Chemotherapy-Associated Cardiotoxicity: A Silent Threat Evidenced in a Retrospective Cohort Study
Felipe A Muñoz-Rossi, Santiago Cárdenas-Corredor, Luis Fernando Saldarriaga Osuna, Diego A Guerra Kunze, Patricia León-León, Donovan A Sánchez, Vanessa Mejia Nates, Luis Felipe Franco Puente, Pamela L Suarez Jaramillo, Antonio J Reche Martinez

TL;DR
This study shows that chemotherapy can cause heart damage in cancer patients, with certain drugs and conditions increasing the risk, highlighting the need for better monitoring.
Contribution
The study provides new evidence on the incidence and risk factors of chemotherapy-induced cardiotoxicity in a Colombian cancer cohort.
Findings
20 out of 197 patients (10%) developed cardiotoxicity during follow-up.
Anthracycline exposure was linked to a higher cardiotoxicity risk (11.8% vs. 5.7%).
Patients with cardiotoxicity had lower left ventricular ejection fractions (55.3% vs. 62.1%).
Abstract
Introduction: At present, cancer represents one of the main causes of mortality both globally and in Colombia, with a growing trend that could position it as the leading cause of death shortly, surpassing other diseases of great health impact. Cardiotoxicity associated with antineoplastic treatments can manifest itself at different times, either during the administration of chemotherapy or sometime after its completion, becoming evident only when clinical complications such as heart failure have developed. Therefore, it is essential to use diagnostic tools to identify patients at greater risk of developing cardiotoxicity associated with administering chemotherapeutic agents. Methods: We conducted a descriptive observational cohort study, which included patients over 18 years of age with an active diagnosis of cancer, both of hematological or nonhematological origin, who were treated in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1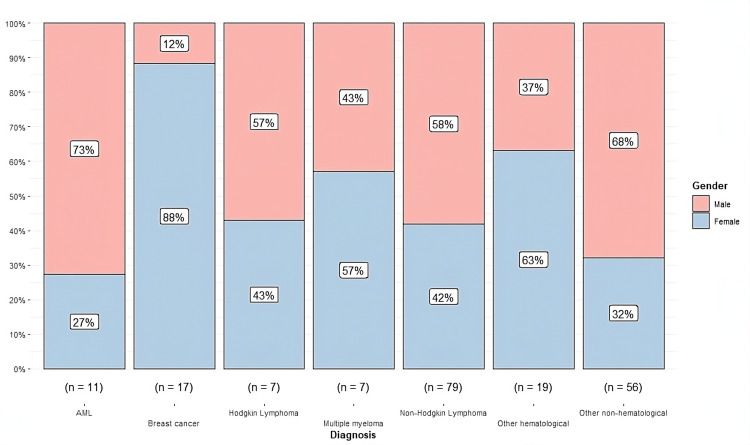 Figure 2
Figure 2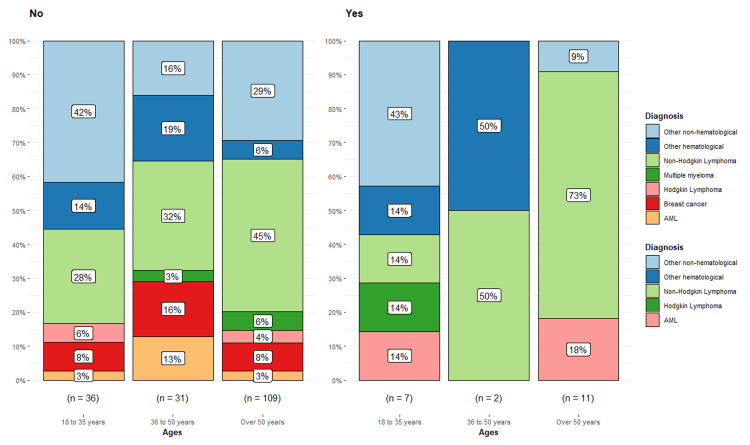 Figure 3
Figure 3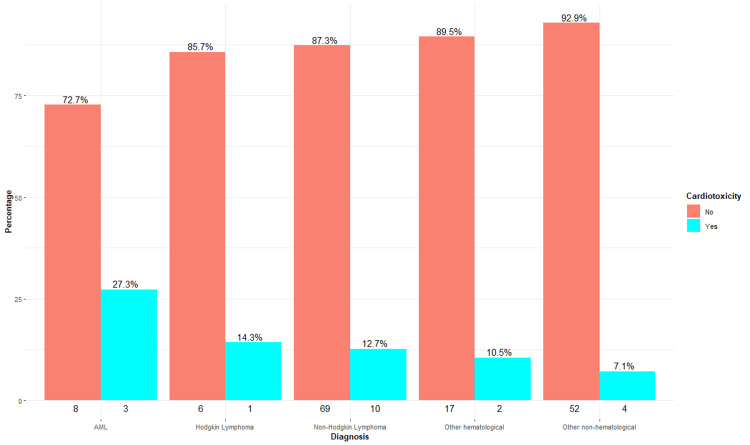 Figure 4
Figure 4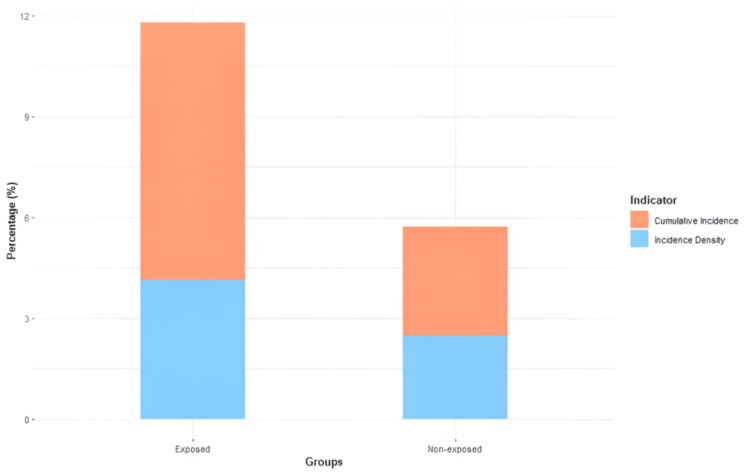 Figure 5
Figure 5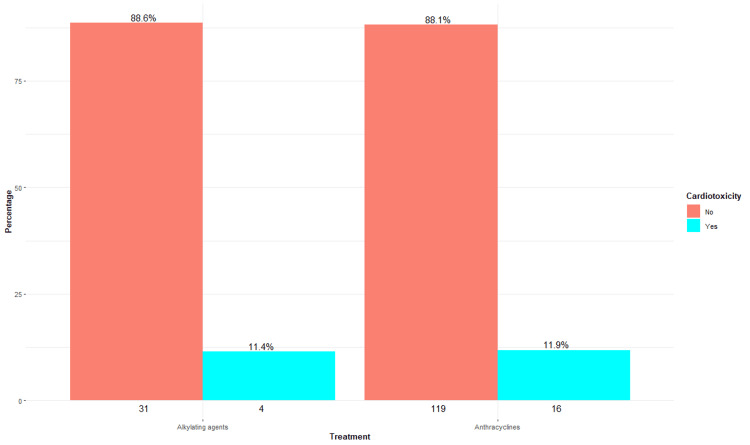 Figure 6
Figure 6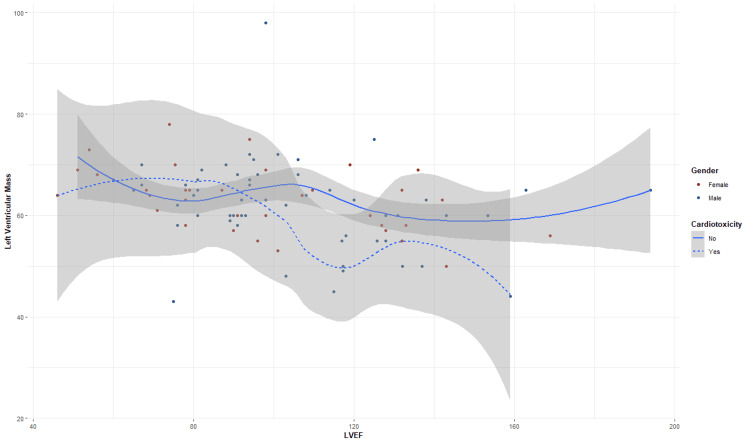 Figure 7
Figure 7| Variables | Values (n = 197) |
| Age, mean (95% CI) | 53 (50.6-55.4) |
| Sex, n (%) | |
| Male | 109 (55) |
| Female | 88 (47.7) |
| Comorbidities, n (%) | |
| Arterial hypertension | |
| No | 92 (71.3) |
| Yes | 37 (28.7) |
| Dyslipidemia | |
| No | 71 (55) |
| Yes | 58 (45) |
| Diabetes mellitus | |
| No | 123 (95.3) |
| Yes | 6 (4.7) |
| Acute coronary syndrome | |
| No | 188 (96) |
| Yes | 7 (3.6) |
| Atrial fibrillation | |
| No | 185 (95) |
| Yes | 10 (5.1) |
| Heart failure | |
| No | 168 (86) |
| Yes | 27 (14) |
| Peripheral artery disease | |
| No | 171 (88) |
| Yes | 24 (12) |
| Cancer type | Total, n (%) | Metastasis, n (%) | Ctox, n (%) |
| Non-Hodgkin lymphoma | 79 (40.3) | 14 (7.1) | 10 (5.1) |
| Other nonhematological | 56 (28.6) | 30 (15.3) | 4 (2.0) |
| Other hematological | 19 (9.7) | - | 2 (1.0) |
| Breast cancer | 17 (8.7) | 7 (3.6) | - |
| Acute myeloid leukemia | 11 (5.6) | - | 3 (1.5) |
| Hodgkin lymphoma | 7 (3.6) | 2 (1.0) | 1 (0.5) |
| Total (n) | 18-35 years (n = 43) | 36-50 years (n = 33) | Over 50 years (n = 121) | Test statistic | |
| 197 | 7 (16.3%) | 2 (6.1%) | 11 (9.1%) | X2 = 2.52; p= 0.28 |
| Total (n) | No (n = 142) | Yes (n = 54) | Test statistic |
| 197 | 15 (10%) | 5 (10%) | X2 = 1.09; p = 0.57 |
| Test statistic | Statistic | p |
| Mann-Whitney U test | 687 | 0.029 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChemotherapy-induced cardiotoxicity and mitigation · Cancer-related cognitive impairment studies · Polymer Nanocomposite Synthesis and Irradiation
Introduction
To this day, cancer remains one of the top causes of death around the globe. It is also the second greatest cause of death in Colombia, accounting for about 17% of the overall mortality rate in the nation [1]. It is anticipated that by the year 2030, cancer will overtake cardiovascular disease as the leading cause of death [2].
In this study, we defined cardiovascular toxicity as cancer therapy-related cardiac dysfunction (CTRCD). This broad concept encompasses diverse clinical and subclinical manifestations and reflects the etiologic link to the extensive scope of oncospecific therapies, including chemotherapy, targeted agents, immunotherapies, and radiotherapy [3].
Definitions taken from the European Society of Radiology and Oncology and the International Society of Cardio-Oncology 2022 were taken to primarily define cardiac dysfunction in the setting of oncospecific therapies [3].
Symptomatic CTRCD is characterized by signs and symptoms of heart failure (HF). According to the intensity of the clinical manifestations, it is classified as very severe, severe, moderate, and mild. In the very severe category, HF requires inotropic support, mechanical circulatory support, or consideration of heart transplantation. In the severe classification, hospitalization for HF is needed. For its part, in moderate conditions, outpatient treatment intensification is necessary, especially with diuretics and management of HF. While in mild cases, there are minimal symptoms of HF that do not require intensification of treatment.
On the other hand, asymptomatic CTRCD includes subclinical cardiac dysfunction and is classified into three groups according to left ventricular ejection fraction (LVEF): severe, moderate, and mild. In the severe category, there is an additional reduction in LVEF to values less than 40%. In the moderate group, two scenarios can be presented; in the first, there is an additional reduction in LVEF of ≥10 percentage points, with final values between 40% and 49%; in the second scenario, there is a reduction in LVEF <10 percentage points within the range of 40%-49%, accompanied by a further relative decrease in global longitudinal strain (GLS) >15% from baseline or a further increase in cardiac biomarkers. Finally, in the mild category, LVEF readings are equal to or greater than 50%, with a new relative drop in GLS greater than 15% compared to baseline and/or a new increase in cardiac biomarkers.
It is feasible to clearly describe cardiac dysfunction produced by oncospecific treatment thanks to these criteria, which makes it possible to allow quick diagnosis and appropriate follow-up of patients at risk of cardiotoxicity. Cardiotoxicity is an adverse effect of cancer-specific treatment; consequently, early identification and continuous monitoring of cardiac function in patients undergoing cancer-specific treatment include initial evaluation by detailed clinical history, complete physical examination, and specific diagnostic tests such as echocardiogram, cardiac magnetic resonance imaging, and measurement of biomarkers such as natriuretic peptides and troponin [4,5].
In this scenario, they may include alternative management and monitoring strategies, such as using different cardiac imaging modalities (nuclear imaging and computed tomography) and variations in the frequency and timing of assessments [6]. Interventions can also be compared with traditional management approaches or different cardioprotection regimens.
Drug-induced anticancer cardiotoxicity is influenced by a number of characteristics, such as patient age, previous cardiovascular disease, duration, and type of oncospecific therapy [7]. Therefore, it is essential to have a comprehensive approach in care centers to detect possible cardiovascular complications and treat them promptly to minimize the risk of cardiovascular damage in the medium and long term [8].
The identification of cardiotoxicity consists of a comprehensive assessment of the patient's preexisting cardiovascular risk factors [9]. A limited number of studies have generated different risk scales in selected patient cohorts. However, none of these scales have validation in prospective studies, and in many cases, clinical judgment ends up being a fundamental decision-making tool in certain patient scenarios [10-15]. Therefore, risk assessment should include a complete clinical history with a thorough physical examination and baseline assessment of cardiac function.
Cardiac biomarkers such as natriuretic peptides and troponin should be added to the initial assessment and during follow-up; this approach allows subclinical detection of asymptomatic left ventricular dysfunction and may influence decision-making about the choice of chemotherapy, initiation of cardioprotective measures, or increased periodic patient surveillance [7,16].
Given the above, the initial assessment of the identification of cardiovascular risk factors allows for the proper interpretation of changes during regular monitoring of patients requiring oncospecific treatment.
The different strategies for screening and detecting cardiotoxicity include cardiac imaging (echocardiography, nuclear imaging, and magnetic resonance imaging) and biomarkers [17]. The choice depends on the availability of resources and expertise in their interpretation. The precise timing and frequency of imaging and/or biomarker acquisition will depend on the oncospecific treatment received, cumulative chemotherapy dose, protocol duration, and the patient's baseline cardiovascular status. As part of good clinical practice, certain principles should be followed when ordering cardiac imaging and biomarkers. Some of these principles highlight that tests and modalities with better reproducibility are preferred, images that also provide relevant clinical information are selected, high-quality images without radiation are preferred if available, and finally, the same imaging modality and biomarkers should be used at both initial evaluation and follow-up, as this allows for point-of-care screening and detection [3,18,19].
Oncology treatment, although effective, carries significant risks of cardiovascular toxicity. Since oncology treatment-induced cardiotoxicity can have serious consequences, such as cardiac dysfunction, it is crucial to identify and manage these side effects effectively. Therefore, the objective of the present study is to determine the incidence of cardiotoxicity in adult cancer patients under antineoplastic treatment in a tertiary level hospital in Colombia.
Materials and methods
A single-center, retrospective cohort study was conducted in a tertiary care institution in Bogotá, Colombia. The data collection period covered three years. The reference population consisted of patients over 18 years of age with an oncologic diagnosis who were treated with chemotherapy on an outpatient or inpatient basis during the study period.
The inclusion criteria include oncologic patients older than 18 years and treated with chemotherapy in a third-level institution in Bogota, Colombia. However, excluded individuals included pregnant patients, those with HIV infection, patients with severe functional and instrumental dependence defined by a Barthel index <50 points and a Lawton scale <5/8, and those whose echocardiographic studies did not comply with Simpson's modified biplane method for ejection fraction or with myocardial deformation measurements by GLS performed with uniform software.
The sample size was calculated using the G*Power 3.1.9.7 program (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany) under an independent mean comparison model with normal distribution. With a confidence level of 95%, a statistical power of 80%, and an effect size of 0.4, 198 subjects were deemed necessary.
Statistical analysis
We began with a univariate analysis to describe the sociodemographic and clinical characteristics of the population. In the bivariate analysis, categorical variables were analyzed using contingency tables and chi-square tests, while continuous variables were described using measures of central tendency, verifying normality with the Kolmogorov-Smirnov test. In the case of normal distribution, Student’s t-tests and Pearson correlation coefficients were used; otherwise, the Mann-Whitney test was used.
As measures of association, relative risks (RR) were calculated, and multivariate analyses were performed with logistic regression models for cardiotoxicity and Cox regression models adjusted for time at risk. Survival curves were generated using the Kaplan-Meier method and evaluated with the log-rank test.
Follow-up included inpatient and outpatient surveillance. Baseline data were collected at patient admission, and follow-up with hepatic profiling was performed until the occurrence of events such as cardiotoxicity, hospital discharge, or death.
Data were analyzed with SPSS version 27.0 (IBM Corp., Armonk, NY) and RStudio (Posit Software, Boston, MA) for visualization, considering a statistical significance level of p < 0.05. Frequency measures included cumulative incidence and incidence rate in the exposed cohort.
Ethical considerations
Considering the retrospective nature of the study, it is a risk-free investigation. No interventions that may modify patient behaviors and treatments will be carried out, so informed consent is not necessary. The confidentiality of the information obtained was guaranteed without mentioning the names of the patients or the medical personnel involved. The health center requested the corresponding authorization to carry out this study. The investigators declare that they have no conflicts of interest.
This research will be carried out in compliance with the fundamental principles established in the Nuremberg Code (1947), the Declaration of Helsinki (1964), and the Belmont Report (1979), which prioritize the well-being and identity of the individuals involved.
Results
The study included 197 subjects admitted for oncospecific treatment: 109 were men, comprising 55.3% of the population, while 88 were women, representing 44.7%. The mean age was 53 years (95% confidence interval, CI = 50.6-55.4). The sum of the periods at risk was 548.8 person-months. During follow-up, 20 patients (10%) presented with cardiotoxicity (Figure 1), while the incidence density was 3.64% person-months of follow-up.
Incidence of cardiotoxicityData are presented as a percentageTotal number of patients: n = 197. Yes: 20 patients (10%). No: 177 patients (90%)
As for the main comorbidities reported, dyslipidemia was the prevalent one, present in 45% (n = 58) of the subjects, followed by arterial hypertension with 28.7% (n = 37), HF with 14% (n = 27), and peripheral arterial disease with 12% (n = 24) (Table 1).
According to the oncological diagnoses, the most frequent was non-Hodgkin's lymphoma, with 40.3% (n = 79), with evidence of cardiotoxicity in 10 subjects. The types of cancer are represented in Table 2.
A distribution by gender and type of oncologic diagnosis is presented, showing a higher representation in our study population of non-Hodgkin's lymphoma (79/196). Most patients are men, constituting 58% (n = 46), while women represent 42% (n = 33), indicating a notable male predominance in this type of oncologic pathology. On the other hand, as expected, breast cancer was primarily observed in women, accounting for 88% (n = 15), while men represented only 12% (n = 2), consistent with the known epidemiology (Figure 2).
Distribution by gender and type of oncologic diagnosisn represents the number of nonmissing values
Characteristics of patients with cardiotoxicity secondary to chemotherapy
A total of 55% of the patients in our research who had cardiotoxicity were over 50 years old (n = 11/20), and they were mostly diagnosed with acute myeloid leukemia (AML; 18%, n = 2/11) and non-Hodgkin's lymphoma (73%, n = 8/11) (Figure 3). Notably, neither multiple myeloma nor breast cancer patients had any instances of cardiotoxicity. However, the difference in cardiotoxicity incidence across age groups (16.3%, 6.1%, and 9.1%) was not statistically significant (Pearson's chi-square, p = 0.28) (Table 3).
Relationship between ages/cardiotoxicity and oncologic diagnosisData are presented as a percentage. n is the number of nonmissing values
Table 3: Cross table comparing dependent ages and cardiotoxicityA p value of <0.05 is considered significant. The statistical test used was Pearson's chi-square test
Regarding the presence of metastases in oncological patients, no discernible patterns were found that could be related to the appearance of cardiotoxicity. Based on this information, it appears that the existence of metastases does not play a significant role in the development of cardiotoxic adverse effects in this group. Furthermore, no statistically significant differences were identified between the groups, as shown by a Pearson's chi-square value of 1.093 (p = 0.57), indicating no significant correlation between the presence or absence of metastases and cardiotoxicity (Table 4).
Table 4: Cross-table comparing dependent metastasis and cardiotoxicityA p value of <0.05 is considered significant
In our analysis of cardiotoxicity according to the different oncologic diagnoses, an incidence of 27% (n = 3/11) was observed in patients with AML, while those with Hodgkin's lymphoma and non-Hodgkin's lymphoma showed an incidence of 14% (n = 1/7) and 13% (n = 10/79), respectively. In contrast, patients with multiple myeloma and breast cancer had no cases of cardiotoxicity. On the other hand, miscellaneous hematologic and nonhematologic diagnoses presented a moderate proportion, with 11% (n = 2/19) and 7% (n = 4/56), respectively (Figure 4). These findings highlight the need to monitor these patients under cardio-oncology programs.
Oncologic diagnoses and cardiotoxicityThe numbers below each bar represent the absolute frequency (n) of patients without (left) and with (right) cardiotoxicity for each diagnosis category
When the incidence of cardiotoxicity in patients was analyzed according to their exposure to anthracyclines, it was shown that the exposed group had a greater frequency of this problem than the other cohort. Within the group of persons who had not been exposed to anthracyclines, four occurrences of cardiotoxicity were recorded among the 70 individuals. The cumulative incidence of these cases was 5.71%, and the incidence density was 2.47 person-months of follow-up. On the other hand, in the exposed cohort, 16 occurrences of cardiotoxicity were found in 135 patients. This resulted in a considerably higher cumulative incidence of 11.8% and an incidence density of 4.13% person-months of follow-up (Figure 5).
Cumulative incidence and incidence density in anthracycline cardiotoxicity
Patients who were given anthracyclines had an RR of cardiotoxicity of 2.074 (95% CI = 1.91-2.24). This indicates that patients who were given anthracyclines had a risk of experiencing this complication that was more than twice as high as patients who were not given this therapy.
Anthracyclines were the most associated therapeutic category with cardiotoxicity, with an incidence of 12% (approximately); however, a similar finding was found concerning alkylating agents, with a cumulative incidence of 11%. In contrast, patients treated with taxanes, antivascular endothelial growth factor (VEGF), antihuman epidermal growth factor receptor 2 (HER2), and antimetabolites showed no cases of cardiotoxicity, which could indicate a possible lower cardiac toxicity related to these agents in this specific cohort (Figure 6).
Oncospecific therapy and cardiotoxicityThe numbers below each bar represent the absolute frequency (n) of patients without (left) and with (right) cardiotoxicity for each treatment category
In patients without cardiotoxicity (solid line), LVEF remains relatively stable as left ventricular mass (LVM) increases, with a tendency to recover at higher LVM values, suggesting that, in the absence of cardiotoxicity, ventricular function can compensate for the increased mass, maintaining an ejection fraction within functional limits.
However, in patients with cardiotoxicity (dotted line), there is a marked decrease in LVEF as LVM increases, probably due to a greater vulnerability of the left ventricle in these patients, secondary to the deleterious effects of the oncospecific treatment on cardiac function, with a statistically significant difference (p = 0.029, Mann-Whitney U test) between both groups with an LVEF of 55.29% (95% CI = 50.0-60.5) in patients with cardiotoxicity and 62.10% (95% CI = 60.79-63.79) in patients without cardiotoxicity, respectively (Table 5). Therefore, the decrease in LVEF in this scenario reveals an increased risk of cardiac dysfunction, reinforcing the need for early interventions and continuous follow-up in patients undergoing oncological treatments (Figure 7).
Table 5: Test statistic for LVEFSignificant Levene's test (p < 0.05) suggests that variances are not equalLVEF: left ventricular ejection fraction
Scatterplot smoothing LVEF/cardiotoxicityLVEF: left ventricular ejection fraction
Discussion
The present investigation places in evidence the incidence of cardiotoxicity in oncology patients undergoing cancer treatment, with findings similar to those reported by Cardinale et al., which indicated an incidence of 9% in a cohort of 2,625 patients, primarily associated with anthracycline dosage and LVEF at the end of treatment [20]. However, in a meta-analysis of 22,815 cancer subjects, 17.9% developed cardiotoxicity, and 10.9% experienced cardiac events during a 9-year follow-up [21].
In our cohort, the observed incidence is like that reported in previous research, which could suggest a susceptibility of our population to the cardiotoxic effects of oncologic regimens that are not far from studies conducted in developed countries.
In turn, the relationship observed between the presence of metastases and cardiotoxicity was not statistically significant. However, the possible association, together with the impact of oncologic treatment and advanced disease stage, warrants further investigation, as it could contribute to increased cardiac vulnerability.
With respect to ventricular function, patients without cardiotoxicity showed relative stability in LVEF as ventricular mass increased. This phenomenon is explained by the compensatory capacity of the left ventricle in the absence of severe myocardial damage [22,23]. However, in patients with cardiotoxicity, the progressive decrease in LVEF is a function of the increase in ventricular mass, probably due to the deleterious effects of oncospecific treatment. This pattern coincides with that reported by Cardinale et al. [24], who evidenced that changes in LVEF are a sensitive indicator of early cardiac damage in patients treated with chemotherapy.
In accordance with the above, we would like to highlight the need to implement cardio-oncology programs, especially for those patients with oncologic diagnoses that imply an elevated risk of cardiotoxicity depending on their oncospecific therapy. Continuous monitoring and early intervention could decrease cardiac complications, allowing better management of oncologic treatment without compromising patients' quality of life.
Finally, although our findings provide relevant information in our setting, they should be interpreted with caution, given the retrospective nature and sample size in this type of observational study. Future studies with longer long-term follow-ups will be necessary to confirm these observations and explore underlying mechanisms that explain the variability in susceptibility to cardiotoxicity in different types of cancer.
Limitations
Despite the reported findings, we would also like to highlight the following limitations that should be considered when interpreting the results. First, the retrospective nature of the research may lead to selection and reporting biases; therefore, to minimize this, a previous recording of the data was performed, analyzing the quality of the responses to the variable of interest. This allowed the data to be comparable between the groups.
Additionally, a pilot test of the selected variables was carried out in 20 subjects with the collection of information, and according to the results, adjustments were made to ensure the complete collection of information and to evaluate the quality of the information sources.
On the other hand, the sample size of some subgroups, such as those exposed to certain agents like anti-VEGF and anti-HER2, was limited, which prevents robust inferences about cardiotoxicity in these specific groups. In turn, the low incidence of some types of cancer (e.g., AML) and the paucity of patients with metastases may have limited the ability to detect statistically significant differences in these subgroups.
Another element to consider is follow-up time. Although rigorous monitoring was undertaken, the observation time may not have been adequate to identify late cardiotoxic episodes, which might underestimate the cumulative frequency of this problem.
Finally, the absence of a randomized control group inhibits the capacity to demonstrate unambiguous causal links between oncospecific therapy and the development of cardiotoxicity.
Conclusions
The findings highlight the importance of considering cardiotoxicity as a critical variable in the comprehensive management of oncology patients, especially in those without metastases and exposed to anthracyclines, where closer monitoring could prevent cardiac complications. Furthermore, it highlights the need to implement cardio-oncology departments and cardioprotective strategies that allow exhaustive and individualized monitoring, favoring personalized therapeutic approaches and improving long-term outcomes in this vulnerable population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Atlas of cancer mortality in Colombia Instituto Nacional de Cancerología - ESE: Bogotá D.C., Colombia 10 2022 Pardo Ramos C Vries Ede Buitrago Reyes LA Gamboa Garay O 2017 https://www.ins.gov.co/Ty S/programas-de-calidad/Documentos%20Programa%20EEDDCARIO/ATLAS_de_Mortalidad_por_cancer_en_Colombia.pdf
- 2Cancer incidence estimates and mortality for the top five cancer in Colombia, 2007-2011 Colomb Med (Cali) Pardo C Cendales R 16224920182998346010.25100/cm.v 49i 1.3596 PMC 6018817 · doi ↗ · pubmed ↗
- 32022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS)Eur Heart J Lyon AR López-Fernández T Couch LS 422943614320223601756810.1093/eurheartj/ehac 244 · doi ↗ · pubmed ↗
- 4Chemotherapy induced cardiotoxicity: a state of the art review on general mechanisms, prevention, treatment and recent advances in novel therapeutics Curr Probl Cardiol Abdul-Rahman T Dunham A Huang H 1015914820233662151610.1016/j.cpcardiol.2023.101591 · doi ↗ · pubmed ↗
- 5NT-pro BNP as predictor factor of cardiotoxicity during trastuzumab treatment in breast cancer patients Breast Blancas I Martín-Pérez FJ Garrido JM Rodríguez-Serrano F 1061135420203297729810.1016/j.breast.2020.09.001PMC 7511727 · doi ↗ · pubmed ↗
- 6Early screening of cardiotoxicity of chemotherapy by echocardiography and myocardial biomarkers Tunis Med Bouhlel I Chabchoub I Hajri E Ernez S Gouider J 10171023982020 https://pubmed.ncbi.nlm.nih.gov/33480006/33480006 · pubmed ↗
- 7Cardiovascular biomarkers in cardio-oncology: antineoplastic drug cardiotoxicity and beyond Biomolecules Attanasio U Di Sarro E Tricarico L 1991420243839743610.3390/biom 14020199 PMC 10887095 · doi ↗ · pubmed ↗
- 8Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations Ann Oncol Curigliano G Lenihan D Fradley M 1711903120203195933510.1016/j.annonc.2019.10.023PMC 8019325 · doi ↗ · pubmed ↗