Pulmonary Embolism in Patients with End-Stage Kidney Disease Starting Dialysis
Kunal N. Patel, Wan-Chi Chan, Vivek Bhat, Monil M. Majmundar, Harsh Mehta, Cyrus Munguti, Kartik Munshi, Sri G. Yarlagadda, Gaurav M. Parmar, Aditya M. Sharma, Daniella Kadian-Dodov, Lewis G. Satterwhite, Jinxiang Hu, Jordan Baker, MS, Kamal Gupta

TL;DR
This study looks at how common and severe pulmonary embolism is in patients starting dialysis for kidney failure and how anticoagulants are used.
Contribution
The study provides new insights into pulmonary embolism incidence and anticoagulant use in patients beginning dialysis.
Findings
Pulmonary embolism occurs at a notable rate in patients starting dialysis.
Anticoagulant use varies among patients with end-stage kidney disease.
Outcomes for patients with pulmonary embolism during dialysis initiation are examined.
Abstract
This cohort study examines the incidence and outcomes of pulmonary embolism as well as anticoagulant use among patients with end-stage kidney disease initiating dialysis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristic | Patients with ESKD, No. (%) | |
|---|---|---|
| All (N = 288 073) | With PE (n = 2377) | |
| Sex | ||
| Male | 161 752 (56.2) | 1146 (48.2) |
| Female | 126 321 (43.8) | 1231 (51.8) |
| Race | ||
| Asian and other | 17 410 (6.0) | 72 (3.0) |
| Black | 71 471 (24.8) | 806 (33.9) |
| White | 199 192 (69.2) | 1499 (63.1) |
| Age, mean (SD), y | 68.7 (12.4) | 66.7 (14.1) |
| Age group, y | ||
| <50 | 22 846 (7.9) | 302 (12.7) |
| 50-64 | 58 352 (20.3) | 506 (21.3) |
| 65-79 | 153 275 (53.2) | 1170 (49.2) |
| ≥80 | 53 600 (18.6) | 399 (16.8) |
| ESKD cause | ||
| Diabetes | 144 406 (50.1) | 1066 (44.9) |
| Hypertension | 92 735 (32.2) | 793 (33.4) |
| Other causes | ||
| Total | 50 932 (17.7) | 518 (21.8) |
| Glomerulonephritis | 16 753 (5.8) | 165 (6.9) |
| Cystic kidney | 4914 (1.7) | 35 (1.5) |
| Urologic causes | 4469 (1.6) | 45 (1.9) |
| Not specified | 24 796 (8.6) | 273 (11.5) |
| Dialysis modality | ||
| Hemodialysis | 254 335 (88.3) | 2181 (91.8) |
| Peritoneal dialysis | 33 738 (11.7) | 196 (8.3) |
| Comorbid conditions | ||
| CAD | 76 443 (26.5) | 672 (28.3) |
| Cancer | 27 419 (9.5) | 304 (12.8) |
| CHF | 106 745 (37.1) | 988 (41.6) |
| COPD | 37 055 (12.9) | 426 (17.9) |
| CVA or TIA | 32 320 (11.2) | 270 (11.4) |
| Diabetes | 184 476 (64.0) | 1472 (61.9) |
| Hypertension | 262 274 (91.0) | 2154 (90.6) |
| PAD | 47 291 (16.4) | 425 (17.9) |
| Tobacco use | 41 994 (14.6) | 494 (20.8) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Acute Ischemic Stroke Management · Atrial Fibrillation Management and Outcomes
Introduction
End-stage kidney disease (ESKD) confers a high risk of pulmonary embolism (PE) and is associated with relatively poor outcomes.^1,2^ Furthermore, ESKD is associated with a greater risk of bleeding, complicating management with anticoagulation (AC).^1^ Despite the complexity, there is a paucity of data regarding PE in patients with ESKD. We retrospectively analyzed data from the US Renal Data System (USRDS) to study the incidence, AC use, and outcomes of PE in patients with ESKD initiating dialysis.
Methods
Using USRDS data, we identified incident patients with ESKD initiating dialysis from 2011 to 2019. Included patients had fee-for-service Medicare coverage within the first 90 days of dialysis initiation (eFigure in Supplement 1). Patients with prior atrial fibrillation, deep vein thrombosis or PE, or AC use were excluded. Outcomes included 1-year PE hospitalization incidence, mortality (in-hospital and 30-day), AC use, inferior vena cava filter use, PE recurrence, and differences in outcomes between hemodialysis (HD) and peritoneal dialysis (PD) (eMethods, eTable in Supplement 1). Data extraction and analyses were performed from March to May 2024 using SAS, version 9.4 (SAS Institute Inc). Continuous variables were compared using a 2-sample t-test, and categorical variables were compared using Pearson χ^2^ test. Two-sided P < .05 was statistically significant. This cohort study was approved by the University of Kansas Medical Center's Institutional Review Board and USRDS with a waiver of informed consent because data were deidentified. We followed the STROBE reporting guideline.
Results
We identified 288 073 patients with ESKD (mean [SD] age, 68.7 [12.4] years; 161 752 males [56.2%]) who were initiating dialysis (Table). The 1-year PE incidence was 0.84% or 942 per 100 000 person-years, increasing from 925 to 1016 per 100 000 person-years between 2011 and 2019 (P = .05). The 3-year incidence was 1.7%. In-hospital and postdischarge 30-day mortality rates were 13.7% and 13.1%, respectively, with no significant temporal trends.
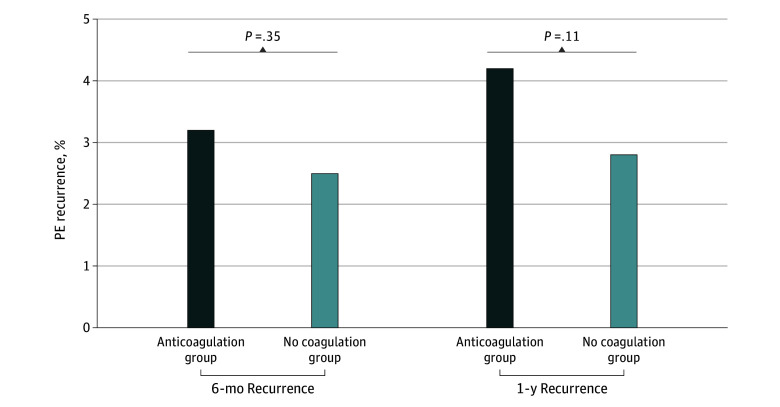
Among 2025 patients discharged alive after PE hospitalization, the 1-year recurrence rate was 4.1%. Of 1454 patients (71.8%) with Part D Medicare coverage, only 597 (41%) filled an AC prescription, with similar PE recurrence rates in those who received an AC prescription and those who did not (4.2% vs 2.8%; P = .11) (Figure). Inferior vena cava filters were placed in 8% of patients, decreasing from 12.6% in 2011 to 5.1% in 2019 (P < .001). Patients who received PD vs HD had a lower 1-year PE incidence (0.61% vs 0.87%, P < .001; hazard ratio [HR], 0.68; 95% CI, 0.58-0.80; P < .001), but in-hospital and 30-day mortality rates were similar and not statistically significant across modalities.
Six-Month and 1-Year Pulmonary Embolism (PE) Recurrence With and Without Anticoagulation Among Patients With End-Stage Kidney Disease Initiating Dialysis
Discussion
This study highlights the complexity of clinical decision-making regarding AC in patients with ESKD who experience PE. Fewer than half of the patients in this cohort filled postdischarge prescriptions for ACs. Low use of AC in these patients and lack of clear clinical benefit in this study is similar to that seen in patients with ESKD and atrial fibrillation, where the net benefit of AC to prevent stroke or death is uncertain.^3,4^
Patients receiving PD had a significantly lower 1-year PE incidence than those receiving HD even after adjusting for confounders. The mechanism of this finding remains unclear and warrants further investigation. The 1-year incidence of PE in patients with ESKD initiating dialysis from 2011 to 2019 exceeded prior estimates, likely reflecting advancements in imaging for PE detection and possibly improvements in coding practices.^1,5^ The persistently high mortality without significant improvement over time in patients with ESKD compared with the general population reflects the challenges of managing PE in ESKD.^6^
Study limitations include reliance on administrative data, with potential miscoding and lack of clinical granularity. Exclusion of younger patients without Medicare coverage limits generalizability to this subgroup. The low use and unclear benefit of AC following PE underscores the need for further research into the mechanisms of increased thrombotic risk to optimize AC strategies and improve outcomes in this high-risk population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tveit DP, Hypolite IO, Hshieh P, . Chronic dialysis patients have high risk for pulmonary embolism. Am J Kidney Dis. 2002;39(5):1011-1017. doi:10.1053/ajkd.2002.3277411979344 · doi ↗ · pubmed ↗
- 2Goto S, Haas S, Ageno W, ; GARFIELD-VTE Investigators. Assessment of outcomes among patients with venous thromboembolism with and without chronic kidney disease. JAMA Netw Open. 2020;3(10):e 2022886. doi:10.1001/jamanetworkopen.2020.2288633112399 PMC 7593818 · doi ↗ · pubmed ↗
- 3Kao TW, Chen ZW, Lin YH. Anticoagulation for patients with concomitant atrial fibrillation and end-stage renal disease: a systematic review and network meta-analysis. J Am Heart Assoc. 2024;13(8):e 034176. doi:10.1161/JAHA.123.03417638606775 PMC 11262503 · doi ↗ · pubmed ↗
- 4Goel N, Jain D, Haddad DB, Shanbhogue D. Anticoagulation in patients with end-stage renal disease and atrial fibrillation: confusion, concerns and consequences. J Stroke. 2020;22(3):306-316. doi:10.5853/jos.2020.0188633053946 PMC 7568986 · doi ↗ · pubmed ↗
- 5Kumar G, Sakhuja A, Taneja A, ; Milwaukee Initiative in Critical Care Outcomes Research (MICCOR) Group of Investigators. Pulmonary embolism in patients with CKD and ESRD. Clin J Am Soc Nephrol. 2012;7(10):1584-1590. doi:10.2215/CJN.0025011222837271 PMC 3463201 · doi ↗ · pubmed ↗
- 6Di Nisio M, van Es N, Büller HR. Deep vein thrombosis and pulmonary embolism. Lancet. 2016;388(10063):3060-3073. doi:10.1016/S 0140-6736(16)30514-127375038 · doi ↗ · pubmed ↗