Imaging Findings of Lupus Mastitis: A Systematic Review of Case Studies
Stephanie Nagy, Kitty Daniel, Marc M Kesselman

TL;DR
This study reviews imaging findings of lupus mastitis, a rare lupus-related breast condition, to improve diagnosis and reduce misdiagnosis.
Contribution
The paper provides a systematic review of imaging findings and suggests a clinical guideline for diagnosing lupus mastitis.
Findings
LM is mostly unilateral and can occur in any breast quadrant.
Most patients were women with an average age of 44 and disease duration of 10 years.
Imaging findings are critical due to the lack of established diagnostic guidelines for LM.
Abstract
Lupus mastitis (LM) is a rare manifestation of systemic lupus erythematosus, resulting in an inflammatory process within the breast tissue. This condition presents diagnostic challenges due to its similarity to other breast pathologies, including infections and malignancies. Clinically, patients may exhibit symptoms such as breast pain, swelling, and erythema, often leading to further investigation through imaging and histopathological analysis. Given the absence of established clinical guidelines for LM, identifying the most effective imaging and laboratory techniques is essential for accurate diagnosis and treatment. In this paper, 32 patient case reports were analyzed, with 20 patients having previous diagnoses of lupus and 12 not previously diagnosed. The study population comprised 90.6% (n=29) women, with a mean age of 44 years and an average disease duration of 10 years. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
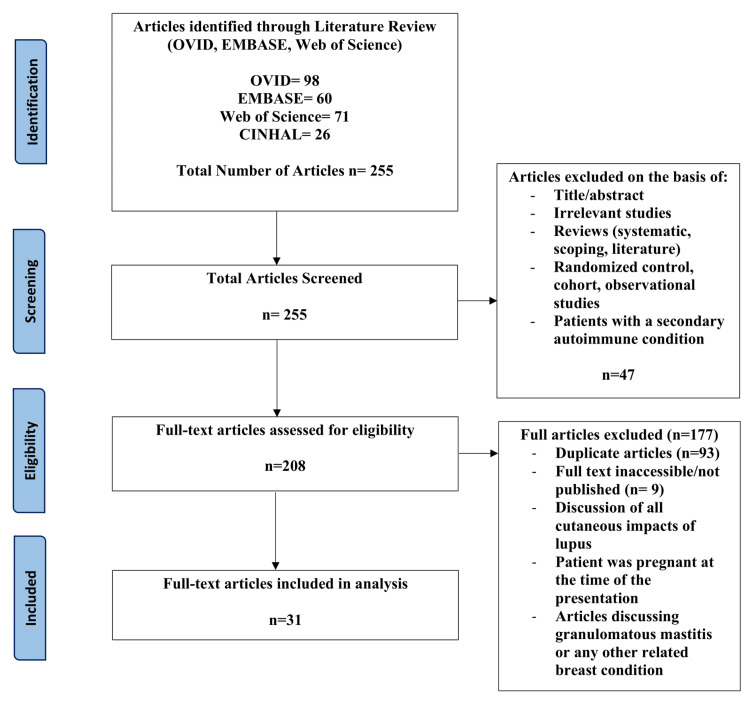 Figure 1
Figure 1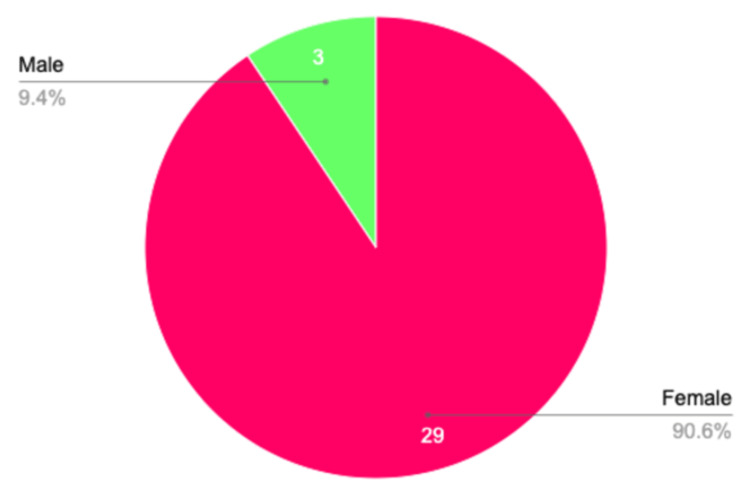 Figure 2
Figure 2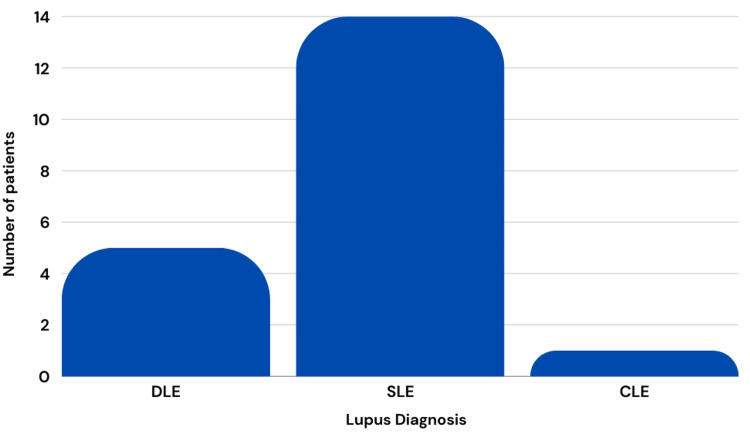 Figure 3
Figure 3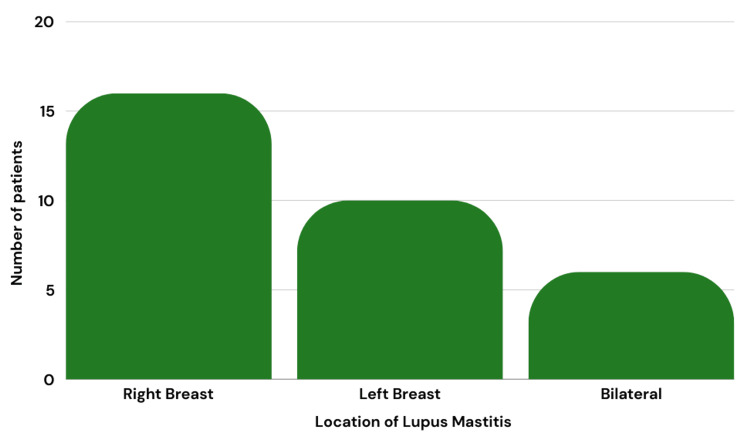 Figure 4
Figure 4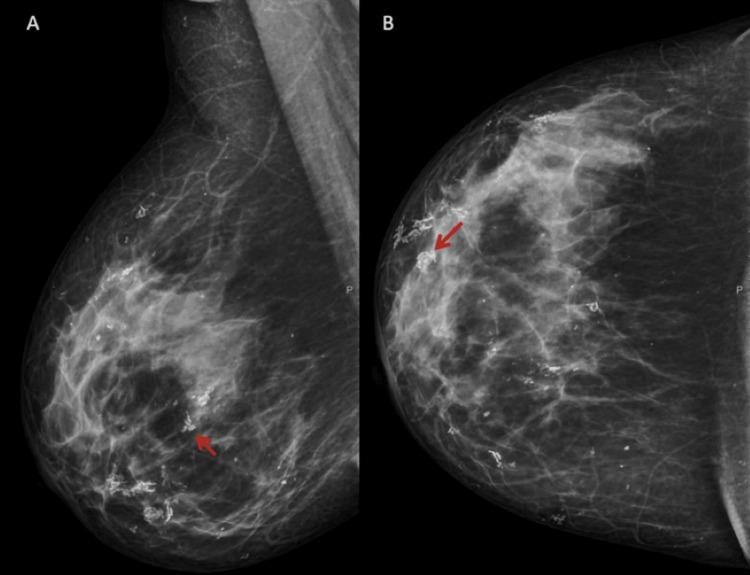 Figure 5
Figure 5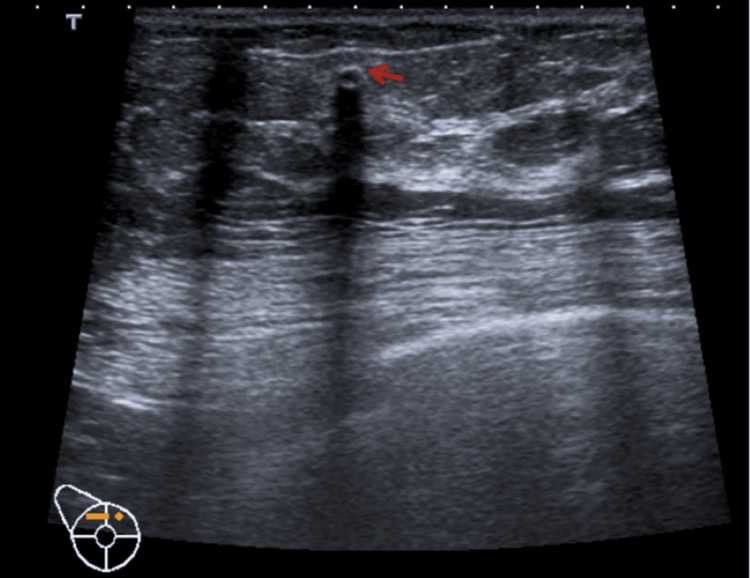 Figure 6
Figure 6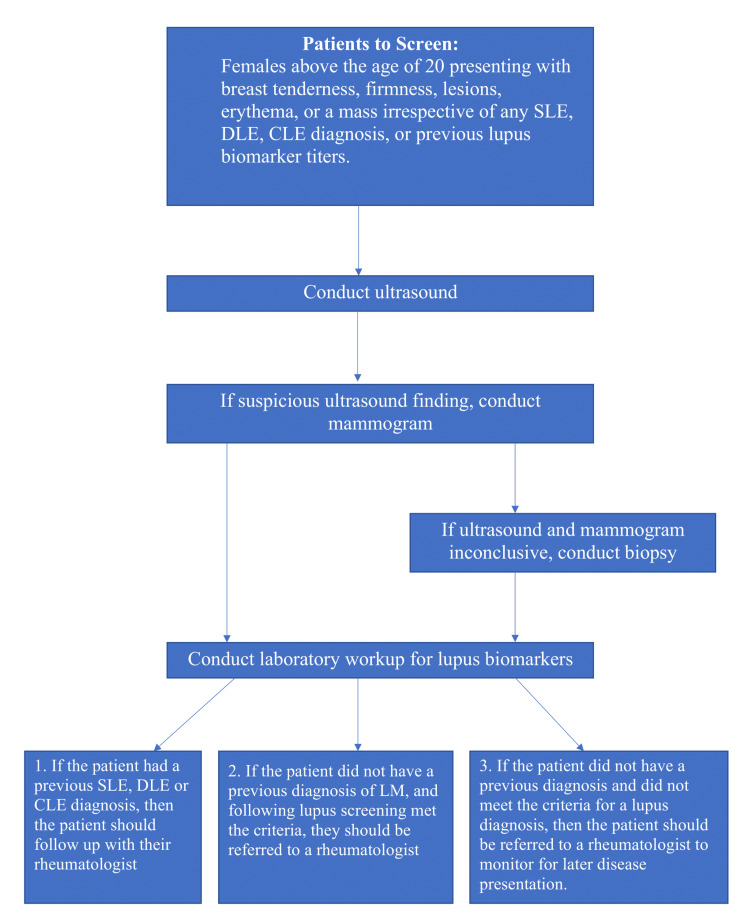 Figure 7
Figure 7| Title | Patient Age and Gender (M/F) | Ethnicity | Disease Duration | History of Lupus | Lab Results | Location | Physical Appearance | US Findings | Mammogram Findings | MRI Findings | CT Findings | Biopsy/Histological Findings | Treatment Received |
| Guo et al. [ | 27 F | Asian (Chinese) | No previous diagnosis | No previous diagnosis. | ESR=57mm; IgG =17.33 g/L; IgA = 3.95 g/L; IgM normal; C3 and C4 normal; ANA normal; ANCA negative ; ribosomal P protein positive | Upper inner quadrant on the right breast | Skin thickening, erythematous; nine months later: the patient declined initial treatment and returned with a palpable mass, ulceration, lymphadenopathy | Subcutaneous, hyperechoic 3cm lesion; abundant peripheral and internal blood flow signals; no distinct mass or calcification. Nine months later: subcutaneous, hyperechoic lesion at 6.5cm; increased blood flow to the hyperechoic area | Not completed. | Nine months later: mass with dimensions of 7.7×6.9×3.2 cm; T1 and T2 intensity type 1 kinetic curve in the right breast; Linear region of intensity extending from the right upper inner breast to left upper inner breast | Not completed | Fat lobule necrosis; mixed lymphoplasmacytic and histiocytic aggregates; granulomas; vasculitis | Corticosteroids; hydroxychloroquine leading to complete remission |
| Taslicay et al. [ | 58 F | Not reported | 11 years | DLE | ANA elevated | Subareolar area of the left breast | Palpable mass and swelling of the left breast. Two years later: the patient was not adherent to medications presented again with painful palpable masses in the left breast and left arm | Diffuse edema; irregular hypoechoic areas; acoustic shadowing | 8 cm mass in the subareolar area of the left breast; skin thickening; diffuse axillary lymphadenopathy. Two years later: skin thickening; newly developed focal asymmetry; diffuse microcalcification; slight regression in the previous focal asymmetry | Fat necrosis; irregular heterogeneous, and rim-enhancing fat-containing masses. Two years later: T1 and T2 hyperintense fat-containing multiple masses with heterogeneous and rim enhancement indicating fat necrosis | Focal masses with increased densities, areas of fat necrosis. Two years later: fat necrosis | Lymphocytic. perineuronal, perivascular, and periductal lymphoid infiltrates; mononuclear cell infiltration with germinal center formation; hyaline-type fat necrosis; lymphocytic vasculitis | Patient used hydroxychloroquine, metronidazole, doxycycline tablets, permethrin, and sodium-sulfacetamide during flare ups. Two years later: Restarted on hydroxychloroquine = complete remission with increased microcalcifications |
| Wang et al. [ | 26 F | Not reported | 9 years | SLE | Not reported | Bilateral mass | No physical findings only palpable masses | Irregular hypoechoic areas bilaterally (right breast = 85×13 mm left breast= 52×13 mm); poorly defined borders; coarse, strong echoes; blood flow in the hypoechoic area | Not completed. | Double breast-occupying lesions | Not completed. | Interstitial fibrosis; Vitreous degeneration; fat necrosis; microcalcifications; lymphocyte infiltration around the lobules and stroma of both breasts | Hydroxychloroquine, corticosteroids |
| Pimentel et al. [ | 35 F | Not reported | Not reported | SLE | Not reported | Right outer lower breast | Swollen hardened breast | Lobulated vascularized 5 cm mass with liquid areas | Not completed | Not completed. | Not completed. | Perilobular and periductal lymphoid infiltrate; lymphocytic vasculitis | Hydroxychloroquine, prednisolone remission in one month |
| Oktay et al. [ | 37 F | Not reported | No previous diagnosis | Diagnosed with SLE following presentation | Hemoglobin = 10.9 g/dL; white blood cells = 2,690/mm3; neutrophils = 53.5%; platelets = 127,000/mm3, anti-ribosomal antibodies positive, ANA positive | Bilateral breasts | Palpable breast masses | Axillary lymphadenopathy Ill-defined isoechoic masses, with acoustic shadows; Dystrophic calcifications | Diffuse calcifications indicating fat necrosis | Not completed | Not completed | Not completed | Hydroxychloroquine, corticosteroid |
| Jimenez-Anton et al. [ | 50 F | Not reported | No previous diagnosis | No previous diagnosis | ANA titer= 1/160 | Right breast | Erythema, scales, and periareolar excoriation | Not completed | Not completed | Not completed | Not completed | Epidermal atrophy; perivascular lymphocytic infiltrate; vacuolar degeneration of the basal layer; accumulation of mucin; lupus band with linear IgG deposits; IgM deposits in the dermal-epidermal junction | Hydroxychloroquine, corticosteroid remission after one year |
| Mazeda et al. [ | 34 F | Not reported | Not reported | SLE | Not reported | Right lower outer quadrant. One year later: Bilateral lesion | Hard, tenderness, warmth | Irregularly defined lobulated mass; Vascularized mass 5 × 5 cm in size | Not completed | Not completed | Not completed | Fibrotic areas; abscesses; ductitis lesions; lymphatic lobulitis; vasculitis | Initial treatment: NSAID, antibiotics. Two weeks later: hydroxychloroquine, prednisolone. One year later: rituximab then reaching remission |
| Sharma et al. [ | 42 F | Not reported | No previous diagnosis | No previous diagnosis | Not reported | Bilaterally | Pain, tenderness | 14 × 11 × 8-mm oval mass; hyperechoic | Not completed | Not completed | Not completed | Fat necrosis; Mixed nodular lymphoplasmacytic and histiocytic aggregates; Karyorrhectic debris; fibrinoid necrosis; microcalcifications; histiocytes positive for CD68 staining | Corticosteroids remission in three months |
| Tanaka et al. [ | 46 F | Not reported | 20 years | SLE | Not reported | Right breast middle-inner | Firmness, crusting of skin | Skin thickening; Diffuse hypoechoic area with calcifications | Coarse calcification | Skin thickening; Skin atrophy; Diffuse enhancement effects of the right mammary gland | Not completed | Lymphocytic infiltration | None, follow-up observation |
| Vilas-Sueiro et al. [ | 60 F | Not reported | 3 years | DLE | ANA titers 1:80 positive DsDNA 1:10 positive | Lower central left breast | Deep and firm erythematous subcutaneous nodule, no skin changes, | Increased density and irregular breast tissue, skin thickening | Not completed | Not completed | Not completed | Lymphocytic infiltration; Hyalinized fat necrosis; IgA, IgG, IgM, and C3 granular deposition | Hydroxychloroquine |
| Voizard et al. [ | Case 1: 64 F Case 2: 66 F | Case 1: White Case 2: White | Case1: No previous diagnosis Case 2: No previous diagnosis | Case 1: No previous diagnosis Case 2: No previous diagnosis | Case 1: Six months later: elevated ANA | Case 1: Upper central right breast. Case 2: Inferior central right breast | Case 1: Skin thickening, erythematous/blue discoloration. Six months later: Extensive cutaneous lesions. Case 2: Erythema, mass in inframammary fold | Case 1: Diffuse hyperechogenic, skin thickening. Six months later: Axillary lymphadenopathy. Case 2: Skin thickening, non-specific hyperechoic infiltration of the subcutaneous fat and parenchyma | Case 1: Trabecular thickening. Six months later: Skin and trabecular thickening. Case 2: mild skin thickening in the right inframammary fold | Case 2: Skin thickening with enhancement of the dermis and subdermal regions | Not completed | Case 1: Hyaline fat necrosis; Lymphocytic infiltration in lobules and stroma; CD3-positive T-lymphocytes; CD20-positive B-lymphocytes. Six months later: perivascular and periductal non-specific lymphocytic infiltrate Follicular hyperplasia in lymph nodes. Case 2: Lymphoplasmacytic perineural infiltration; lymphocytic vasculitis in the deep dermis; hyalinization and sclerosis of adipose tissue and deep dermal mucin deposition | Case 1: Hydroxychloroquine. Case 2: Spontaneous remission |
| Thapa et al. [ | 39 M | Not reported | No previous diagnosis | Diagnosed with DLE following presentation | SSA/Ro positive ANA titer (1:40) positive | Bilaterally. Left supra-areolar region. Right upper outer quadrant | Tender, subcutaneous masses | Hyperechoic; Internal vascularity; 25 × 7 mm in the left breast and 22 × 9 mm in the right breast | Bilateral dense masses ; 3 × 3 cm mass in the left breast; 2 × 2 cm mass in the right breast | Fat stranding with overlying skin thickening hyperintense on T2 weighted; 29 × 24 mm mass in left breast; 13 × 8 mm mass in right breast; Heterogeneous enhancement; Type I kinetic enhancement curves | Not completed | Lymphoplasmacytic cell infiltration; Sclerosis; Intimal edema; Lymphocytic infiltration | Hydroxychloroquine, prednisolone |
| Kim et al. [ | 65 F | Not reported | Not reported | CLE | Not reported | Right breast upper outer area | Skin thickening | Focal asymmetry in the inner breast and upper outer quadrant, skin thickening | Not completed | Not completed | Not completed | Not completed | Not reported |
| Kinonen et al. [ | Case 1: 58 F Case 2: 52 F | Case 1: African American Case 2: African American | Case 1: 10 years Case 2: Not reported | Case 1: SLE Case 2: DLE | Not reported | Case 1: Right upper breast. 1 year later: Upper center left breast. Case 2: Left upper and central breast | Case 1: Firm, palpable mass | Case 1: Ill-defined, hyperechoic, 2.6-cm lesion, vascularity. One year later: Similarly to initial presentation | Case 1: Ill-defined, soft tissue density. 1 year later: Similarly to initial presentation. Case 2: Focal irregular density, microcalcifications | Not completed | Not completed | Case 1: Hyaline fat necrosis; Lymphocytic infiltration in subcutaneous fat, with germinal center formation; CD20+ B-cell follicles; CD3+, CD5+, CD4+, CD8+ T cells. 1 year later: Lymphoplasmacytic infiltrate of lobules and septa with vascularity. Case 2: lymphocytic infiltration of the adipose tissue in perivascular and periductal regions | Case 1: Hydroxychloroquine Case 2: Not reported |
| Lucivero et al. [ | 47 F | Not reported | 10 years | SLE | SSA/Ro Antibody positive | Upper and lower quadrants of right breast | Firm, painless mass | Irregularly defined vascularized; Hypoechoic nodule 15 mm | Not completed | Not completed | Not completed | Dysplastic ductal cells; Macrophages with a foamy cytoplasm; Necrosis of adipose tissue; Chronic granulomatous inflammation; Mammary gland dysplasia with simple cysts that are coated with flattened epithelial ductal cells; Dense aggregates of lymphocytes and monocytes with plurinucleate giant cells; Stromal fibrosis; Hyaline degeneration; Vascularity in basal structures; Increased thickness of blood vessels; CD20-positive B lymphocytes; IgG-secreting plasma cells; Few CD4 and CD8 T cells; CD68-positive monocytes and macrophages; C3 in vascular and epithelial basal membranes | Previous episodes of LM treated with antibiotics and anti-inflammatory medications, no specified. Current treatment for flare up, not mentioned. |
| Wang et al. [ | 28 F | Not reported | 13 years | SLE | Not reported | Bilaterally | Bilateral mastalgia; lump sensation | Ill-defined; hypoechoic areas | Multifocal, coarse calcifications | Not completed | Not completed | Coarse dystrophic calcification; Fatty necrosis; perivascular lymphocyte infiltration | Corticosteroids remission within one week |
| Mosier et al. [ | 40 F | African-American | 20 years | DLE | Not reported. | Left breast | Painful, palpable | Dystrophic calcifications | Coarse; central calcifications | Hypointense; coarse calcifications; irregular; thick rim of enhancement | Not completed | Hyalinization; Lymphocytic inflammation; necrosis | Hydroxychloroquine with topical steroids |
| Warne et al. [ | 34 F | Not reported | 7 years | SLE | Not reported | Right breast upper outer | Swelling and pain. Two years later: Patient returned with swelling and pain and peau d’orange with no palpable mass | Irregular hypoechoic mass; Diffusely oedematous. Two years later: 7 cm mass in the upper outer quadrant; breast edema; axillary lymphadenopathy | Increased density | Not completed | Not completed | Hyaline fat necrosis; calcification; aclerosis; Lymphocytic infiltrates in the Periductal, perivascular and perilobular; Lymphocytic vasculitis; interstitial fibrosis. Two years later: Similar findings to initial biopsy | The patient developed Pseudomonas infection at the biopsy site as a result steroids were not recommended and the patient was started on antibiotic only |
| Wani et al. [ | 24 F | Not reported | 13 years | SLE | Normochromic normocytic anemia; Leucopenia; Albumin = 2.6 gm/dl; Mild elevation of transaminases; ESR = 115 mm; serum ferritin level = less than 2000 μg/ dl. | Left breast three months later: Right breast | Palpable lumps in the left breast, largest reported to be 4x3cm with axillary lymphanopathy. Three months later: Pain and swelling in right breast; Lumps reported in both breasts | Diffuse calcifications; Acoustic shadowing | “Unusual” calcifications | Not completed | Calcifications in breasts | Degenerated fat cells; lymphocytes; foci of calcification | Observed |
| Fernendez-Flores et al. [ | 42 M | Not reported | No previous diagnosis | Did not meet criteria for diagnosis all antibodies negative | Not reported | Left breast | Diffuse moderate enlargement of the left breast with a red; scaly plaque around the nipple | Not completed | Not completed | Not completed | Not completed | Mixed lobular and septal lymphocytic panniculitis; lymphocytic infiltration with lymphoid follicles; vasculitis; vacuolar alteration with a smudge appearance along the dermoepidermal junction; thickened basement membrane; mixed population of B cells-CD20+; T cells -CD3+, CD4+, and CD8– and histocytes -CD68+; polyclonal rearrangement of IgH, CDR2, CDR3, and TCR-gamma | Not reported |
| Arsenovic et al. [ | 33 F | Not reported | 3 years | SLE | WBC= 11.2×109/L; ESR= 46-80mm/h; dsDNA antibody level elevated =98 IU/mL; Urea=9.5mmol/L; Creatinine=156 µmol/L | Right upper quadrant breast | Tenderness and firm lump with a fluctuant center, 7×5×3.5 cm | Heterogeneous mass with multifocal; coarse calcifications; Poorly defined margins | Not completed | Not completed | Not completed | Atrophic epidermis; fat necrosis; lymphocytic infiltrate; microcalcification; fibrinoid necrosis; mononuclear inflammatory infiltrate; lymphocytic vasculitis | Prednisone |
| Sanders et al. [ | 31 F | African American | No previous diagnosis | Did not meet criteria for diagnosis | Not reported. | Right upper outer quadrant | Painless palpable thickening and erythema of the skin | Skin thickening; subcutaneous hyperechogenicity without a focal mass | Skin thickening; Increased subjacent stromal density; lymphadenopathy | Extensive skin thickening in the right; moderate persistent and plateau enhancement (Type I⁄II kinetics); bilateral axillary and subpectoral lymphadenopathy | Not completed. | Atrophic changes; segmental perivascular lymphoplasmacytic infiltrate of the deep dermal arteries; hyaline fat necrosis | Not reported |
| Fernandez-Torres et al. [ | 57 F | Not reported | No previous diagnosis | No previous diagnosis | Not reported | Left breast | Erythematous plaque; ill-defined; orange-peel; rubbery; deep; stone-like areas; superficial telangiectasia; intense atrophy | Not completed | Conducted no abnormalities noted | Not completed | Not completed | Lymphocytic vasculitis; Lymphocytic infiltrate forming lymphoid follicles with germinal centers; fibrinoid degenerative; coarse calcifications in the reticular dermis | Oral antimalarials initiated but, shortly discontinued due to adverse reaction and began on Dapson |
| Crevitis et al. [ | 39 M | Not reported | No previous diagnosis | Diagnosed with DLE following workup | Anti-SSA positive ANA titer of 1:40 | Bilateral; left supra-areolar region; right upper outer quadrant | Tender subcutaneous masses 3x3cm and 2x2cm | Ill-defined, hyperechoic; Subcutaneous mass with internal vascularity measuring 25 × 7 mm in left and 22 × 9 mm in the right | Ill-defined; dense mass | Focal areas of marked fat stranding with overlying skin thickening measuring 29 × 24 in the left and 13 × 8 mm in the right; areas marked as hyperintense on T2 weighted fat-suppressed sequence; Heterogeneous enhancement; type I kinetic enhancement curves | Not completed. | Fibrofatty infiltrated with lymphoplasmacytic cells arranged in a lobular and focally septal distribution; Sclerosis; intimal edema; lymphocytic infiltration | Prednisolone and hydrochloroquine |
| Georgian-Georgian-Smith et al. [ | 44 F | Not reported. | 16 years | SLE | Not reported | Left breast | Painful, erythema | Not completed | Curvilinear and coarse calcifications; Fat necrosis; Diffuse increased density of fibroglandular tissues | Not completed | Not completed | Necrotizing vasculitis; Fat necrosis Microcalcifications; mixed population of T and B lymphocyte; Perivascular lymphocytic infiltrate; dense stromal fibrosis; microcalcifications | Prednisone but could not tolerate medication eventually lead to a mastectomy due to severe pain |
| Bachmeyer et al. [ | 30 F | Not reported | 11 years | DLE | Not reported | Right breast | Painful, erythema | Not completed | Curvilinear and coarse calcifications | Not completed | Not completed | Deposits of IgG, IgM, and C3 along the dermoepidermal junction; Lymphocytic infiltrate; Voluminous calcifications | Prednisolone and hydroxychloroquine |
| Nigar et al. [ | 40 F | Not reported | 12 years | SLE | Elevated ANA titers 1:5120; Elevated anticardiolipin antibodies; Anti-SS-A positive | Right breast | Tender, lump. | Eight years later: low echogenicity; minimal vascularity | 1 year later: 20-mm irregular mass | Not completed. | Not completed. | One year later: dense lymphoid infiltrates Reactive lymphoid follicle; Fibrosis; Densely hyalinized breast stroma with ‘onion-skin’ type of concentric fibrosis around the local vessels and into breast ducts and lobules; Focal hyaline fat necrosis. 8 years later: Dense lymphoplasmacytic infiltrate | Not reported |
| Carducci et al. [ | 62 F | Not reported. | No previous diagnosis | Diagnosed with DLE following workup | ANA titer of 1:40 | Right breast upper quadrant | Painful, erythema, nodules | Skin thickening; hyperechoic; poorly defined; Absence of flow signal | Increased density; hypodiaphania | Not completed | Not completed | Fat necrosis | Antimalarials |
| Chen et al. [ | 29 F | African- American | Not reported | SLE | Lupus anticoagulant positive | Left breast, upper inner quadrant | Round, nontender, 5 cm nodule | Ill-defined; isoechoic; heterogeneous mass | Not completed. | Not completed | Not completed | Lymphocytic infiltration; plasma cell infiltrates | Not reported |
| Sabate et al. [ | 33 F | White | 7 years | SLE | Not reported. | Left breast, upper quadrant | Nontender, fixed, mass | Echogenic mass with ill-defined margins; Skin thickening | 2-cm irregular mass; Ill-defined margins involving the subcutaneous fat pad of the left breast; Skin thickening; Subtle retraction on the adjacent superficial parenchymal gland | Heterogeneous mass involving the subcutaneous fat pad with a peripheral zone of low signal intensity and a central area of high signal intensity Irregular margins; Rim enhancement; Skin thickening; Subtle parenchymal distortion | Not completed. | Hyaline necrosis; fat necrosis; perivascular lymphocytic inflammation; vasculitis | Corticosteroids |
| Physical findings | Ultrasound findings | Mammogram findings | MRI findings | CT findings | Biopsy findings |
| Skin thickening; erythematous; palpable mass; ulceration; lymphadenopathy; edema; scaling; crusting; warmth; excoriation; firmness; rubbery; stone-like; peau d’orange; cutaneous lesions; atrophy; telangiectasia [ | Hyperechoic lesion; hypoechoic lesion; isoechoic lesion; irregular; ill-defined; axillary lymphadenopathy; focal asymmetry; poorly defined borders; lobulated; vascularization; skin thickening; calcifications; edema; acoustic shadowing; strong echoes [ | Skin thickening; trabecular thickening; axillary lymphadenopathy; calcifications; increased density [ | Type 1 kinetic curve; fat necrosis; T1 and T2 hyperintensity; rim-enhancing lesions; skin thickening; skin atrophy; diffuse enhancement; heterogeneous enhancement; fat stranding; hypointensity; calcification [ | Increased density; fat necrosis [ | Fat necrosis; lymphoplasmacytic aggregates; lymphocytic infiltration; histiocyte aggregates; mononuclear cell infiltration; macrophages with a foamy cytoplasm; dysplastic ductal cells; mammary gland dysplasia with simple cysts; lymphoid follicles with germinal centers; vasculitis; granulomas; interstitial fibrosis; stromal fibrosis; calcification; epidermal atrophy; hyalinization; sclerosis; ductitis lesions; karyorrhectic debris; vacuolar alteration with a smudge appearance; accumulation of mucin; IgG, IgM, IgA deposits; C3 deposits; CD68 monocytes and macrophages; CD3, CD4, CD5, CD8 t cell deposit; CD 20 b cells deposit [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Lupus Erythematosus Research · Herpesvirus Infections and Treatments · Hair Growth and Disorders
Introduction and background
Lupus mastitis (LM) is a rare manifestation of systemic lupus erythematosus (SLE), resulting in an inflammatory process within the breast tissue. In 1883, Kaposi first described lupus panniculitis, a condition characterized by inflammation in the deep subcutaneous layer of the skin, leading to nodules or plaques [1,2]. LM is an uncommon presentation of lupus panniculitis in breast tissue. LM is commonly seen in patients with diagnosed SLE or discoid lupus erythematosus (DLE); however, rarely, LM may be the initial presentation of SLE or DLE before official diagnosis [3,4]. LM can present as single or multiple subcutaneous masses, unilaterally or bilaterally, which may be painful or palpable. The overlying skin can be unaffected or exhibit atrophy, lipoatrophy, hypertrichosis, hyperkeratosis, ulceration, erythema, thickening, scaling, and lesions [5,6]. Histologically, it most commonly presents with lymphocytic infiltrates and fat necrosis.
Given the higher prevalence of autoimmune conditions in women, LM is more commonly observed in middle-aged premenopausal women, typically around 40 years old. However, it can affect individuals between 18 and 70 years old, with significantly fewer cases reported in men [5,7]. In the literature, only five reported cases of LM occurred in men from 1983 to 2016 [8-12].
Due to the rarity of LM, incidence is often based on the finding of lupus panniculitis, which refers to inflammation of the subcutaneous fat and occurs in 2-3% of patients with SLE. LM is a subset of lupus panniculitis only affecting the breast tissue. There is currently no definitive incidence rate for LM [13,14].
The pathophysiology of LM is yet to be concretely discovered. Hypotheses believe that the inflammatory process of both the adaptive and innate immune systems impacts the skin overlying the breasts, resulting in visual changes from erythema, scaling, atrophy, ulcerations, and lesions. This theory is further supported by the presence of immune complexes, immunoglobulins of IgA, IgG, IgM, and complement factors of C3 and C4 within the basement membrane of the dermal-epidermal junction and blood vessels. This is the most supported hypothesis, as patients have been found to improve with the use of anti-inflammatory medications, including corticosteroids [3-6,15]. Some patients exhibit no visible breast changes, which is attributed to vasculitis [16]. Furthermore, trauma to the affected site through a biopsy is thought to worsen the condition and is advised to be avoided if diagnoses could be made through non-invasive imaging [5,17]. There is no current evidence linking LM with any other subsequent disease manifestation of lupus, such as lupus nephritis, as the pathophysiology significantly differs.
While certain medications can induce SLE, there is no direct evidence linking these medications to the development of LM. LM is more likely to occur in the context of pre-existing SLE or DLE rather than being directly induced by certain medications. The literature primarily focuses on the systemic effects of drug-induced lupus, which typically includes musculoskeletal symptoms, serositis, and skin manifestations, but does not specifically address LM. Therefore, while these drugs can induce SLE, their role in causing LM remains unsubstantiated [18,19].
Due to the heterogeneous presentation of LM, clinicians consider differential diagnoses for patients at the time of presentation, including medullary breast carcinoma, inflammatory breast carcinoma, diabetic mastopathy, subcutaneous panniculitis-like T-cell lymphoma, and granulomatous mastitis. Therefore, histopathology is crucial to proper diagnoses [7,15].
Despite its clinical significance, LM remains poorly understood, and no standardized diagnostic guidelines currently exist. This study aims to bridge this gap by analyzing reported cases of LM to identify common clinical and imaging findings and propose a diagnostic framework for clinicians. We also recommend modifying existing clinical guidelines to acknowledge that an LM diagnosis fulfills the criteria for an SLE diagnosis, regardless of whether the additional requirements outlined in current guidelines are met.
Review
Methods
Search Strategy
A systematic review was conducted using OVID, EMBASE, and Web of Science using the search term of only “Lupus mastitis.” To ensure the relevancy of the articles, those published between 2000 and 2024 were assessed to ensure that a larger number of studies could be reviewed due to the rarity of this condition. The articles were analyzed in a step-wise process, first evaluating the title, abstract, and study design. Full texts were then used to analyze the availability of articles and ensure patients who only had LM without a secondary autoimmune condition were analyzed. Nova Southeastern University’s library database was used to access databases and full-text articles.
Selection Criteria
The study designs included only case studies. Exclusion criteria included study designs of literature, systematic or scoping reviews, randomized control trials, cross-sectional studies, observational studies, cohort prospective/retrospective studies, and animal studies. Abstracts without full text were excluded to limit the analysis to fully described patient characteristics and associated imaging. Articles were removed if the patient had a secondary autoimmune condition or pregnancy to limit confounding variables and articles that discussed other forms of mastitis. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) were used to develop a flow diagram of the selection criteria for reproducibility (Figure 1) [20].
PRISMA flow diagram for selection criteria PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Results
In total, 255 articles were populated between the databases of OVID, EMBASE, Web of Science and CINHAL, with 30 articles being selected after first and second-tier screening. Table 1 indicates the characteristics of the 32 patients with LM that were analyzed among the articles; 29 (90.6%) were female, with only three (9.4%) being seen in male (Figure 2). The age ranged from 24 to 66 years old, with a mean age of 44. Twelve patients were not previously diagnosed with any form of lupus at the time of presenting with LM. Following a diagnosis of LM, four of the 12 patients were diagnosed with lupus (one SLE, three DLE). Out of the remaining studies with previous diagnosis, 15 reported disease duration with a range of 3 to 20 years, and the mean duration was 10 years. Ethnicity was reported in only nine of the studies (one Asian, three White, and five African-American).
Comparison of female to male patients
Of the patients who were previously diagnosed, five were diagnosed with DLE, 14 with SLE, and one with CLE (Figure 3). Figure 4 represents the location of the initial breast lesions, with 16 (50%) on the right breast, 10 (31.2%) on the left breast, and 6 (18.8%) bilaterally.
Type of lupus diagnosis among those with previous diagnosisSLE: Systemic lupus erythematosus; CLE: cutaneous lupus erythematosus; DLE: discoid lupus erythematosus
Location of lupus mastitis
The exact location within the breasts varied greatly, with masses in the right breast found in the upper inner, upper outer, upper central, lower central, lower outer, and middle inner quadrants versus those in the left breast seen in the subareolar, supraaerolar, lower central and upper central quadrants. Table 2 summarizes the common physical presentations of LM from the studies analyzed within ultrasound, mammogram, MRI, CT, and biopsy.
Figures 5, 6 show the LM images that visually depict common findings of calcification and fibrotic changes characteristic of the condition [43].
Oblique lateral (A) and craniocaudal (B) mammograms showing coarse and diffuse calcifications within lupus mastitis (red arrows)Image credit: Magalhaes et al. [43] (licensed under Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License; http://creativecommons.org/licenses/by-nc-sa/4.0/)
Breast ultrasound indicating fibrotic changes in the glandular tissue and a coarse calcification (red arrow)Image credit: Magalhaes et al. [43] (licensed under Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License; http://creativecommons.org/licenses/by-nc-sa/4.0/)
Discussion
LM is a subset of lupus panniculitis that impacts the subcutaneous layer of the breast as well as the mammary glands. LM is a rare condition that usually occurs in those with a previously established diagnosis of SLE or DLE; however, it rarely can also be the initial presentation [6].With its heterogeneous presentation, clinicians are unaware of this subsequent condition that can arise with a lupus diagnosis, as more prominent conditions often overshadow it.
In the diagnosis of LM, all cases received a combination of ultrasound, mammography, MRI, and rarely CT. Due to LM presenting physically similar to breast malignancy, it is crucial to make that differentiation. Non-invasive ultrasounds were encountered to be the most commonly utilized initial imaging. Ultrasound findings included hyperechoic, hypoechoic and isoechoic lesions with poorly defined borders, the masses are described as irregular, lobulated, or oval with acoustic shadowing, coarse strong echoes, and associated features of edema, increased vascularization, and skin thickening. Mammograms demonstrated ill-defined masses with high density, focal asymmetries, diffuse, coarse, or micro calcifications, and associated features of axillary lymphadenopathy on the side of insult and skin thickening. MRI findings included a type 1 kinetic curve correlating to benign findings, fat necrosis, rim-enhancing lesions, and diffuse and heterogeneous enhancement. The diagnosis of LM can become complicated as rim-enhancing lesions and heterogenous enhancement are both characteristics of malignancy. As a result, a previous diagnosis of lupus can help guide the diagnosis to LM [44,45]. Suspicious findings were deemed BIRADS 4 and biopsies were done following imaging, with more common pathological findings of lymphocytic, histiocytic, mononuclear cell infiltration, sclerosis, fibrosis, vasculitis, accumulation of mucin, and deposition of immune complexes. Lymphocytic infiltration has been deemed to be a key feature of LM; however, it is also commonly found within diabetic mastopathy. A key differentiating feature is that in LM, it is present in the lobules and is more profuse [5,7,35].
There are currently conflicting verdicts on the use of biopsy. Biopsies are not recommended unless imaging is inconclusive, as trauma to the site has been correlated to flare-ups; however, in almost all of the patients, biopsies were utilized following imaging [35,46]. This raises the question of the lack of consensus regarding diagnostic criteria for LM, resulting in the continuous use of biopsy to confirm the findings. However, some clinicians believe that the diagnosis of this condition should be conservative through clinical features, and imaging is sufficient to develop the diagnosis [16,47]. Surgical removal of the mass is further deemed unnecessary and was not completed in any of the studies analyzed. In the sparse cases in which gross examination was conducted, the masses were described as well-circumscribed, lobulated, irregular cavities with greasy liquid-filled, pink-tan nodular areas, yellow-tan adipose tissue with fibrous tissue, and white-tan induration [4,5].
Interestingly, six patients were not diagnosed with any form of lupus at the time of presentation. The reason for this matter can be due to LM not being a diagnostic criterion identified by the American College of Rheumatology. In order to be diagnosed with SLE based on the EULAR/ACR 2019 criteria, a score of above 10 is required, and an isolated incident of LM does not meet any criteria [48]. Furthermore, these patients may be in the preclinical stage of lupus with LM as an isolated symptom without yet meeting the rest of the criteria.
Currently, no leading organization or committee has established published diagnostic criteria specifically for LM. Due to its heterogeneous presence and lack of guidance for clinicians, the diagnosis of LM is complex. LM is often misdiagnosed if it presents as firm, hard, palpable masses, or the calcifications seen within imaging can initially raise alarms for malignancy. Establishing precise diagnostic criteria is crucial to avoid unnecessary surgery and psychological worry among patients [7]. Through analyzing the case studies, we propose the first diagnostic and management guidelines and the following steps for the diagnosis of LM (Figure 7).
Suggested diagnostic management for LMSLE: Systemic lupus erythematosus; CLE: cutaneous lupus erythematosus; DLE: discoid lupus erythematosus; LM: lupus mastitis
We also propose adapting current clinical guidelines to include the fact that a diagnosis of LM does satisfy the criteria of an SLE diagnosis with or without meeting the additional requirements required by established clinical guidelines. Similarly, after a renal biopsy indicates lupus nephritis, those patients are then subsequently diagnosed with lupus even if they do not meet the remaining (i.e. SLICC, ACR, EULAR) criteria. We propose a similar action be taken with LM. Thirty-six percent of patients were diagnosed with LM without having a previous diagnosis of lupus, and only four out of the 12 patients met diagnostic criteria for lupus, while the other eight did not but still had LM. The question is raised of how a patient could be diagnosed with LM without meeting the established criteria as a result, we believe they should be subsequently diagnosed with lupus and/or monitored to assess for subsequent development of SLE. Furthermore, we recommend patients who have not met established criteria for diagnosis to still be connected with a rheumatologist and follow up yearly, as LM may be the initial presentation of the condition that may present additional symptoms in the years to come. None of the case studies did follow-ups on the patient to monitor this phenomenon to see if they met lupus criteria later on as a result long-term and prospective cohort studies are recommended.
The link between LM and traditional biomarkers of ANA, anti-dsDNA, anti-Sm, anti-histone, and complement factors of C3 and C4 is unclear in the literature. Only one external study analyzed these factors within “non-lactational mastitis,” but the patients did not meet the criteria for lupus. Within the case studies analyzed, a variety of biomarkers were analyzed, those found to be elevated amongst the patients included ANA, lupus anticoagulant, dsDNA antibodies, anti-SSA antibodies, anticardiolipin antibodies, and elevated IgA and IgG levels [6,9,13,15,22,25,26,40,41,49]. Additional biomarkers of interferon-alpha, IP-10, SIGLEC-1, CCL8, CXCL13, and IL-1 RA have been identified as biomarkers to indicate inflammatory states within SLE, but none have been investigated thus far in LM. Further research is required within the LM population to develop a clear understanding of the influence of lupus biomarkers; as patients are being diagnosed with LM without having elevated biomarkers, we recommend LM to be enough of an independent factor to diagnose a patient with lupus.
LM is a chronic disease that can result in remissions years later, as seen in almost 30% of the patient cases analyzed or if misdiagnosed, lead to prolonged care or disfigurement of the breast [3,5,6,21,22,27,34]. Lupus panniculitis which is the inflammation of the subcutaneous layer of the skin only requires corticosteroids either topically or as an injection; however, LM generally requires an anti-malarial medication of hydroxychloroquine that may be given individually or combined with steroids [5,6,11,15,21-27,32,33]. Hydroxychloroquine was first identified to be effective in CLE and has since expanded in its use for SLE [50].
Leading rheumatology organizations have yet to establish the causes and diagnostic criteria for LM. Given its rarity and similarity to malignancy in imaging, official guidelines are needed to assist clinicians in laboratory and imaging assessments
The limitations of this article include the scarce research conducted on patients with LM. As LM is a rare condition, the current evidence only consists of case studies, and there is a lack of primary studies conducted on these patients. Further research must be conducted to understand the underlying cause of LM, as that can guide diagnostic imaging and workup criteria. Furthermore, in patients who developed LM without meeting diagnostic criteria at the moment, research should be conducted to understand what patient characteristics may potentially lead to LM being the initial presentation of lupus in these patients. Finally, little demographic data was provided regarding the patients which should be further evaluated to better understand if a specific group of patients are at higher risk than others as trends are commonly seen within autoimmune conditions.
Conclusions
LM is a complex condition that has been heavily under-researched in today’s literature. It has a heterogeneous presentation, occurs in various age ranges, and has a range of disease durations, and some patients who have not met the diagnostic criteria for SLE or DLE. Understanding this condition further is crucial to monitoring its development ahead of time and tailoring treatment options. A goal of this study was to provide a workflow for the diagnosis of LM and we strive that our recommended clinical guidelines will help provide clarity to clinicians on the imaging procedures to take when approached with the uncommon diagnosis of LM.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pathologie und Therapie der Hautkrankheiten Kaposi M Vienna, Austria Urban & Schwarzenberg 1883 https://archive.org/details/b 2040038 x
- 2Lupus erythematosus panniculitis: clinicopathological, immunophenotypic, and molecular studies Am J Dermatopathol Park HS Choi JW Kim BK Cho KH 24303220102009808110.1097/DAD.0b 013e 3181 b 4a 5ec · doi ↗ · pubmed ↗
- 3Lupus mastitis: a clinicopathologic review and addition of a case Adv Anat Pathol Summers TA Jr Lehman MB Barner R Royer MC 56611620091909846710.1097/PAP.0b 013e 3181915 ff 7 · doi ↗ · pubmed ↗
- 4Lupus mastitis heralding systemic lupus erythematosus with antiphospholipid syndrome J Rheumatol De Bandt M Meyer O Grossin M Kahn MF 12171220201993 https://pubmed.ncbi.nlm.nih.gov/8371223/8371223 · pubmed ↗
- 5Lupus mastitis: an uncommon complication of systemic or discoid lupus Am J Surg Pathol Kinonen C Gattuso P Reddy VB 9019063420102041080910.1097/PAS.0b 013e 3181 da 00fb · doi ↗ · pubmed ↗
- 6Lupus mastitis as a first manifestation of systemic disease: about two cases with a review of the literature Eur J Radiol Voizard B Lalonde L Sanchez LM 1241319220172862401010.1016/j.ejrad.2017.04.023 · doi ↗ · pubmed ↗
- 7Lupus mastitis: a review Ann Diagn Pathol Rosa M Mohammadi A 2302331720132319068110.1016/j.anndiagpath.2012.09.003 · doi ↗ · pubmed ↗
- 8Lupus mastitis in the male breast mimicking inflammatory carcinoma Breast J Fernandez-Flores A Crespo LG Alonso S Montero MG 2722731220061668433010.1111/j.1075-122X.2006.00256.x · doi ↗ · pubmed ↗