Innovative Endoscopic Management of Recurrent Gastrogastric Fistula Post-Roux-en-Y Gastric Bypass Patient Using Cardiac Septal Occluder and Lumen-Apposing Metal Stent
Ajay Gade, Kalpit Devani

TL;DR
A new endoscopic method using a cardiac device and stent successfully treated a rare stomach fistula in a patient who had gastric bypass surgery.
Contribution
Combining a cardiac septal occluder with a lumen-apposing metal stent offers a novel, non-surgical treatment for complex gastrogastric fistulas.
Findings
The fistula was successfully closed using a cardiac septal occluder and lumen-apposing metal stent.
The patient experienced complete symptom resolution after the procedure.
This approach provides a promising alternative to surgery for managing complex GGF cases.
Abstract
Gastrogastric fistula (GGF) is a rare complication of post-Roux-en-Y gastric bypass, often challenging to manage. This case report presents a 63-year-old patient with recurrent GGF and gastrojejunal stricture, refractory to prior endoscopic treatments. Using a minimally invasive approach with atrial septal defect closure device and a lumen-apposing metal stent, the fistula was successfully closed, and stricture relieved. The patient reported complete symptom resolution at follow-up. This innovative approach of combining a cardiac septal occluder and lumen-apposing metal stent for management of complex GGF cases offers a promising alternative to surgical interventions.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
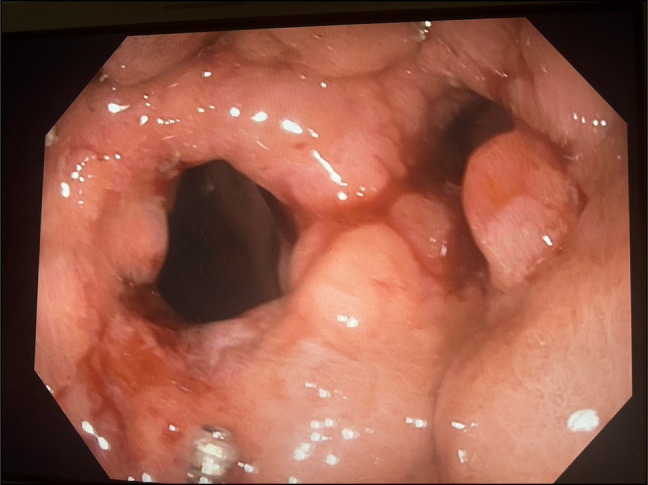 Figure 1
Figure 1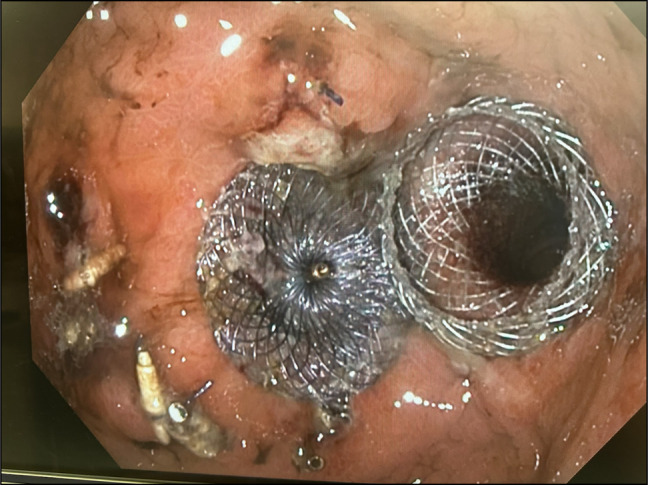 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastroesophageal reflux and treatments · Esophageal and GI Pathology · Congenital Diaphragmatic Hernia Studies
INTRODUCTION
Gastrogastric fistula (GGF) is a rare but significant late complication following Roux-en-Y gastric bypass (RYGB)^1^ associated with abdominal pain, acid reflux, weight regain, and diabetes recurrence. Up to 6% of post-RYGB patients develop GGF requiring endoscopic or surgical intervention.^2^ Endoscopic interventions, though less invasive, can have recurrence especially with concomitant gastrojejunal (GJ) strictures that exacerbate symptoms and complicate management.^1^ This report details the novel use of a cardiac septal occluder (CSO) and lumen-apposing metal stent (LAMS) to manage a recurrent GGF and GJ stricture, offering a minimally invasive solution with promising outcomes.
CASE REPORT
A 63-year-old woman with a history of RYGB performed for class-III obesity presented with recurrent GGF for 4 years. The GGF was identified 5 years after the RYGB surgery. Despite multiple endoscopic treatments, including argon plasma coagulation (APC) and over-the-scope clip placement at an outside facility, her symptoms of abdominal pain, nausea, vomiting, and weight regain persisted.
Upon referral to our facility, she underwent through-the-scope suturing with an X-tack device in a figure-of-8 pattern, achieving temporary symptom relief. However, symptoms recurred within 6 weeks. Follow-up endoscopy revealed GGF recurrence, and she underwent APC ablation (80 W, 1 L/min) and full-thickness suturing with an Apollo endoscopic suturing device. Fistula was successfully closed, and subsequent upper gastrointestinal series confirmed the closure. However, the patient's symptoms recurred, and imaging reconfirmed the fistula.
Repeat evaluation revealed a 14-mm GGF and GJ outlet stricture near the fistulous tract, with residual suture material from prior closures. Initial endoscopies identified a GJ stricture, but prior attempts did not include stricture dilations which led to persistent symptoms and recurrent fistula. We opted for endoscopic closure using an atrial septal defect (ASD) closure device and concomitant GJ stricture management to offload pressure on the fistula for durable closure.
Step-by-step procedure
- Fistula Ablation: APC was applied to the fistula at 80 W with 1 L/min flow to resurface mucosa.
- ASD Closure Device Placement: A 0.035-inch guidewire was introduced into the Roux limb to aid LAMS placement. Considering the fistula size (14 mm), a 16-mm ASD closure device was chosen to avoid occluding the GJ outlet. The device was back-loaded into a double-channel therapeutic scope. Using a rat-tooth grasper, the device was successfully deployed, sealing the fistula with its dual-disc design (Figure 1).
- LAMS Placement: A 15 mm × 10 mm LAMS was deployed over the guidewire, with the proximal flange in the pouch and the distal flange in the Roux limb, ensuring GJ patency (Figure 2).
Showing a fistulous tract between gastric pouch and excluded stomach on the left side. Right side opening is the strictured opening of Gastrojejunostomy.
Showing devices cardiac septal occluder used in closing the fistula (left side) and lumenapposing metal stent (right side) across gastrojejunal anastomosis outlet.
The patient was placed on a liquid diet for 1 week and prescribed omeprazole 40 mg twice daily for 4 weeks. At a 4-week televisit follow-up, she reported complete symptom resolution including no further nausea, vomiting, abdominal pain, or weight gain, with stable glycemic control. She relocated before follow-up endoscopy, leaving LAMS removal pending.
DISCUSSION
The combination of a CSO and LAMS reflects an innovative, minimally invasive approach to managing recurrent GGFs and GJ strictures. GJ stricture management is essential in these cases to reduce pressure on the GGF, a key factor in preventing recurrence.
GGF, an abnormal connection between stomach segments post-RYGB, can lead to weight regain, ulceration, and infection. Its closure is critical.^1^ The CSO, typically used for ASDs or patent foramen ovale, has been repurposed for gastrointestinal applications fistulas.^1^ Its dual-disc structure creates a secure seal, promoting healing and permanent closure.^3^
LAMS, a specialized endoscopic stent, has broad applications, including pseudocyst drainage, bypassing gastric outlet obstructions, and managing leaks or strictures.^3^ Its large lumen ensures effective drainage, while wide flanges prevent migration. For GJ stricture cases, LAMS establishes a durable pathway, reducing fistula pressure, and recurrence risk.^4–6^
This case highlights the successful combination of an Amplatzer Septal Occluder for durable GGF closure and LAMS for maintaining GJ patency. The dual-disc occluder's adaptability ensured effective sealing, while the LAMS addressed stricture-related complications, achieving symptom resolution in a single session.
Prior studies report that the success rate for endoscopic closure of GGF with CSO ranges from 70% to 85%, with complications including device migration and occlusion. LAMS placement for GJ stricture has demonstrated a success rate of approximately 75%–90%, with potential complications such as bleeding, stent migration, and restenosis.^7–10^ The estimated cost of a CSO ranges from 6,000,^11^ while a LAMS device can cost up to $20,000.^12^ While these costs may seem significant, they must be weighed against the potential expense of surgical intervention and hospitalization for recurrent complications.
Combining a CSO with LAMS offers a minimally invasive, effective strategy for recurrent GGFs and GJ strictures post-RYGB. This dual-device approach provided symptom relief, durable fistula closure, and GJ patency. Future studies should explore long-term outcomes to establish this as a viable alternative to surgery for complex GGFs.
DISCLOSURES
Author contributions: A. Gade primarily contributed to conceptualizing the case report, gathering clinical data, conducting the literature review, and drafting the case report and is the article guarantor. K. Devani: Senior author who provided oversight and guidance throughout the preparation of the case report, reviewed the manuscript critically, and ensured its clinical and academic integrity.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alyaqout K Almazeedi S Alhaddad M Efthimiou E Loureiro Md P. Gastrogastric fistula after Roux-en-Y gastric bypass: A case report and review of literature. Arq Bras Cir Dig. 2020;33(2):e 1509.32844882 10.1590/0102-672020190001 e 1509 PMC 7448858 · doi ↗ · pubmed ↗
- 2Dolan RD Mc Carty TR Jirapinyo P Thompson CC. Endoscopic closure versus surgical revision in the management of gastrogastric fistula after Roux-en-Y gastric bypass. i GIE. 2022;1(1):44–8.
- 3Weilert F Binmoeller KF. Specially designed stents for translumenal drainage. Gastrointest Interv. 2015;4(1):40–5.
- 4Binmoeller KF Shah J. A novel lumen-apposing stent for transluminal drainage of nonadherent extraintestinal fluid collections. Endoscopy. 2011;43(4):337–42.21264800 10.1055/s-0030-1256127 · doi ↗ · pubmed ↗
- 5Pandey S Aggarwal N Edhi A Jamil LH. Dislodged lumen-apposing metal stent (LAMS) in EUS-guided gastrojejunostomy salvaged by LAMS-in-LAMS technique. Gastrointest Endosc. 2023;97(4):799–800.36516949 10.1016/j.gie.2022.12.008 · doi ↗ · pubmed ↗
- 6Persaud T Dawod E Shah S Sharaiha R Sampath K. Endoscopic management of gastrojejunocolic fistula after endoscopic gastrojejunostomy. Video GIE. 2022;7(11):395–7.36407038 10.1016/j.vgie.2022.07.010PMC 9669498 · doi ↗ · pubmed ↗
- 7Aziz M Haghbin H Gangwani MK, et al. Efficacy and safety of endoscopic through-the-scope suture system for gastrointestinal defects: A systematic review and meta-analysis. J Clin Gastroenterol. 2024;58:602–6.39008567 10.1097/MCG.0000000000002019 · doi ↗ · pubmed ↗
- 8De Moura DTH Baptista A Jirapinyo P De Moura EGH Thompson C. Role of cardiac septal occluders in the treatment of gastrointestinal fistulas: A systematic review. Clin Endosc. 2020;53(1):37–48.31286746 10.5946/ce.2019.030PMC 7003006 · doi ↗ · pubmed ↗