Polyostotic vertebral osteomyelitis and myositis in a dog with Anaerobiospirillum succiniciproducens bacteraemia
T. Liatis, A. Skarbek, C. Jones, S. Wyatt

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
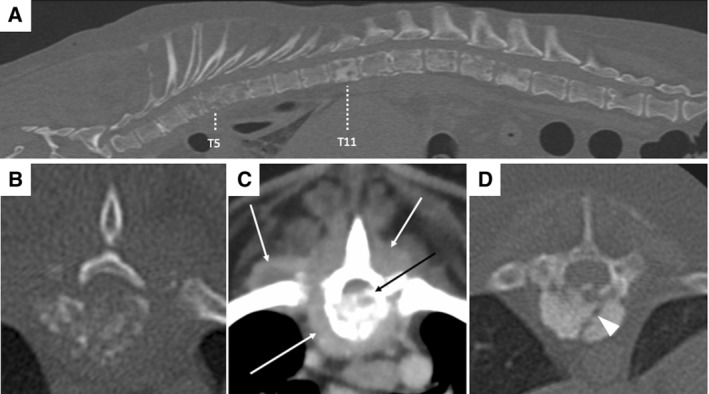 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMicrobial infections and disease research · Hematological disorders and diagnostics · Orthopedic Infections and Treatments
A 12‐year‐old male neutered Dachshund presented following a 3‐week history of lethargy, hyporexia, pyrexia and spinal pain, which acutely progressed to non‐ambulatory paraparesis. Amoxicillin‐clavulanate 20 mg/kg intravenously was administered once 1 day prior. The dog was diagnosed with sterile panniculitis 4‐years prior and has since been maintained on oral prednisolone (currently 0.8 mg/kg once on alternate days). Physical examination revealed pyrexia and generalised poor muscling. Neuroanatomical localisation was consistent with a T3‐L3 myelopathy. Haematology revealed inflammatory leukogram, and anaemia (28.5%, reference intervals [RI]: 37% to 55%), whilst serum biochemistry revealed increased C‐reactive protein (167.6 mg/L, RI <10 mg/L). CT revealed polyostotic osteolytic lesions affecting multiple vertebrae (Fig 1), the right eleventh rib, iliac wings and left scapula. Additionally, there were thickened heterogeneously hyperattenuating and moderately enhancing paraspinal soft tissues and a cranial mediastinal lymphadenomegaly. Differential diagnoses included vertebral osteomyelitis (bacterial/fungal) or neoplasia (multiple myeloma/multifocal osteosarcoma). Urinalysis was unremarkable including negative Bence‐Jones proteins. CT‐guided cytology of T5 and L3 vertebrae and paraspinal muscles suggested neutrophilic inflammation, whilst hepatic and splenic cytology were unremarkable. Bone marrow cytology and biopsy from the right ilium revealed myeloid hyperplasia without evidence of microorganisms or neoplastic cells. Bacterial and fungal cultures from urine and bone marrow were negative. Blood culture was positive to Anaerobiospirillum succiniciproducens and a diagnosis of suspected bacterial vertebral osteomyelitis and myositis was made. Concurrent meningomyelitis cannot be excluded as cerebrospinal fluid analysis was not performed. Treatment with amoxicillin‐clavulanate for 12 weeks and multimodal analgesia was initiated, and prednisolone was discontinued. At 8‐weeks, the dog was comfortable but remained non‐ambulatory, and subsequently had a relapse of clinical signs (pyrexia, anorexia and marked spinal hyperaesthesia) 4 weeks after discontinuation of antibiotics. A. succiniciproducens is a rare anaerobic bacterium considered part of the normal gastrointestinal microbiota in dogs and it has been implicated in sporadic cases of bacteraemia, usually in immunocompromised human patients. In this case, chronic immunosuppression was proposed as a cause for opportunistic bacterial infection with a commensal species. Urine and bone marrow cultures may be negative due to prior use of antibiotics or their low sensitivity in regions with mild lesions and low microbial burden (e.g., iliac bone).