76597·57139 70794·55p < 0·001 Hospitalisation4570·3029764·99 No hospitalisation150 99599·70142 34894·27p < 0·001Musculoskeletal condition Any healthcare treatment4 8883·234 63394·78 No healthcare treatment146 56496·77138 01294·17p = 0·07 Specialist outpatient care4 8143·184 56394·79 No specialist outpatient care146 63896·82138 08294·17p = 0·07 Hospitalisation2720·1825694·12 No hospitalisation151 18099·82142 38994·19p = 0·96Other health conditions Any healthcare treatment59 89139·5456 19593·83 No healthcare treatment91 56160·4686 45094·42p < 0·001 Specialist outpatient care58 65838·7355 05993·86 No specialist outpatient care92 79461·2787 58694·39p < 0·001 Hospitalisation7 5214·976 93592·21 No hospitalisation143 93195·03135 71094·29p < 0·001Health two years prior to pregnancy (chronic healthAny health condition Any healthcare treatment33 42722·0730 88692·40 No healthcare treatment118 02577·93111 75994·69p < 0·001 Specialist outpatient care32 52721·4830 08692·5 No specialist outpatient care118 92578·52112 55994·65p < 0·001 Hospitalisation1 0800·7189783·06 No hospitalisation150 37299·29141 74894·26p < 0·001Mental disorder Any healthcare treatment1 9291·271 42673·92 No healthcare treatment149 52398·73141 21994·45p < 0·001 Specialist outpatient care1 8431·221 37274·44 No specialist outpatient care149 60998·78141 27394·43p < 0·001 Hospitalisation1170·085748·72 No hospitalisation151 33599·92142 58894·22p < 0·001Musculoskeletal condition Any healthcare treatment1 5501·021 45693·94 No healthcare treatment149 90298·98141 18994·19p = 0·67 Specialist outpatient care1 5081·001 41793·97 No specialist outpatient care149 94499·00141 22894·19p = 0·71 Hospitalisation290·022689·66 No hospitalisation151 42399·98142 61994·19p = 0·30Other health conditions Any healthcare treatment29 78019·6627 69392·99 No healthcare treatment121 67280·34114 95294·48p < 0·001 Specialist outpatient care28 88319·0726 89093·10 No specialist outpatient care122 56980·93115 75594·44p < 0·001 Hospitalisation8630·5775086·91 No hospitalisation150 58999·43141 89594·23p < 0·001Household income and educational level measured approximately two years prior to pregnancy
Mothers receiving any healthcare treatment for any health condition in the year before pregnancy had lower odds of being eligible for earnings-related benefits (OR 0·79, 95%CI 0·76–0·83; Model 1) compared to mothers with no healthcare treatment (Table 3). The estimate was similar for mothers receiving outpatient care (OR 0·80, 95%CI 0·77–0·84; Model 1). However, mothers hospitalised for any health condition had even lower odds of being eligible for earnings-related benefits compared to mothers who were not hospitalised for any health condition (OR 0·60, 95% CI 0·56–0·65; Model 1). Mothers who received any healthcare treatment for mental disorders in the year preceding pregnancy had significantly decreased odds of being eligible for earnings-related benefits compared with mothers who did not receive treatment for mental disorders (OR 0·22, 95%CI 0·20–0·23; Model 1). Mothers admitted to hospital for mental disorders had even lower odds for eligibility for earnings-related benefits compared to mothers who were not hospitalised for mental disorders (OR 0·12, 95% CI 0·10–0·14; Model 1). Moreover, mothers receiving outpatient care or hospitalised for other health conditions also demonstrated significantly lower odds of being eligible for earnings-related benefits compared with healthy mothers (OR 0·87, 95%CI 0·83–0·90 for outpatient care (Model 1); OR 0·70, 95%CI 0·64–0·76 for hospitalisation (Model 1)). In contrast, there was no evidence of an association between receiving any healthcare treatment for musculoskeletal conditions in the year prior to pregnancy and being eligible for earnings-related parental leave benefits (OR 1·09, 95%CI 0·96–1·24; Model 1) (Table 3). Figure 2 and Table 3(Appendix 3) displays the average marginal effects in the association between health prior to pregnancy and eligibility for earnings-related parental leave benefits to facilitate comparison with odd ratio estimates. Table 3. The association between any health condition; mental disorders; musculoskeletal conditions; and other health conditions; and eligibility for earnings-related parental leave benefits (N = 151 452)Health in the year prior to pregnancyHealth in the two consecutive years prior to pregnancy (chronic health) **Any healthcare treatmentSpecialist outpatient CareHospitalisationAny healthcare treatmentSpecialist outpatient CareHospitalisationModel 1****OR (95% CI)Model 2OR (95% CI)Model 1OR (95% CI)Model 2OR (95% CI)Model 1OR (95% CI)Model 2OR (95% CI)Model 1OR (95% CI)Model 2OR (95% CI)Model 1OR (95% CI)Model 2OR (95% CI)Model 1OR (95% CI)Model 2OR (95% CI)**No health condition111111111111Any health condition0·79(0·76–0·83) ***0·88(0·84–0·92) ***0·80(0·77–0·84) ***0·88(0·85–0·92) ***0·60(0·56–0·65) ***0·71(0·66–0·77) ***0·64(0·62–0·68) ***0·74(0·71–0·78) ***0·66(0·63–0·69) ***0·76(0·72–0·80) ***0·29(0·25–0·34) ***0·41(0·35–0·49) ***No mental disorders111111111111Any mental disorders0·22(0·20–0·23) ***0·28(0·26–0·31) ***0·22(0·21–0·24) ***0·29(0·26–0·32) ***0·12(0·10–0·14) ***0·19(0·15–0·23) ***0·16(0·15–0·18) ***0·22(0·20–0·25) ***0·17(0·15–0·19) ***0·22(0·20–0·25) ***0·06(0·04–0·09) ***0·11(0·08–0·17) ***No musculoskeletal condition1111111111§§Any musculoskeletal condition1·09(0·96–1·24)1·18(1·03–1·34) *1·09(0·96–1·24)1·18(1·04–1·35) *0·93(0·56–1·55)1·06(0·63–1·78)0·91(0·74–1·13)0·99(0·80–1·23)0·92(0·74–1·14)0·99(0·80–1·23)No other health condition111111111111Any other health condition0·86(0·82–0–89) ***0·94(0·89–0·98) **0·87(0·83–0·90) ***0·94(0·90–0·99) *0·70(0·64–0·76) ***0·80(0·73–0·88) ***0·74(0·70–0·77) ***0·83(0·79–0·88) ***0·75(0·71 −0·79) ***0·85(0·81–0·90) *0·40(0·32–0·48) 0·53(0·43–0·65) Model 1: Adjusted for child’s year of birth, mother’s ageModel 2: Adjusted for child’s year of birth, mother’s age, educationOR Odds ratio, 95%CI 95% confidence intervals^§^Not enough units in cell to perform analysis for hospitalization^^p < 0·05^^p < 0·01^^p < 0·001Fig. 2The average marginal effects with 95% confidence intervals of logistic regression exploring the association between any health condition; mental disorders; musculoskeletal conditions; and other health conditions; and eligibility for earnings-related parental leave benefits in the year prior to pregnancy (N = 151 452). A: Any healthcare treatment, B: Outpatient care, and C: Hospitalisation
The inclusion of education in the models largely did not influence the pattern of associations, with the exception of musculoskeletal conditions. Mothers who received outpatient care for such conditions were more likely to be eligible for earnings-related benefits (OR 1.18, 95%CI 1.03–1.34; Model 2) (Table 3).
Moreover, the odds of being eligible for earnings-related parental leave benefits were further reduced among mothers receiving healthcare treatment for any health condition, mental disorders, or other health conditions in both of the two consecutive years prior to pregnancy, compared to mothers who did not receive any healthcare treatment during those years. This was particularly apparent among mothers who received healthcare treatment for mental disorders (OR 0·16, 95%CI 0·15–0·18; Model 1). Odds ratio estimates were reduced further among those who were hospitalised for mental disorders (OR 0·06 95%CI 0·04–0·09; Model 1). When analyses were further adjusted by education, similar patterns remained (Table 3).
Sub-analyses
Receiving healthcare treatment for any and other health conditions differed by region of origin (Table 4). The proportion of mothers receiving outpatient care and being admitted to hospital was lowest among Swedish born mothers (41·38% and 38·19%), followed by mothers from OECD regions (43·32% and 41·52%), and mothers from non-OECD regions (47·26% and 45·26%), for any and other health conditions, respectively. In contrast, the proportion of mothers receiving healthcare treatment for mental disorders and musculoskeletal conditions was similar across region of origin groups, and ranged from 2·1–2·6% for mental disorders and 2·91–3·25% for musculoskeletal conditions. Table 4. The association between any health condition; mental disorders; musculoskeletal conditions; and other health conditions in the year prior to pregnancy; and eligibility for earnings-related parental leave benefits by region of origin (n = 151·452)**Born in Sweden (n = 133 527)****Born in OECD regions (n = 8 451)****Born in non-OECD regions (n = 9 474)N%Model 1OR (95% CI)Model 2OR (95% CI)N%Model 1OR (95% CI)Model 2OR (95% CI)N%Model 1OR (95% CI)Model 2OR (95% CI)**Any health condition No healthcare treatment78 26758·62114 79056·68114 99752·7411 Any healthcare treatment55 26041·380·80(0·76–0·84) ***0.88(0.84–0.93) ***3 66143·320·87(0·75–1·00) *0.94(0.82–1.09)4 47747·260·91(0·82–1·00)0.96(0.87–1.07) No outpatient care79 31959·40114 83757·24115 08053·6211 Outpatient care54 20840·600·80(0·76–0·85) ***0.89(0.84–0.93) ***3 61442·760·87(0·75–1·00)0.95(0.82–1.10)4 39446·380 ·92(0·83–1·02)0.97(0.88–1.08) No hospitalisation126 58194·80117 96794·27118 80992·9811 Hospitalisation6 9465·200·59(0·54–0·65) ***0.69(0.63–0.77) ***4845·730·68(0·52–0·90) **0.77(0.58–1.01)6657·020·78(0·65–0·94) *0.86(0.71–1.04)Mental disorders No healthcare treatment130 12397·45118 27397·89119 22897·4011 Any healthcare treatment3 4042·550·18(0·16–0·19) ***0.23(0.21–0.25) ***1782·110·37(0·26–0·53) ***0.45(0.31–0.65) ***2462·600·39(0·30–0·51) ***0.43(0.33–0.57) *** No outpatient care130 23997·54118 28398·01119 24397·5611 Outpatient care3 2882·460·18(0·17–0·20) ***0.24(0.21–0.26) ***1681·990·42(0·29–0·62) ***0.51(0.34–0.76) **2312·440·42(0·32–0·55) ***0.45(0.34–0.60) *** No hospitalisation133 13499·71118 42799·72119 43499·5811 Hospitalisation3930·290·10(0·08–0·12) ***0.16(0.13–0.20) ***240·280·20(0·08–0·45) ***0.25(0.11–0.60) **400·420·25(0·13–0·47) ***0.35(0.18–0.67) **Musculoskeletal conditions No healthcare treatment129 19196·75118 20597·09119 16896·7711 Any healthcare treatment4 3363·251·00(0·86–1·16)1.08(0.93–1.26)2462·911·01(0·67–1·55)1.18(0.76–1.83)3063·231·58(1·13–2·20) **1.59(1.14–2.23) ** No outpatient care129 25696·80118 20797·11119 17596·8411 Outpatient care4 2713·201·00(0·86–1·16)1.08(0.93–1.25)2442·891·01(0·66–1·54)1.17(0.76–1.82)2993·161·63(1·16–2·28) **1.65(1.17–2.33) ** No hospitalisation133 28199·82118 44099·87119 45999·8411 Hospitalisation2460·180·93(0·51–1·71)1.09(0.89–2.01)110·131.08(0.13–8.49)1.32(0.16–10.73)150·160.70(0.22–2.19)0.67(0.21–2.15)Other health conditions No healthcare treatment81 43360·99114 94258·48115 18654·7411 Any healthcare treatment52 09439·010·89(0·85–0·94) ***0.97(0.92–1.03)3 50941·520·88(0·76–1·02)0.96(0.83–1.11)4 28845·260·91(0·82–1·01)0.97(0.87–1.07) No outpatient care82 52861·81114 99259·07115 27455·6711 Outpatient care50 99938·190·90(0–85-0·95) ***0.98(0.93–1.03)3 45940·930·89(0·77–1·03)0.97(0.84–1.12)4 20044·330·93(0·84–1·03)0.98(0.88–1.09) No hospitalisation127 09395·18117 99094·55118 84893·3911 Hospitalisation6 4344·820·72(0·64–0·80) 0.82(0.73–0.92) 4615·450·71(0·54–0·94) 0.80(0.60–1.07)6266·610·82(0·68–1·00) 0.88(0.72–1.08)Reference category is no health condition, mental disorder· musculoskeletal condition or other health conditionModel 1: Adjusted for child’s year of birth mother’s ageModel 2: Adjusted for child’s year of birth mother’s age, educationOR Odds ratio, 95%CI 95% Confidence intervals^^p < 0·05^^p < 0·01^^p < 0·001
Sub-analyses by origin (Table 4, Tables A4 and A5, Appendices 4 and 5) further showed that associations were typically strongest among Swedish-born mothers. Among mothers receiving healthcare treatment for any health condition, the odds of being eligible for earnings-related benefits were 0·80 (95%CI 0·76–0·84; Model 1) among Swedish-born mothers, 0·87 (95%CI 0·75–1·00; p < 0.05; Model 1) among mothers from OECD regions, and 0·91 (95%CI 0·82–1·00; p = 0.059; Model 1) among mothers from non-OECD regions, relative to their counterparts who did not receive healthcare treatment.
While mothers receiving healthcare treatment for mental disorders from all groups had significantly lower odds of being eligible for earnings-related benefits compared to their healthy counterparts, this association was most pronounced among Swedish-born mothers (OR 0·18, 95%CI 0·16–0·19). The odds of being eligible for earnings-related benefits was similar among foreign-born mothers (OR 0·37, 95%CI 0·26–0·53 for those from OECD regions (Model 1) versus OR 0·39, 95%CI 0·30–0·51 for those from non-OECD regions (Model 1)).
Similar to the main analysis, there was no evidence of an association between receiving treatment for musculoskeletal conditions in the year prior to pregnancy and being eligible for earnings-related benefits for Swedish-born mothers and mothers from OECD regions. However, the odds of being eligible for earnings-related benefits increased among mothers receiving outpatient care for musculoskeletal conditions who were from non-OECD regions (OR 1·63 95%CI 1·16–2·28; Model 1) compared with mothers from non-OECD regions who did not receive care. When education was included into the model, both Swedish-born mothers and mothers from OECD regions also had increased odds of being eligible for earnings-related benefits if they received treatment for musculoskeletal conditions.
Sensitivity analyses
We also examined the potential role of urbanicity in the association between health in the year before pregnancy and chronic health and eligibility for earnings-related parental leave benefits, and found no change in odd ratios estimates when urbanicity was included in our models (results not shown). Exclusion of mothers who were hospitalised (i.e., those with more severe illnesses) from analyses of outpatient care demonstrated estimates that were very similar to those observed in the main analyses (Table A6, Appendix 6).
Discussion
Our findings indicated that mothers who were hospitalised and/or received outpatient care before pregnancy, particularly for mental disorders, were less likely to be eligible for earnings-related parental leave benefits compared to mothers who did not receive healthcare treatment. Moreover, the likelihood of being eligible for more generous benefits was decreased further for mothers receiving healthcare treatment in the two consecutive years prior to pregnancy (indicative of chronic problems). Overall, no difference was observed between mothers with and without musculoskeletal conditions; however, mothers from non-OECD regions receiving outpatient care for musculoskeletal conditions were more likely to be eligible for earnings-related benefits.
In our study, mental health, rather than physical health, prior to pregnancy had a greater impact on eligibility for earnings-related parental leave benefits, suggesting that mechanisms explaining the relationship between health and labour market attachment may vary based on specific health outcomes. For example, some musculoskeletal conditions (e.g., back pain and neck strain) may temporarily prevent individuals from working with minimal impact on job security, whereas individuals with mental disorders may face greater challenges in the workplace, especially without supportive accommodations such as flexible hours and health-related leave [13]. Furthermore, individuals with mental disorders may also encounter greater difficulties in securing employment [14, 15].
Our findings are also in line with the accumulation of risk model [16], as we observed that mothers with chronic health conditions, particularly mental disorders, had even lower odds of being eligible for earnings-related parental leave benefits. This suggests that eligibility for more generous benefits may reinforce inequalities that existed before pregnancy.
In Sweden, healthcare access is universal for all residents; however, utilisation differs between native-born and foreign-born individuals, a trend observed in many high-income countries [17]. Evidence suggests that migrants typically use less psychiatric healthcare than Swedish-born individuals, particularly during their first years in the country [18]. However, utilisation among migrants increases with time, and those who have been in Sweden for more than a decade generally exhibit higher psychiatric care use. Additionally, psychiatric health care use among migrants varies depending on their region of origin [18].
We observed that mothers from non-OECD regions receiving outpatient care for musculoskeletal conditions remained in the labour market while undergoing treatment, leading to higher odds of being eligible for earnings-related benefits. This observation aligns with prior research [19, 20] where migrants tend to engage in more physically demanding jobs compared to native-born workers, and continue employment despite physical ailments. A similar pattern, albeit less pronounced, was observed for mothers from other origins when education was taken into consideration. It appears that highly educated mothers in all groups tend to remain in the labour market to secure earnings-related benefits, possibly being aware of the consequences of not being employed during this life stage. Furthermore, we observed an increase in the odds of eligibility only among mothers who received healthcare treatment in the year before pregnancy, but not among mothers with chronic musculoskeletal conditions. This observation may suggest that musculoskeletal conditions in the year before pregnancy are milder, allowing women to continue employment.
Furthermore, our findings showed that immigrant mothers, particularly those from non-OECD regions, were less likely to qualify for earnings-related benefits than Swedish-born mothers. Nonetheless, the associations between pre-pregnancy healthcare treatment and eligibility for earnings-related benefits were more pronounced among Swedish-born mothers, even though all mothers receiving healthcare treatment, regardless of their origin, had lower odds of eligibility for more generous benefits. This may indicate that immigrant mothers are more likely to remain active in the labour market even when they are unwell, a trend observed in other settings [21, 22].
The Swedish parental leave scheme is renowned for its generosity; however, as this study shows, the relatively strong work requirement for earnings-related parental leave benefits might be an unintentional source of economic inequalities, and further health inequalities. Thus, the health inequalities observed in this study could be larger in contexts with more stringent work requirements. For example, in some European countries, self-employed individuals do not receive the same entitlements as employed individuals; in the United Kingdom, self-employed individuals are not eligible to paid parental leave [23], while in Italy, self-employed parents are not entitled to the same length of paid leave as those employed (3 versus 6 months) [24]. Furthermore, even though the proportion of mothers who were not eligible for earnings-related benefits was relatively low (around 6%) in our study, the rising prevalence of mental disorders among young adults [25] and the increasing precariousness of the labour market [26], where temporary contracts continue to grow, suggest that inequalities in access to the most generous benefits can increase if strict conditions remain [27].
The main strength of the study is that we used data from Swedish total population and health registers, which ensures representativeness. Furthermore, by relying on medical records, we were able to avoid recall bias. The study does have some limitations. Firstly, we only included mothers with complete data. However, the proportion of missing data was low (only 6·3%). Secondly, although our health measures capture more severe health outcomes, such as hospitalisations, individuals in Sweden can self-refer to specialised outpatient care for mental disorders. Of adults receiving mental health care, 49% are treated in primary care, 32% in secondary care, and 18.5% are jointly treated in both primary and secondary care [28]. Accordingly, our measure was possibly able to capture milder mental health complaints in outpatient care. This may explain the observed association between health and eligibility for generous parental leave benefits even when there is likely some health-based selection into motherhood. Thirdly, we were not able to use a more detailed categorisation of birthplace in order to maintain enough statistical power; however, our categorisation matches those used in previous studies, ensuring comparability [11, 29]. Fourthly, our results were robust across different likelihood estimates (ORs and AMEs). Finally, despite using longitudinal data and being able to determine the temporal order of the events, we cannot rule out the possibility that a weaker attachment to the labour market is responsible for a mother’s poor health rather than the other way around.
To the best of our knowledge, this study is the first to evaluate whether there is health selection into earnings-related parental leave benefits, both in Sweden and worldwide. Consequently, comparisons with previous studies are not possible. The results of our study can inform policy makers to design much-needed equitable parental leave systems [30]. Our findings support the need to embrace a Health in all Policiesapproach, whereby health implications are considered when designing social interventions [31]. This framework facilitates an examination of structural factors that lead to health inequalities, and its adoption can enable an improved public health and health equity.
Generous parental leave has been shown to be protective for mother’s mental health including those with pre-existing mental health conditions [3]. Consequently, the fact that mothers with mental disorders are less likely to be eligible for more generous parental leave remunerations due to weaker labour market attachment [4] implies that the design of the parental leave policy, through its eligibility criteria, may contribute to increasing social and health inequalities in society. In Sweden, there is no formal childcare available for children under twelve months of age, which may place financial strain on parents during this period, potentially increasing health burdens [32, 33], and compromising gender equity, as fathers typically hold better positions in the labour market. Relaxing some of the stringent work requirements for eligibility for earnings-related parental leave benefits may contribute to reducing health inequities in society while promoting gender equity across social groups. In the Swedish context, this could be achieved by extending the work eligibility period, similar to the Norwegian model, where eligibility is based on being employed for six out of the last ten months before the birth and earnt above a minimum income level [34].
Moreover, mothers with access to childcare may return to work sooner than those with more generous benefits, as the basic benefit is insufficient as a living wage. This may result in less time for post-pregnancy recovery, reduced opportunities for bonding, and potentially suboptimal breastfeeding practices [35]. Furthermore, mothers with weak labour market attachment or low earnings may delay starting a family until they are older and established in the labour market, increasing the chances of experiencing age-related problems during pregnancy (including but not limited to maternal complications, such as pre-eclampsia, gestational diabetes and caesarean section) [36].
Conclusion
This is the first study to examine associations between mother’s health prior to pregnancy and eligibility for earnings-related parental leave benefits. Mothers who received specialist outpatient care or were hospitalised before pregnancy, particularly for mental disorders, were less likely to be eligible for earnings-related parental leave benefits, thereby highlighting inequalities in accessing the most generous parental leave benefits.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Försäkringskassan. Parental benefits [Föräldrapenning]: Försäkringskassan; 2023 [24 April 2023]. Available from: https://www.forsakringskassan.se/privatperson/foralder/foraldrapenning.
- 2Organization WH. Mental health at work: World Health Organization; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-health-at-work. Cited 12 July 2023.
- 3The Helsinki statement on Health in All Policies. Health Promotion International. 29(Supplement 1):i 17-i 8.10.1093/heapro/dau 03625217353 · doi ↗ · pubmed ↗