Navigating Treble Clef Aorta: A Challenge for Transfemoral Transcatheter Aortic Valve Replacement—A Case Report
Helen S. Anwar, José M. Montero-Cabezas, Frank Van Der Kley

TL;DR
This case report describes a successful TAVR procedure in a patient with a uniquely challenging aortic arch shape resembling a treble clef.
Contribution
The novelty lies in demonstrating the feasibility of transfemoral TAVR in a patient with an extremely tortuous aortic arch.
Findings
A patient with a treble clef-shaped aortic arch successfully underwent transfemoral TAVR.
The case highlights the importance of careful planning and advanced imaging in complex vascular anatomy.
Transfemoral access remains viable even in anatomically challenging scenarios.
Abstract
Transcatheter aortic valve replacement (TAVR) has emerged as a widely approved intervention for managing severe aortic stenosis. As the number of patients undergoing TAVR continues to rise, certain cases present unique challenges, particularly in relation to vascular access. This report highlights a case of successful transfemoral TAVR performed in a patient with an exceptionally tortuous and elongated aortic arch, characterized by significant curvature reminiscent of the treble clef musical symbol.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
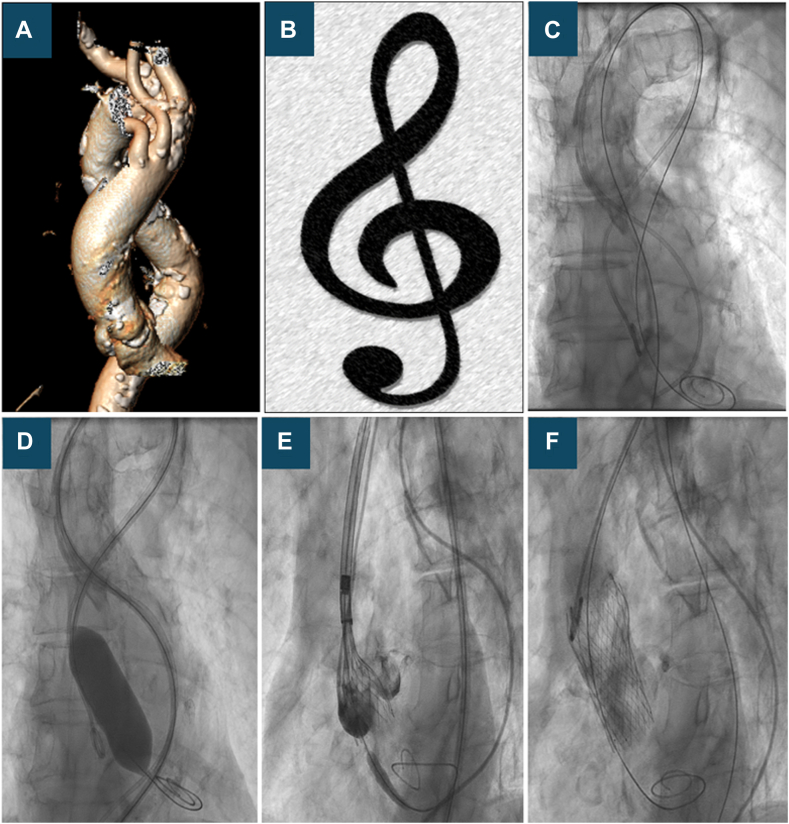 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Cardiac Imaging and Diagnostics
Tortuous aorta poses unique challenges during transcatheter aortic valve replacement (TAVR) procedure. The complexities of navigating highly twisted and curved vessels can hinder device delivery, increase the risk of complications such as vascular injury or device malposition, and lead to longer procedural time.1^,^2 Severe tortuosity of the access route can affect guide wire manipulation and increase the risk of left ventricular perforation.3 Advanced imaging techniques and preprocedural planning are crucial to navigate the complex anatomy, and specialized tools and skills, or alternative access routes, may be considered to ensure procedural success and patient safety.
Case presentation
An 84-year-old man with symptomatic severe aortic stenosis was referred to our institution for aortic valve intervention. Our patient had multiple cardiovascular risk factors (diabetes, hypertension, and dyslipidemia), previous percutaneous coronary intervention, and several comorbidities (a history of right mammary cancer and mastectomy, diverticulosis and left hemicolectomy, and right hip replacement). The patient’s surgical risk was high (EuroSCORE I logistic of 10.11%), and TAVR was discussed as the best and only interventional option for him.
During the pre-TAVR multidetector computed tomography (MDCT) workup, we found extremely diseased, tortuous, and elongated descending thoracic aorta and aortic arch resembling a “treble clef” on the reconstructed images (Figure 1A, B). Transaxillary TAVR was less favorable due to a porcelain aorta and an aberrant subclavian artery (arteria lusoria). Our center had little experience with transcarotid TAVR, so transfemoral TAVR was accepted with this challenging anatomy. Cerebral protection device (Sentinel; Boston Scientific) was discussed but deemed not applicable due to arteria lusoria.Figure 1Treble clef aorta: 3D multidetector computed tomography reconstruction and fluoroscopic imaging showed the extremely tortuous and elongated aortic arch resembling the Treble clef musical sign (A-C). Fluoroscopic imaging of transcatheter aortic valve replacement (D-F).
The TAVR procedure was done under local anesthesia with an ultrasound-guided puncture using a single right groin access. A14-F sheath (Cook) was placed in the descending aorta over the available super stiff INNOWI SX TAVR wire (SYMEDRIX GmbH) giving better support in this tortuous anatomy (Figure 1C). Valvuloplasty was done with a 22.0-mm VASC III balloon (OSYPKA AG) (Figure 1D). Medtronic Evolut FX valve was chosen owing to the great flexibility of the delivery system and for the superior benefit of recapture and retrieval of the valve. An Evolut FX 26.0-mm valve (Medtronic) was advanced into the aorta, which was very technically challenging, requiring extensive manipulation of the delivery system to negotiate the aortic arch, consisting of in back-and-forth movements and modification of the orientation of the wire position to facilitate the passage of the delivery system toward the aortic valve. Eventually, we succeeded, and the valve was correctly aligned and successfully deployed under accelerated pacing (Figure 1E, F; Supplemental Video 1).
Both final angiography and transthoracic echocardiography demonstrated good valve positioning and transvalvular gradient, with trace paravalvular leakage. At the end of the procedure, an aortogram was performed, which did not show any evidence of aortic injury. No other complications such as conduction defect or stroke were detected.
Discussion
TAVR has become an established technique to treat patients with severe aortic stenosis aged older than 75 years.4 The recommendations are now extended to more patients even with moderate or low surgical risk after the favorable outcomes shown by multiple trials.5^,^6 Meticulous preprocedural planning is pivotal for the success of TAVR procedures. The primary objectives of this planning are to determine the most suitable vascular access route and conduct a comprehensive anatomical assessment of the aortic valve and aortic root. These evaluations are critical for selecting the appropriate valve type and size.7 Preprocedural multimodality imaging including echocardiography, angiography, and MDCT is essential in addressing these objectives, with MDCT playing a crucial role in precisely assessing the vascular access site.
Our patient’s pre-TAVR workup revealed an extremely tortuous and elongated aortic arch and descending thoracic aorta. The tortuous aorta has been described in previous literature,8 but an extremely tortuous and elongated aortic arch with arteria lusoria has not been stated before. This type of abnormality increases the challenges for both transfemoral and trans-axillary access.
Conclusions
The precise and proper pre-TAVR MDCT-based planning makes performing transfemoral TAVR in even the most complex anatomical scenarios feasible using tailored techniques.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kinnel M.Faroux L.Villecourt A.Abdominal aorta tortuosity on computed tomography identifies patients at risk of complications during transfemoral transcatheter aortic valve replacement Arch Cardiovasc Dis 113320201591673173244510.1016/j.acvd.2019.10.006 · doi ↗ · pubmed ↗
- 2Mach M.Poschner T.Hasan W.The Iliofemoral tortuosity score predicts access and bleeding complications during transfemoral transcatheter aortic valve replacement: Data from the V Ienna Cardio Thoracic a Ortic valve registr Y (VICTORY)Eur J Clin Invest 516202111210.1111/eci.13491 PMC 824392133432599 · doi ↗ · pubmed ↗
- 3Ichise T.Nagata Y.Nakatsuji H.Guidewire-induced left ventricular perforation related to thoracic aorta tortuosity during transcatheter aortic valve implantation J Transcatheter Valve Ther 61202414
- 4Thyregod H.G.H.Jørgensen T.H.Ihlemann N.Transcatheter or surgical aortic valve implantation: 10-year outcomes of the NOTION trial Eur Heart J 45132024111611243832182010.1093/eurheartj/ehae 043PMC 10984572 · doi ↗ · pubmed ↗
- 5Mack M.J.Leon M.B.Thourani V.H.Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients N Engl J Med 380182019169517053088305810.1056/NEJ Moa 1814052 · doi ↗ · pubmed ↗
- 6Reardon M.J.Van Mieghem N.M.Popma J.J.Surgical or transcatheter aortic-valve replacement in intermediate-risk patients N Engl J Med 376142017132113312830421910.1056/NEJ Moa 1700456 · doi ↗ · pubmed ↗
- 7Bloomfield G.S.Gillam L.D.Hahn R.T.A practical guide to multimodality imaging of transcatheter aortic valve replacement J Am Coll Cardiol Img 54201244145510.1016/j.jcmg.2011.12.01322498335 · doi ↗ · pubmed ↗
- 8Liu S.Toleva O.Ravandi A.Pozeg Z.Menkis A.Kass M.Transcatheter aortic valve implantation in an extremely tortuous S-shaped aorta Case Rep Cardiol 201720171310.1155/2017/2936513 PMC 535286928352480 · doi ↗ · pubmed ↗