Pseudoangioedema as a presenting symptom of dermatomyositis with antinuclear matrix protein 2 autoantibodies
Han Li, Steven Svoboda, Kiran Motaparthi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3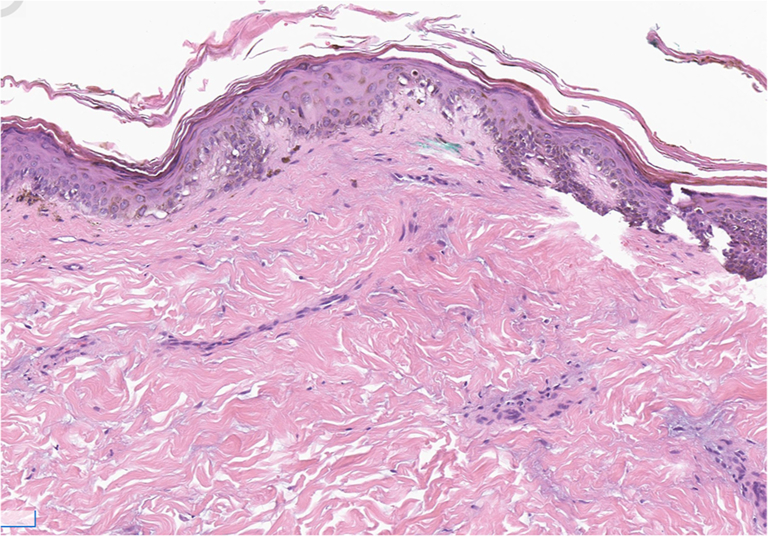 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune Bullous Skin Diseases · Coagulation, Bradykinin, Polyphosphates, and Angioedema · Dermatological and Skeletal Disorders
Introduction
Dermatomyositis (DM) is an inflammatory myopathy with characteristic cutaneous findings of heliotrope rash, Gottron papules and sign, periungual erythema, calcinosis cutis, telangiectasias, and ulcers. DM is associated with several autoantibodies, such as antinuclear matrix protein 2 (NXP-2), antitranscriptional intermediary factor 1, and antimelanoma differentiation-associated protein 5; cutaneous manifestations vary depending upon the associated autoantibodies.1 NXP-2 DM is associated with a higher prevalence of severe myositis, malignancy in adults, and atypical cutaneous findings, which, when present, include calcinosis and subcutaneous edema.2 We present a case of NXP-2 DM presenting with pseudoangioedema of the lips.
Case presentation
A 21-year-old man with no significant medical history presented with 2 months of progressive proximal muscle weakness in upper and lower extremities, lip swelling, dysphagia, and a rash on the upper arms, thighs, neck, chest, and back. The patient denied taking any medications in the months preceding symptom onset. Physical examination was notable for marked edema of the lips (Fig 1) and poikilodermatous plaques on the back, flanks, thighs, and neck and shoulders (Figs 2 and 3). No heliotrope rash, Gottron papules, or nail fold changes were observed. Laboratory findings were significant for a creatine kinase of 3458 units/liter and lactate dehydrogenase of 605 units/liter. Electromyography was consistent with a myopathic process. Histopathology demonstrated a cell-poor vacuolar interface dermatitis with increased dermal mucin and perivascular lymphocytic infiltrate (Fig 4). A myositis antibody panel demonstrated high positivity for anti-NXP-2 antibodies. Computed tomography of the chest and abdomen did not reveal evidence of interstitial lung disease or malignancy, and ultrasound of the scrotum was unremarkable. Computed tomography of the neck showed diffuse intramuscular edema of the prevertebral musculature. Intravenous immunoglobulin was initiated at a dose of 2 g/kg intravenous divided over 4 days and pulse methylprednisolone 1 g intravenous daily for 5 days followed by prednisone at 1 mg/kg with marked improvement in symptoms including edema and dysphagia.Fig 1. Marked edema (pseudoangioedema) of the lips.Fig 2. Flagellate erythema on the upper back.Fig 3. Poikilodermatous to hyperpigmented plaques over the chest, abdomen, flank, and thigh.Fig 4. Cell poor vacuolar interface dermatitis with increased dermal mucin and perivascular lymphocytic infiltrate (H&E, 200× magnification).
Discussion
The features of DM vary depending on the underlying serologic subtype. DM associated with anti-NXP-2 antibodies has a bimodal age distribution, with a 20% to 25% prevalence in juvenile dermatomyositis and a 2% to 25% prevalence in adult DM.3 While anti-NXP-2 DM in older adults is associated with classic features including Gottron papules and heliotrope rash, the juvenile variant is marked by disabling myopathy, calcinosis cutis, and periorbital edema. As an isolated finding, the differential diagnosis of pseudoangioedema of the lips would include granulomatous cheilitis (GC) and disorders associated with GC, such as Melkersson-Rosenthal syndrome, sarcoidosis, and Crohn disease. However, the presenting symptoms and remainder of physical examination findings were characteristic of DM but could not be explained by GC or disorders associated with GC. Anti-NXP-2 DM is strongly associated with malignancy in older adults, with cancer prevalence increasing in an age-dependent manner from below 25% in ages 20-30 up to 55% in ages over 60.4 Interstitial lung disease is relatively rare in anti-NXP-2 DM compared to other DM subtypes.5 The mainstay of treatment comprises glucocorticoids and intravenous immunoglobulin for severe myopathy, with methotrexate and rituximab serving as adjunct therapies or steroid-sparing agents.
Periorbital edema, dysphagia, and generalized subcutaneous edema have previously been described in association with anti-NXP-2 DM.2^,^5^,^6 The mechanism of subcutaneous edema is unknown but is postulated to reflect increased subcutaneous vascular permeability secondary to immune complex deposition and elevated vascular endothelial growth factor expression.7 Pseudoangioedema has been described in association with antimelanoma differentiation-associated protein 5, anti-SAE, and antitranscriptional intermediary factor 1 antibodies but has not previously been reported in anti-NXP-2 DM.8, 9, 10 Pseudoangioedema of the lips is a rare cutaneous manifestation of DM, and this unusual feature may serve as a clue to promote prompt diagnosis.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Okiyama N.Clinical features and cutaneous manifestations of juvenile and adult patients of dermatomyositis associated with myositis-specific autoantibodies J Clin Med 1082021172510.3390/jcm 1008172533923564 PMC 8073628 · doi ↗ · pubmed ↗
- 2Ichimura Y.Konishi R.Shobo M.Anti-nuclear matrix protein 2 antibody-positive inflammatory myopathies represent extensive myositis without dermatomyositis-specific rash Rheumatology (Oxford)61320221222122710.1093/rheumatology/keab 51834152410 · doi ↗ · pubmed ↗
- 3De Wane M.E.Waldman R.Lu J.Dermatomyositis: clinical features and pathogenesis J Am Acad Dermatol 822202026728110.1016/j.jaad.2019.06.130931279808 · doi ↗ · pubmed ↗
- 4Fiorentino D.F.Chung L.S.Christopher-Stine L.Most patients with cancer-associated dermatomyositis have antibodies to nuclear matrix protein NXP-2 or transcription intermediary factor 1γArthritis Rheum 651120132954296210.1002/art.3809324037894 PMC 4073292 · doi ↗ · pubmed ↗
- 5Yan T.T.Zhang X.Yang H.H.Association of anti-NXP 2 antibody with clinical characteristics and outcomes in adult dermatomyositis: results from clinical applications based on a myositis-specific antibody Clin Rheumatol 40920213695370210.1007/s 10067-021-05667-x 33712891 · doi ↗ · pubmed ↗
- 6Fredi M.Cavazzana I.Ceribelli A.An Italian multicenter study on anti-NXP 2 antibodies: clinical and serological associations Clin Rev Allergy Immunol 632202224025010.1007/s 12016-021-08920-y 35092577 PMC 9464148 · doi ↗ · pubmed ↗
- 7Yoshimi R.Nakajima H.Subcutaneous edema in polymyositis and dermatomyositis Intern Med 621520232161216210.2169/internalmedicine.1199-2237532512 PMC 10465285 · doi ↗ · pubmed ↗
- 8Xu X.Huang J.Wang X.Li M.Yang J.Pseudoangioedema in dermatomyositis patients indicates severe disease and poor prognosis J Am Acad Dermatol 862202247447510.1016/j.jaad.2021.09.04334592381 · doi ↗ · pubmed ↗