Diffuse Large B-Cell Lymphoma With Tracheoesophageal Fistula Healed Using Chemotherapy: A Case Report and Review of the Literature
Naoko Yagi, Takuro Yoshimura, Minako Tsutsumi, Takafumi Nakao

TL;DR
A patient with diffuse large B-cell lymphoma and a tracheoesophageal fistula achieved full recovery through chemotherapy without surgery.
Contribution
This is the first reported case of DLBCL-associated tracheoesophageal fistula resolving spontaneously with chemotherapy.
Findings
Chemotherapy led to complete remission of DLBCL and spontaneous resolution of the tracheoesophageal fistula.
No recurrence of lymphoma or fistula was observed 46 months after treatment.
Conservative management with chemotherapy may be effective for lymphoma-associated fistulas.
Abstract
Malignant lymphomas are rarely associated with tracheoesophageal or bronchoesophageal fistulas (TEFs/BEFs). Lymphomas accompanied by TEFs/BEFs have a more favorable prognosis than solid tumors. Here, we present a unique case of a 74-year-old patient with diffuse large B-cell lymphoma (DLBCL). Contrast-enhanced computed tomography (CT) revealed TEF, aspiration pneumonia, and multiple lymphadenopathy. Histopathology helped confirm DLBCL, leading to a Lugano IIE staging. Complete DLBCL remission could be achieved by adjusting chemotherapy dosages for complications, which also resulted in spontaneous TEF resolution without requiring interventions such as stent insertion or surgical correction. No instances of lymphoma recurrence or tracheoesophageal fistula were observed 46 months post-chemotherapy. Among 33 documented cases, this is the first instance of DLBCL-associated TEF resolution…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
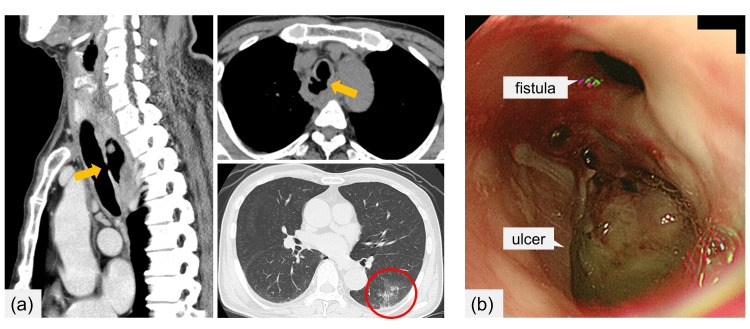 Figure 1
Figure 1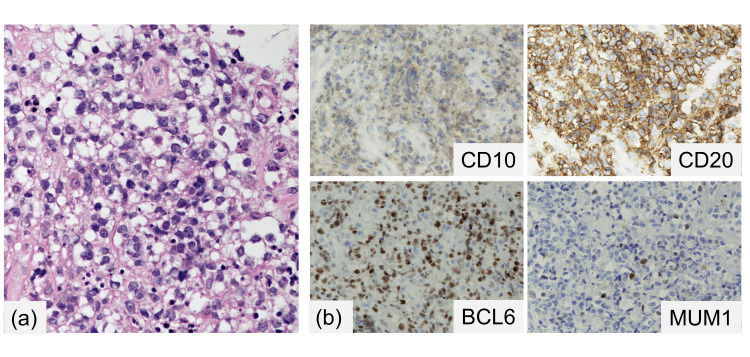 Figure 2
Figure 2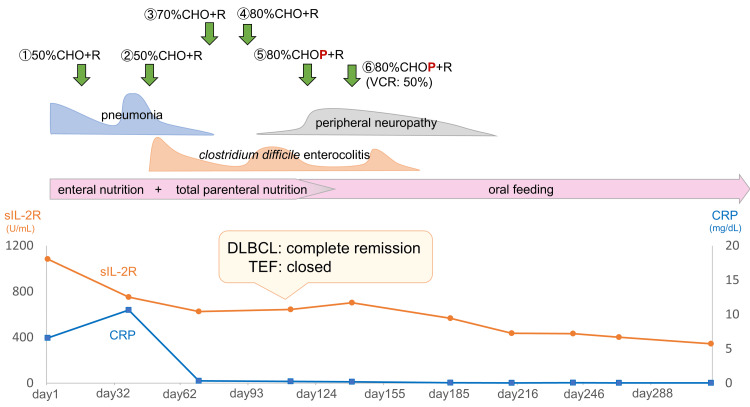 Figure 3
Figure 3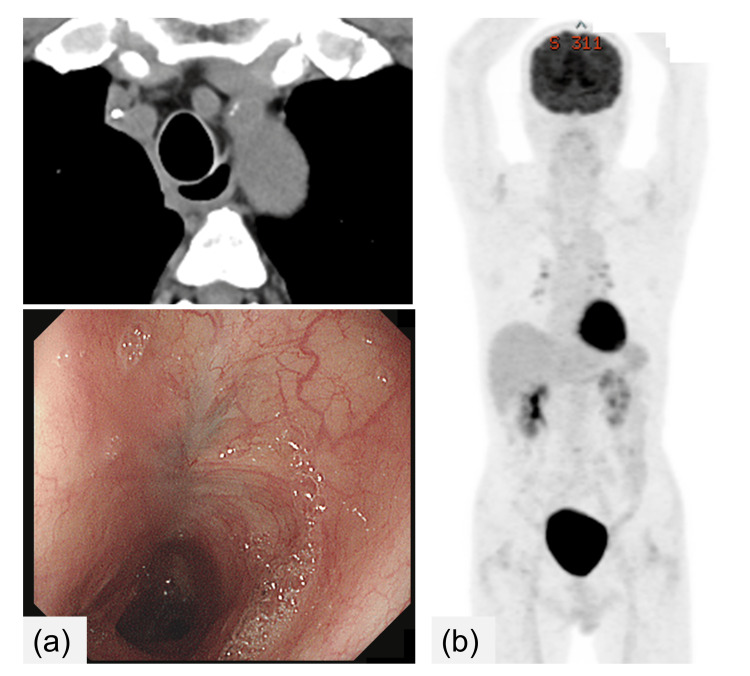 Figure 4
Figure 4| No. | First Author, Year | Age, Gender | Disease Type | Stage | Fistula Locations | Fistula Size (mm) | Time of Fistula Discovery | Treatment for Lymphoma | Management for Fistula | Outcome | Fistula Closure Status | Follow-up Period | |||
| Surgery | Stent Placement | OTSC | Enteral Nutrition | ||||||||||||
| 1 | Sharpe et al., 1992 [ | 55, M | HL | ⅣB | left main bronchus | 4 | after 4th chemo cycle | chemo | yes | (-) | (-) | (-) | remission | artificial closure | 20 mos after initial diagnosis |
| 2 | Greven and Evans., 1992 [ | 25, F | HL | ⅡB | trachea | N/A | at relapse | RT | (-) | (-) | (-) | yes | remission | spontaneous closure | 7 mos post-RT |
| 3 | Alba et al., 1994 [ | 60, F | HL | N/A | right main bronchus | N/A | prior to lymphoma diagnosis | none | (-) | (-) | (-) | (-) | ♰ death (respiratory failure) | persistence | 7 days post-admission |
| 4 | Pac-Ferrer et al., 1994 [ | 15, M | HL | N/A | mid trachea | 15 | during treatment | chemo, RT | (-) | yes | (-) | (-) | progression | artificial closure | N/A |
| 5 | Small et al., 1995 [ | 54, M | HL | IV | left main bronchus | 7 | at diagnosis | chemo (ChlVPP) | yes | (-) | (-) | (-) | relapse | artificial closure | 6 mos post-chemo |
| 6 | Lingand Bushunow., 1996 [ | 47, F | HL | ⅡB | mid trachea | N/A | at relapse | chemo, RT | (-) | (-) | (-) | yes | remission | spontaneous closure | 1 yr post-chemo |
| 7 | Lackner et al., 1996 [ | 32, M | DLBCL | ⅡA | trachea | 8 x 6 | during chemo | chemo (CMOP) | yes | (-) | (-) | (-) | remission | artificial closure | 18 mos post-surgery |
| 8 | Zueger et al., 1997 [ | 56, M | low-grade NHL | ⅠB | left main bronchus | 6 | at diagnosis | chemo (CY/PSL) | (-) | (-) | (-) | yes | remission | spontaneous closure | 2 yrs post-chemo |
| 9 | Jougon and Couraud., 1998 [ | 19, F | NHL | N/A | trachea | 60 | 2 yrs post-chemo | chemo (CHOP) | yes | (-) | (-) | yes | remission | artificial closure | 4 yrs post-surgery |
| 10 | Kassis et al., 1998 [ | 70, M | HL | ⅢB | bronchus intermedius | N/A | at diagnosis | chemo (ABVD) | yes | (-) | (-) | (-) | ♰ death (lymphoma progression) | artificial closure | 8 mos after initial presentation |
| 11 | Fan et al., 2002 [ | 58, M | ALCL | N/A | mid trachea | N/A | post-chemo | chemo, RT | (-) | yes (esophagus, trachea) | (-) | (-) | progression | artificial closure | N/A |
| 12 | Hosoya et al., 2004 [ | 65, M | DLBCL | Ⅳ | trachea | 10 | during first CHOP cycle | chemo | yes | (-) | (-) | yes | remission | artificial closure | 2 yrs post-surgery |
| 13 | Bernal et al., 2005 [ | 33, F | HL | N/A | right main bronchus | 25 | at diagnosis | chemo | (-) | yes (esophagus) | (-) | yes | CR | artificial closure | N/A |
| 14 | Munshi et al., 2006 [ | 27, M | HL | ⅡB | trachea | N/A | at diagnosis | chemo (ABVD), RT | N/A | N/A | N/A | N/A | CR | spontaneous closure | 1 yr post-treatment completion |
| 15 | Moree et al., 2006 [ | 10, M | T-cell lymphoblastic lymphoma | N/A | trachea | 50 | during chemo | chemo | (-) | (-) | (-) | yes | ♰ death (bleeding) | persistence | 66 days post-admission |
| 16 | Valenti et al., 2008 [ | 68, M | DLBCL | N/A | trachea | N/A | post-chemo | chemo (R-CHOP) | yes | yes | (-) | yes | remission | artificial closure | N/A |
| 17 | Joshi et al., 2008 [ | 56, M | ALK-1 positive ALCL | ⅢB | trachea | N/A | at diagnosis | chemo (CHOP, DHAP), ASCT | (-) | (-) | (-) | yes | good response | spontaneous closure | N/A |
| 18 | Kutchuk et al., 2009 [ | 36, F | relapsed HL | Ⅳ | trachea (connected to esophagus and left common carotid artery) | 13 | post-mortem (autopsy) | none | (-) | (-) | (-) | (-) | ♰ death (hemorrhagic shock) | persistence | 12 hours post-admission |
| 19 | Sharma et al., 2011 [ | 63, M | PTCL-NOS | advanced stage | right intermediate bronchus | N/A | at diagnosis | chemo (COP) | (-) | (-) | (-) | yes | good response | N/A | N/A |
| 20 | Westin et al., 2012 [ | 53, F | HL | advanced stage | trachea | N/A | 6 yrs post-diagnosis (untreated) | chemo (AVD) | (-) | yes (trachea) | (-) | yes | CR | spontaneous closure (stent later removed) | 6 yrs post-initial treatment |
| 21 | Rigney et al., 2013 [ | 29, M | HL | ⅢB | right upper lobe bronchus | 30 | at diagnosis | chemo (BEACOPP) | (-) | yes (esophagus) | (-) | yes | good response | spontaneous closure (stent later removed) | 3 mos post-chemo completion |
| 22 | So and Adler, 2014 [ | 76, M | NHL | N/A | trachea | 10 | post-chemo | chemo | (-) | yes (esophagus) | yes | yes | N/A | artificial closure | N/A |
| 23 | Munikoty et al., 2017 [ | 10, F | HL | ⅢBE | mid trachea (two locations) | 22 x 25 x 24 | at diagnosis | chemo (DXR/VCR/ETP/PSL/CY/DTIC) | yes | (-) | (-) | yes | good response | artificial closure | more than 1 y post-surgery |
| 24 | Teerakanoket al., 2017 [ | 60, M | DLBCL | ⅣB | trachea, left main bronchus | 30 and 15, in double location | at diagnosis | chemo (R-CHOP) | (-) | yes (esophagus, tracheobronchial tree) | (-) | yes | good response | persistence | until completion of chemo |
| 25 | Dai et al., 2017 [ | 52, F | MALT lymphoma | N/A | trachea | 6 x 7 | 6 mos post-tracheal resection (TEF caused by prolonged tracheal stent placement and RT for post-resection stenosis) | surgery (tracheal resection and carina reconstruction) | yes (reoperation) | yes (trachea) | (-) | yes | remission | artificial closure | N/A |
| 26 | Kashyap et al., 2019 [ | 21, F | PMBL | N/A | trachea | N/A | post-chemo | RT, chemo (Rituximab, CY/DXR/VCR) | yes | yes (esophagus) → removed | (-) | yes | palliative care | N/A | N/A |
| 27 | Smiti et al., 2019 [ | 27, M | HL | IV | right bronchus | N/A | 1 m after 2nd chemo cycle | RT, chemo | (-) | (-) | (-) | (-) | ♰ death (respiratory failure) | persistence | N/A |
| 28 | Fontanella et al., 2020 [ | 67, M | PMBL | IV | almost at the carina | 4 | 8 mos post-treatment | chemo (R-CHOP), RT | (-) | yes (esophagus) | (-) | (-) | CR | artificial closure | N/A |
| 29 | Wang et al., 2021 [ | 66, F | DLBCL | IV | trachea | 35 | 20 days post-treatment | chemo (CVP) | (-) | (-) | (-) | (-) | good response → treatment discontinued per family's decision | persistence | N/A |
| 30 | Nwankwo et al., 2021 [ | 76, F | relapsed DLBCL | N/A | left bronchus | 30 | after discontinuation of chemo | chemo (tafasitamab-cxix/lenalidomide) | (-) | yes (esophagus) | (-) | (-) | respiratory failure, opted for palliative care | artificial closure | N/A |
| 31 | Hayashi et al., 2022 [ | 46, F | ALK-negative ALCL | IIE | trachea | N/A | after first CHOP cycle | chemo (CHOP, BV, GDP), ASCT | yes | (-) | (-) | yes | CR | artificial closure | 2 yrs post-ASCT |
| 32 | Xuan et al., 2023 [ | 27, F | HL | III | trachea | 20 x 12 | after 2nd chemo cycle | chemo (ABVD) | (-) | yes (esophagus, trachea) | (-) | yes | remission | artificial closure | N/A |
| 33 | Ali et al., 2023 [ | 79, F | DLBCL | N/A | trachea | N/A | at diagnosis | none | (-) | (-) | yes | (-) | uncontrolled pneumonia and septic shock, opted for palliative care | artificial closure | N/A |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTracheal and airway disorders · Esophageal and GI Pathology · Esophageal Cancer Research and Treatment
Introduction
Diffuse large B-cell lymphoma (DLBCL) is an aggressive and the most common subtype of non-Hodgkin lymphoma (NHL), accounting for 30-40% of cases. Tracheoesophageal or bronchoesophageal fistulas (TEFs/BEFs) are pathological connections between the tracheobronchial tree and the esophagus. These fistulas typically present with symptoms such as dysphagia, fever, weight loss, and the characteristic sign of coughing during meals [1]. While malignant esophagorespiratory fistulas are frequently associated with esophageal and lung cancers, with squamous cell carcinoma (SCC) accounting for 85.5% to 87.9% of cases, their occurrence in lymphoma is rare, constituting merely 0.4% to 1.4% of all cases [2,3]. Solid tumor-associated TEFs/BEFs have a poor prognosis, characterized by a median survival duration of 35 days [3,4]. Conversely, lymphoma-related TEF/BEF exhibits a relatively favorable prognosis relative to solid tumors [5-8]. Limited reports, particularly those involving Hodgkin's lymphoma and low-grade NHL, have documented the healing of fistulas subsequent to chemo/radiotherapy without the need for surgical or stenting interventions. However, this phenomenon has not been reported in patients diagnosed with diffuse large B-cell lymphoma (DLBCL). We present the first case of DLBCL, an aggressive NHL, with TEF resolution following chemotherapy alone.
Case presentation
A 74-year-old man with a history of hypertension and prostate cancer was referred to our hospital with a 2-week history of worsening productive cough and fever. Contrast-enhanced computed tomography (CT) revealed indications of right supraclavicular and mediastinal lymphadenopathy alongside a cervical-to-thoracic esophageal mass. Additionally, CT indicated a TEF (measuring 5 mm in diameter and 1 cm in length) and signs of aspiration pneumonia (Figure 1a). Upper gastrointestinal endoscopy revealed an ulcer and a tracheal fistulous connection at the site of cervical esophageal stenosis (Figure 1b). Histopathological analysis demonstrated primarily necrotic esophageal ulcers. Furthermore, a right supraclavicular lymph node biopsy revealed diffuse infiltration of abnormally large lymphoid cells, demonstrating positive CD20 and BCL6 expression and negative CD10 and MUM1 expression (Figure 2). The patient was diagnosed with DLBCL (germinal center B-cell type), with the bone marrow remaining unaffected, resulting in classification under the Lugano IIE clinical stage.
Computed tomography (CT) image and upper gastrointestinal endoscopy findings upon admission(a) CT image depicted a tracheoesophageal fistula measuring 5 mm in diameter and 1 cm in length, alongside aspiration pneumonia. (b) Upper gastrointestinal endoscopy findings revealed an ulcerous lesion and a fistulous connection to the trachea within the cervical esophagus.
Histopathological findings of the right supraclavicular lymph node(a) Hematoxylin-eosin staining showed the diffuse infiltration of abnormal large lymphoid cells (at 400× magnification). (b) Immunostaining indicated the positive staining of abnormal lymphoid cells for CD20 and BCL6 while testing negative for CD10 and MUM1.
The aspiration pneumonia was managed with antibiotics, oral intake cessation, and initiation of enteral nutrition via a gastric tube. After successful pneumonia control, a regimen of reduced-dose rituximab-combined chemotherapy was initiated (cyclophosphamide 375 mg/m^2^, doxorubicin 25 mg/m^2^, and vincristine 0.7 mg/m^2^ administered intravenously on day 1, and rituximab 375 mg/m^2^ administered intravenously on day 7). Owing to concerns about exacerbating pneumonia, steroids were excluded from this regimen. Notably, pneumonia recurred post-initial chemotherapy owing to vomitus aspiration. Subsequent to the resolution of pneumonia with antibiotics, the second chemotherapy cycle was initiated using the same regimen alongside total parenteral nutrition. From the third cycle onward, the chemotherapeutic dosage was progressively increased, with a total of six cycles administered (Figure 3). The patient achieved complete remission of DLBCL after four cycles, along with fistula closure (Figure 4). No esophageal leaks were observed during esophageal angiography. As the risk of aspiration diminished, steroids (prednisolone 100 mg/body, orally administered on days 1-5) were introduced during the fifth and sixth chemotherapy cycles. Following the fourth cycle, a liquid diet was reintroduced, eventually progressing to a regular diet 6 months post-chemotherapy completion. The patient presently maintains a well-nourished status through oral feeding. As of 46 months post-chemotherapy completion, there have been no observed instances of lymphoma recurrence or TEF.
Clinical courseC: cyclophosphamide; H: daunorubicin; O, VCR: vincristine; P: prednisolone; R: rituximab; sIL-2R: soluble interleukin-2 receptor; CRP: C-reactive protein
Images after chemotherapy(a) CT and endoscopy findings after four chemotherapy cycles showed fistula closure and complete remission of DLBCL. (b) Positron emission tomography (PET) image after six chemotherapy cycles indicated complete metabolic remission.
Discussion
To the best of our knowledge, this is the first reported case of DLBCL-associated TEF that healed following chemotherapy. Our study presents two critical insights. First, in lymphoma-related TEF/BEF, minimizing the risks of aspiration and infection is paramount, requiring a preliminary conservative approach for fistula management. Second, in cases that initially present with a fistula followed by a positive response to chemotherapy and/or radiotherapy, there is a possibility of spontaneous fistula resolution without the requirement for interventions, such as stenting and surgical correction.
Between 1990 and 2023, we identified 33 documented instances of lymphoma complicated by TEF/BEF within the English literature (Table 1) [6-39]. The median age in these cases was 53 years (range: 10-79 years), with 18 men and 15 women. Notably, Hodgkin's lymphoma emerged as the most prevalent subtype (15/33 cases, 45%). Within non-Hodgkin's lymphomas, DLBCL constituted the predominant type (7/33 cases, 21%).
In instances of lymphoma complicated by TEF/BEF, effective management of aspiration and infection is pivotal for improving outcomes. Among the documented cases, interventions targeted at fistula closure were administered in 22/33 cases: 8 underwent surgery, 9 received stent placement, 3 underwent a combination of stent and surgery, 1 received a combination of stent and OTSC (over-the-scope clip), and 1 was managed solely with OTSC. Notably, the prevalence of stent placements increased after 2010. Within these 33 cases, 6 were managed solely through enteral nutrition, out of which 4 achieved fistula closure through chemo/radiotherapy. While fistula management requires individualization, several reports recommend an initial conservative approach with enteral nutrition [9,10]. Furthermore, in cases where respiratory symptoms persist, less invasive interventions, such as removable stents, could be considered and escalated to surgical correction if warranted [11]. In our case, we opted for total parenteral nutrition and enteral nutrition without stent insertion because i) the esophageal stenosis was proximal and ii) inadequate stenosis within both the esophagus and trachea heightened the risk of stent migration. Given its potential to heal, adopting a conservative approach toward fistula management is advised. Moreover, as exemplified in our case, tailoring chemotherapy dosages to the patient's condition can ameliorate risks associated with bone marrow suppression and subsequent infections.
Two mechanisms have been proposed for the formation of lymphoma-related TEF/BEF [5]: the first attributes the fistula to primary lymphomatous involvement of the esophagus or tracheobronchial tree, whereas the second links it to the necrosis and breakdown of mediastinal lymph nodes between the esophagus and tracheobronchial tree. Specifically, the former can lead to fistula formation during the initial presentation, analogous to our case, whereas the latter, associated with lymph node necrosis, might result in fistula development during or after chemo/radiotherapy [12,13].
Our report categorizes cases into two types: those with a fistula present at the time of initial diagnosis or relapse, termed “pre-treatment fistula,” and those that emerge during or after chemo/radiotherapy, referred to as “post-treatment fistula.” Within the literature (Table 1), “pre-treatment fistula” was observed in 15/33 cases (45%), “post-treatment fistula” was noted in 17 cases (52%), and in one case, the fistula was identified posthumously. Additionally, “pre-treatment fistula” was more prevalent within Hodgkin's lymphoma cases (10/15 cases). Out of the 33 cases, information concerning the status of fistula closure was available for 31 cases. Notably, seven of these exhibited “healing” of the fistula (two of which had undergone stent placement prior to initiating treatment). Subsequently, the fistula closed, leading to the removal of the stent) [7,9,11,12,14-16]. All seven of these cases manifested a “pre-treatment fistula” and showcased a favorable response to chemotherapy and/or radiotherapy. In contrast, spontaneous closure was not observed when fistulas developed during or after therapy (“post-treatment fistula”), despite the lymphoma having entered remission, with such patients requiring interventions for fistula repair. Notably, the precise mechanism underlying fistula healing remains elusive; however, Rigney et al. proposed that esophageal defects undergo epithelialization, suggesting that the fistula might heal upon achieving sepsis control, positive tumor response to treatment, and the establishment of effective enteral nutrition [11]. Two out of the 15 “pre-treatment fistula” cases could not undergo lymphoma treatment due to respiratory failure or sepsis, which may suggest that fistula closure occurred more frequently in patients with relatively stable conditions.
In anatomical analyses, regarding fistula location, the majority were situated in the trachea, accounting for 64% (21/33) of the cases, followed by the left main bronchus (4 cases), and the right main bronchus (3 cases). One case involved both the trachea and left main bronchus, another occurred at the carina, and three were located distal to the right main bronchus. No significant differences were observed in fistula location between cases with healed versus persistent fistulas. Data on fistula size were available for 19 of the 33 cases, with a median diameter of 15 mm (range: 4-60 mm). Among these, two cases with sizes of 6 mm and 30 mm healed following chemotherapy. In our case, the fistula measured 5 × 10 mm, and no definitive correlation was observed between fistula size and closure.
Outcome data were available for 32 out of 33 cases. Of these, 20 cases survived without progression of the lymphoma, while 3 cases experienced progression or recurrence. In 4 cases, palliative care or treatment withdrawal was chosen, and 5 cases resulted in death where two due to respiratory failure, 2 from hemorrhage, and 1 from lymphoma progression. Among the seven cases where fistula healing was achieved, six had a median follow-up period of 12 months (range: 3-72 months), with no recurrence of either the lymphoma or the fistula (one case lacked a documented follow-up duration). Additionally, in our case, the patient remained progression-free for 46 months post-treatment, suggesting that long-term survival may be achievable when fistula healing is attained. In most instances, determining survival outcomes was challenging owing to the limited follow-up duration.
Conclusions
TEF represents a rare complication within malignant lymphomas. The prognosis of TEF/BEF within lymphomas is more promising than that of solid tumors. Cases featuring initial fistula presentations have the potential for fistula resolution using chemotherapy and/or radiotherapy in tandem with effective management of aspiration and lymphoma. To investigate the mechanisms of fistula formation, healing, and long-term prognosis, it is necessary to accumulate additional cases and examine the characteristics of those with fistula complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tracheoesophageal fistula Chest Surg Clin N Am Reed MF Mathisen DJ 2712891320031275531310.1016/s 1052-3359(03)00030-9 · doi ↗ · pubmed ↗
- 2Esophagorespiratory fistulas of tumorous origin. Non-operative management of 264 cases in a 20-year period Eur J Cardiothorac Surg Balazs A Kupcsulik PK Galambos Z 110311073420081867850410.1016/j.ejcts.2008.06.025 · doi ↗ · pubmed ↗
- 3Malignant esophagorespiratory fistula: management options and survival Ann Thorac Surg Burt M Diehl W Martini N 12221229521991175567410.1016/0003-4975(91)90005-b · doi ↗ · pubmed ↗
- 4Management of malignant tracheoesophageal fistula Thorac Surg Clin Shamji FM Inculet R 3934022820183005407710.1016/j.thorsurg.2018.04.007 · doi ↗ · pubmed ↗
- 5Tracheoesophageal fistula in the patient with lymphoma: case report and review of the literature Surgery Perry RR Rosenberg RK Pass HI 7707771051989 https://www.surgjournal.com/article/0039-6060(89)90338-3/abstract 2471284 · pubmed ↗
- 6Primary esophageal diffuse large B cell lymphoma presenting with tracheoesophageal fistula: a rare case and review World J Gastrointest Oncol Teerakanok J De Witt JP Juarez E Thein KZ Warraich I 431435920172908557010.4251/wjgo.v 9.i 10.431PMC 5648987 · doi ↗ · pubmed ↗
- 7Tracheoesophageal fistula in a patient with recurrent Hodgkin's disease. A case for hope or despair Chest Ling D Bushunow P 8508511091996861710510.1378/chest.109.3.850 · doi ↗ · pubmed ↗
- 8Tracheoesophageal fistula developing during chemotherapy for non-Hodgkins lymphoma J Surg Oncol Lackner RP Bierman PJ Galbraith TA 265267631996898237210.1002/(SICI)1096-9098(199612)63:4<265::AID-JSO 9>3.0.CO;2-A · doi ↗ · pubmed ↗