Spongiform Venous Malformation Presenting as an Extensive Lesion in the Gluteal Region
Ilse Marilú Gutiérrez Villarreal, Circe Ancona Castro, Carlos S Sáenz de León, Génesis A Cabral Rodríguez, Juan Pablo Montemayor Lozano, Roberto Arenas Guzmán

TL;DR
A 53-year-old woman with a large gluteal venous malformation showed significant improvement after sclerotherapy treatment.
Contribution
This case emphasizes the effectiveness of sclerotherapy in managing extensive venous malformations.
Findings
Sclerotherapy led to significant improvement in the patient's condition.
Doppler ultrasound and MRI were effective in diagnosing the venous malformation.
Multidisciplinary management is crucial for treating complex venous malformations.
Abstract
Venous malformations (VMs) are vascular malformations affecting a small portion of the population. A 53-year-old woman presented with a congenital VM on the left gluteal region confirmed through clinical imaging and histopathology. Treatment with sclerotherapy led to significant improvement. VMs often cause pain, swelling, or mobility limitations. Diagnosis relies on Doppler ultrasound and MRI, while sclerotherapy is the preferred treatment due to its safety and efficacy. This case highlights sclerotherapy as a key treatment in a multidisciplinary management approach.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
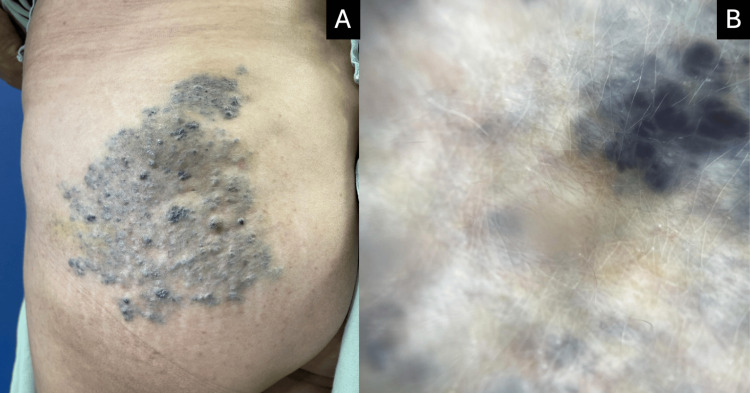 Figure 1
Figure 1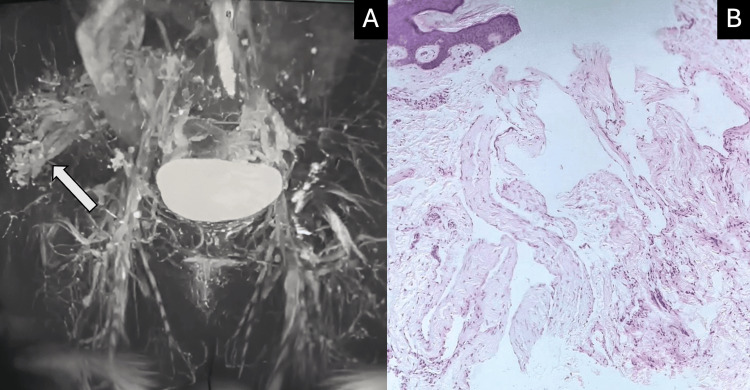 Figure 2
Figure 2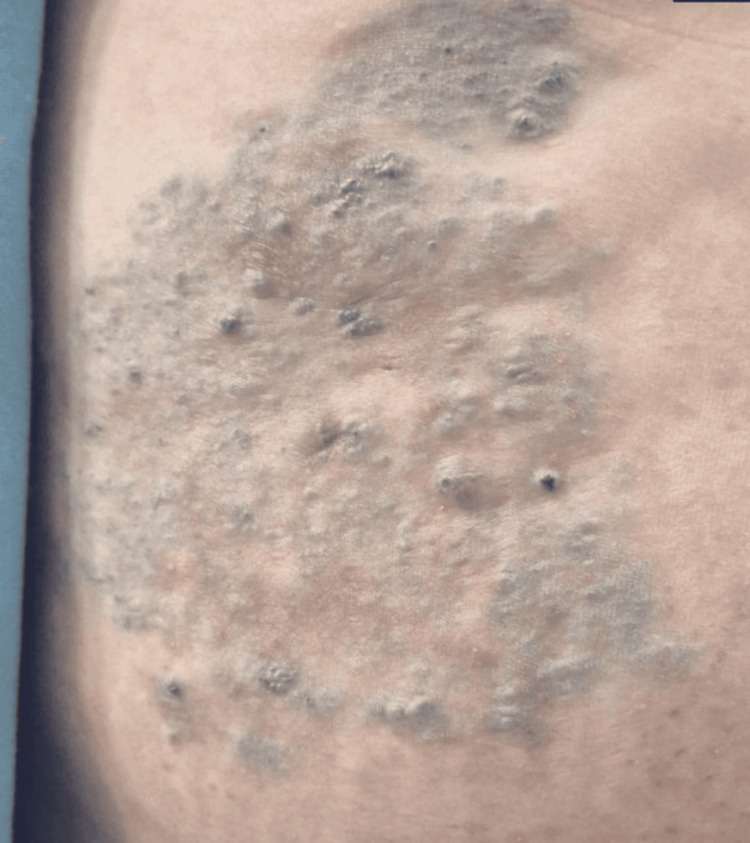 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations and Hemangiomas · Diagnosis and Treatment of Venous Diseases · Central Venous Catheters and Hemodialysis
Introduction
Venous malformations (VMs) are among the frequent types of vascular malformations, occurring in approximately 1 to 5 out of every 10,000 people [1]. VMs often cause pain, swelling, or mobility limitations. Diagnosis relies on doppler ultrasound and MRI, while sclerotherapy is the preferred treatment due to its safety and efficacy [2]. A 53-year-old woman presented with a congenital VM on the left gluteal region, which was confirmed through clinical imaging and histopathology. This case highlights sclerotherapy as a key treatment in a multidisciplinary management approach.
Case presentation
A 53-year-old woman with a personal medical history relevant for rheumatoid arthritis since 2015 in control with etanercept and leflunomide presented to us with a 6 cm violaceous neoformation affecting the gluteal region that had been present since birth, with progressive growth of the lesion starting at 18 years of age. Two months prior to the visit, the lesion began bleeding after an unspecified direct trauma, which was the reason for the examination. The patient presented with a dermatosis on the posterolateral aspect of the left lower extremity, extending to the outer gluteal region. It consisted of a vascular-appearing plaque-like neoformation measuring approximately 13×11.5 cm. The lesion was rhomboid in shape, blue-green in color, with well-defined regular borders, an irregular cobblestone-textured surface, and multiple nodules of varying sizes ranging from 5 to 10 mm in diameter (Figure 1A). The lesion was compressible to pressure, and no lesions were found in oral mucosa or annexes. She reported occasional pain in the affected area and slight heaviness of the limb. Dermoscopy showed multiple blue lacunae that tend to group together in a circular arrangement (Figure 1B).
Venous malformation images.(A) Spongiform venous malformation affecting the gluteal region. (B) Dermoscopy shows multiple blue lacunae that tend to group together in a circular arrangement.
In our initial approach, a simple ultrasound of the left gluteal region was performed, which revealed an increase in subcutaneous cellular tissue thickness (33 mm) compared to the contralateral side, with heterogeneous, predominantly echogenic characteristics. Doppler ultrasound showed tortuous low-flow vessels and an 8 mm phlebolith. Contrast magnetic resonance imaging of the pelvis was performed, revealing multiple linear and serpiginous paths hyperintense on T2, reported in the subcutaneous cellular tissue of the left gluteal area, affecting the subdermal region with extension to the subcutaneous cellular tissue, gluteus maximus muscle, and the most proximal portion of the iliac crest (Figure 2A). A punch biopsy was performed due to uncertainty regarding the type of vessel involved, which reported an epidermis with loose hyperkeratosis and follicular plugging. In the reticular dermis, numerous vascular spaces lined by flat endothelial cells and an intercommunicated fibrous stroma were observed (Figure 2B). Immunohistochemistry stains were performed, which tested positive for CD34 and negative for podoplanin/D2-40 and CD31.
Contrasted MR (A) Shows multiple linear and serpiginous paths showing extension of the lesion marked by an arrow. (B) Dermis with numerous vascular spaces lined by flat endothelial cells and an intercommunicated fibrous stroma.
Considering our diagnostic protocol, the findings suggested a vascular malformation of venous origin, and ultimately, a diagnosis of spongiform venous malformation was made. The patient was treated with a 1% polidocanol sclerotherapy session (with a total volume of 8 mL of the solution injected), achieving significant improvement of the lesion with aesthetic and functional improvement; she did not experience any adverse events (Figure 3).
Improvement of the lesion. Improved lesion after one session of 1% polidocanol sclerotherapy.
Discussion
Venous malformations (VMs) are estimated to occur in approximately 1-5 per 10,000 live births, making them the most prevalent type of vascular malformation (70%) [1]. There is no clear ethnic or gender predisposition, although some studies suggest that venous malformations (VMs) are more frequently observed in females [2,3]. Venous malformations (VMs) are congenital, slow-flow lesions composed of a network of serpentine veins connected by ectatic venous channels that lack vascular smooth muscle [3]. These malformations can be focal, multifocal, or infiltrative and are commonly located in the head and neck (40%), extremities (40%), and trunk (20%) [4].
Pain is the most common symptom associated with venous malformations (VMs). According to Rikihisa et al., pain was most frequently observed in lesions larger than 10 cm (67%), followed by lesions between 5 cm and 10 cm (56%) and those smaller than 5 cm (29%). Subfascial venous malformations (VMs) in the lower extremities are more likely to cause pain. As children age, the frequency of pain increases, reaching 50% by approximately 7 years of age [4,5]. Additional symptoms of venous malformations (VMs) include swelling, varicosity, ulcers, discoloration, itching, and a sense of heaviness, with their manifestation varying based on lesion location, extent, and depth. Despite the movement limitations often reported in venous malformations (VMs) involving muscle tissue [6], the patient in this case did not experience functional or mobility restrictions.
The initial imaging technique at some reference centers for vascular malformations is gray-scale ultrasonography combined with color Doppler imaging and spectral analysis due to its affordability, lack of ionizing radiation, and ability to provide fast, real-time results. However, this method has limitations, such as reduced accuracy in assessing large or deep lesions and difficulties detecting bone involvement. On color Doppler imaging, monophasic venous flow is the typical finding within venous malformations (VMs) [7].
Niu et al. reported 74 cases of vascular malformations, with lymphatic malformations being the most common subtype (47 cases) and venous malformations the second most common (15 cases) [8]. Magnetic resonance (MR) imaging is considered the most valuable imaging modality for vascular malformations (VMs) due to its high temporal and contrast resolution, which enables precise evaluation of the malformations and their relationship with adjacent structures. Venous malformations (VMs) typically appear hypointense on T1-weighted images and hyperintense on T2-weighted images and fluid-sensitive sequences. Phleboliths, a characteristic feature of venous malformations (VMs), are visualized as scattered, rounded areas of low signal intensity [8].
Histopathologic diagnosis is rarely necessary. VMs are composed of irregular venous channels lined by flat endothelium, and vascular endothelial cells are negative for lymphatic endothelial markers such as D2-40 and PROX-1. D2-40 binds to a specific marker found in lymphatic endothelial cells, helping to differentiate blood vessels from lymphatic vessels. PROX-1, on the other hand, plays a key role in the differentiation and maturation of lymphatic vessels and is used to evaluate lymphatic malformations and tumors associated with the lymphatic system [3]. Both markers are crucial for studying vascular malformations, but neither was available in our local setting.
There is no fully standardized treatment for venous spongiform malformations (VSMs), and treatment is often sought due to pain or cosmetic concerns. When considering treatment options, factors such as the lesion's pathophysiology, etiology, and potential complications should be considered [9]. The first step in managing vascular malformations is often conservative therapy, particularly when symptoms are mild or intermittent [10].
Treatment options for venous spongiform malformations (VSMs) include surgery, sclerotherapy, and laser therapy, with sclerotherapy being the preferred technique due to its minimally invasive nature, cost-effectiveness, and superior outcomes compared to surgery, which carries a higher risk of intraoperative bleeding and complications [9-11]. Combining these therapies may result in improved outcomes, both in terms of functionality and aesthetics. Well-demarcated, localized lesions tend to respond well to surgical resection [10].
Conclusions
Venous malformations, particularly when affecting large or extensive areas, often require multiple treatment sessions to address a range of symptoms, from aesthetic concerns to more debilitating issues. Fortunately, sclerotherapy offers a minimally invasive treatment option with low associated risks and generally acceptable outcomes, with many patients opting for repeated sessions. The management of VMs requires a multidisciplinary approach involving a dermatologist, interventional radiologist, vascular surgeon, plastic surgeon, and psychologist to ensure adequate care. Our case highlights the challenges faced by patients with spongiform venous malformations, particularly in obtaining an accurate diagnosis and receiving effective treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Venous malformations Semin Pediatr Surg Cooke-Barber J Kreimer S Patel M Dasgupta R Jeng M 1509762920203306928410.1016/j.sempedsurg.2020.150976 · doi ↗ · pubmed ↗
- 2Characteristics, clinical presentation, and treatment outcomes of venous malformation in the extremities J Vasc Surg Venous Lymphat Disord Kim H Joh J Labropoulos N 1521581020223409110410.1016/j.jvsv.2021.05.011 · doi ↗ · pubmed ↗
- 3Evaluation of pain incidence due to venous malformation based on data from 85 institutions in Japan J Vasc Surg Venous Lymphat Disord Rikihisa N Akita S Osuga K Mimura H Yuzuriha S Sasaki S 244250820203147127510.1016/j.jvsv.2019.03.008 · doi ↗ · pubmed ↗
- 4Comprehensive phenotypic and genomic characterization of venous malformations Hum Pathol Hirose K Hori Y Ozeki M 485514520243836781610.1016/j.humpath.2024.02.004 · doi ↗ · pubmed ↗
- 5Low-flow vascular malformation pitfalls: from clinical examination to practical imaging evaluation-part 2, venous malformation mimickers AJR Am J Roentgenol Olivieri B White CL Restrepo R Mc Keon B Karakas SP Lee EY 95296220620162699964710.2214/AJR.15.15794 · doi ↗ · pubmed ↗
- 6Clinical and sonographic features of pediatric soft-tissue vascular anomalies part 2: vascular malformations Pediatr Radiol Johnson CM Navarro OM 119612084720172877918710.1007/s 00247-017-3906-x · doi ↗ · pubmed ↗
- 7Imaging of vascular malformations Radiol Clin North Am Hussein A Malguria N 8158305820203247154610.1016/j.rcl.2020.02.003 · doi ↗ · pubmed ↗
- 8Clinicopathologic study of pediatric vascular anomalies: a report of 117 cases Zhonghua Bing Li Xue Za Zhi Niu HL Zhou SY Lin QQ 2522574520162703338910.3760/cma.j.issn.0529-5807.2016.04.008 · doi ↗ · pubmed ↗