Micro-Computed Tomography Assessment of the Quality of Obturation (Voids) of Single-Canal Maxillary Second Premolars by the Lateral Compaction versus Continuous Warm Vertical Condensation Techniques
Romina Hajipour, Maryam Zare Jahromi, Masood Khabiri

TL;DR
This study compared two root canal filling techniques using micro-CT to assess voids in maxillary second premolars and found no significant difference in void formation between the methods.
Contribution
The novel contribution is the use of micro-CT to quantitatively compare void formation in root canal obturation techniques for maxillary second premolars.
Findings
No significant difference was found between CLC and CWVC in void volume in the coronal third of root canals.
The lowest void volume and percentage were observed in the apical third for the CWVC group.
Neither technique achieved void-free root canal obturation.
Abstract
One of the most important stages of root canal treatment is obturation for the root canal, an obturation with less voids will have fewer treatment complications in the future. This study was conducted to compare the quality of obturation of single-canal maxillary second premolars by the cold lateral compaction (CLC) versus continuous warm vertical condensation (CWVC) techniques using micro-CT. In this experimental study, 36 extracted single-canal maxillary premolars were selected. The root canals were instrumented by Denco Blue rotary files. The teeth were randomly assigned to three groups (n=12) of control (no root filling), root canal obturation with CLC technique, and root canal obturation with CWVC technique. Next, they underwent micro-CT, and the mean volume and volume percentage (VP) of voids were calculated in the apical, middle, and coronal thirds of the root canals. Data were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
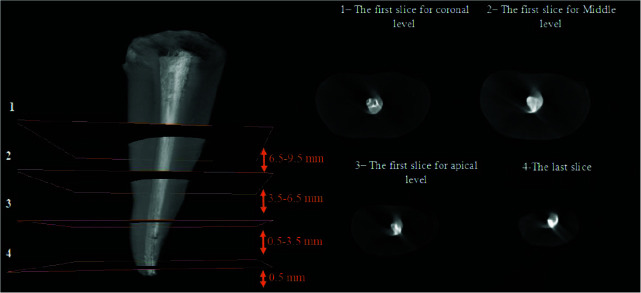 Figure 1
Figure 1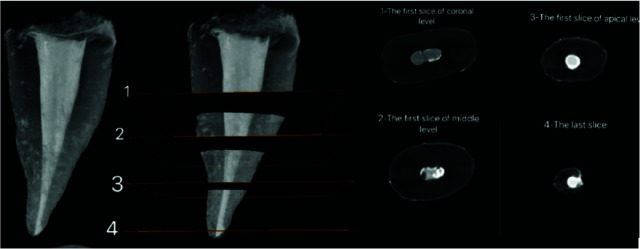 Figure 2
Figure 2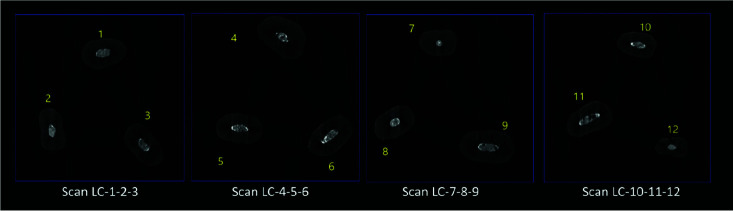 Figure 3
Figure 3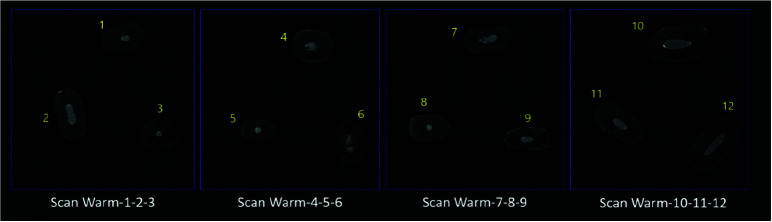 Figure 4
Figure 4| Volume of voids | Volume of filled areas | VP | |||||
|---|---|---|---|---|---|---|---|
| Mean | Std. deviation | Mean | Std. deviation | Mean | Std. deviation | ||
| CLC | Apical | 0.05304 | 0.040 | 1.1966 | 0.367 | 4.349 | 2.723 |
| Middle | 0.0789 | 0.0720 | 2.1652 | 0.692 | 3.4354 | 2.449 | |
| Coronal | 0.1292 | 0.108 | 3.7069 | 1.349 | 3.3309 | 2.167 | |
| Entire canal | 0.2614 | 0.210 | 7.0688 | 2.312 | 3.5569 | 2.169 | |
| CWVC | Apical | 0.0132 | .009 | 1.1024 | 0.262 | 1.1792 | 0.808 |
| Middle | 0.1544 | 0.132 | 2.5088 | 0.799 | 6.4839 | 7.431 | |
| Coronal | 0.1659 | 0.099 | 4.5344 | 1.967 | 3.8377 | 2.544 | |
| Entire canal | 0.3335 | 0.203 | 8.1458 | 2.860 | 4.3031 | 3.534 | |
| Volume of voids | Volume of filled areas | VP | |||||
|---|---|---|---|---|---|---|---|
| Mean | Std. deviation | Mean | Std. deviation | Mean | Std. deviation | ||
| Apical third | CLC | 0.05304 | 0.040 | 1.1966 | 0.367 | 4.349 | 2.723 |
| CWVC | 0.0132 | 0.009 | 1.1024 | 0.262 | 1.1792 | 0.808 | |
| Statistic | 3.28 | 0.722 | -3.233 | ||||
| 0.006 | 0.478 | 0.001 | |||||
| Middle third | CLC | .0789 | .0720 | 2.1652 | .692 | 3.4354 | 2.449 |
| WVC | .1544 | .132 | 2.5088 | 0.799 | 6.4839 | 7.431 | |
| Statistic | -1.386 | -1.328 | -1.155 | ||||
| 0.166 | 0.184 | 0.248 | |||||
| Coronal third | CLC | .1292 | 0.108 | 3.7069 | 1.349 | 3.3309 | 2.167 |
| CWVC | .1659 | 0.099 | 4.5344 | 1.967 | 3.8377 | 2.544 | |
| Statistic | -1.097 | -0.808 | -0.525 | ||||
| 0.273 | 0.419 | 0.605 | |||||
| Volume of voids | Volume of filled areas | VP | ||||
|---|---|---|---|---|---|---|
| Mean | Std. deviation | Mean | Std. deviation | Mean | Std. deviation | |
| CLC | .2614 | .210 | 7.0688 | 2.312 | 3.5569 | 2.169 |
| CWVC | .3335 | .203 | 8.1458 | 2.860 | 4.3031 | 3.534 |
| Statistic | -1.039 | -0.808 | -0.346 | |||
| 0.299 | 0.443 | 0.755 | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndodontics and Root Canal Treatments · Dental Radiography and Imaging · Dental materials and restorations
Introduction
The success of endodontic treatment depends on three main steps of effective debridement, efficient disinfection, and optimal obturation [ 1
- 2 ]. Ideally, the root filling material should three-dimensionally and homogenously fill the entire root canal space; however, this goal cannot be perfectly achieved in the clinical setting [ 3 ]. Resultantly, the microorganisms lodged in accessory canals or the periapical region may proliferate and colonize the residual voids [ 3 ].
The cold lateral compaction (CLC) technique is the widely practiced method of root canal obturation [ 4 ]. The CLC technique does not have high technical sensitivity, and is affordable. Nonetheless, the auxiliary (lateral) gutta-percha points used in this technique cannot ideally adapt to the root canal wall irregularities and some voids may remain [ 5 ].
The continuous warm vertical condensation (CWVC) technique is another root canal obturation technique, which was introduced to improve homogeneity and adaptation of root filling material to the root canals. In this technique, the master gutta-percha point along with sealer is introduced into the canal to the working length; the gutta-percha point is then packed into the canal by an element to 5 mm to the apex. Next, the residual space is filled with injectable thermoplastic gutta-percha [ 6
- 7 ].
Micro-computed tomography (micro-CT) is a novel highly accurate technique for reproducible assessment of specimens without their destruction [ 8
- 11 ]. Micro-CT was capable of precise 3D reconstruction of root canal filling [ 12 ]. Micro-CT was developed in early 1980, as a non-invasive and non-destructive imaging modality to obtain 3D images. It operates based on convergence of X-ray beams on the specimen and their receipt by a sensor. The irradiated X-ray is then converted to digital images [ 13 ].
In endodontic treatment, selection of an optimal root canal obturation technique is imperative to prevent root canal reinfection.
Considering all the above, the purpose of this study was to compare the quality of obturation of single-canal maxillary second premolars by the CLC versus CWVC techniques using micro-CT.
Materials and Method
This in vitro, experimental study was conducted on 36 single-canal maxillary second premolars extracted for reasons not related to this study such as orthodontic treatment or poor periodontal prognosis. The study was approved by the Ethics Committee of School of Dentistry, Islamic Azad University, Khorasgan Branch (IR.IAU.KHUISF.REC.1399.062).
Eligibility criteria
Mature teeth with closed apex, without root resorption, absence of tooth anomalies or calcification or anatomical variations or previous endodontic treatment were included in the study.
Schneider's method was used to measure the curve canals and teeth with a curve of 15 to 20 degrees were selected [ 14 ].
Each tooth underwent digital periapical radiography in labial and proximal directions to ensure meeting the eligibility criteria.
Sample size
The minimum sample size was calculated by random and simple method to be 12 in each of the three groups assuming alpha=0.5, beta=0.2, study power of 80%, mean values of 1.02 and 4.1 in the two groups, and standard deviations of 0.42 and 2.7 in the two groups. To increase accuracy, 12 teeth were included in each group.
Specimen preparation
The teeth were cleaned with 5.25% sodium hypochlorite (Morvabon, Iran) after extraction and stored in saline until use. Eligible teeth were then selected and decoronated with a diamond fissure bur (Teezkavan, Iran) under water coolant such that 14mm of root length remained for the purpose of standardization.
Root canal instrumentation
A K-file #10 (Mani, Japan) was introduced into the canal until its tip was visible at the apex; 1mm was subtracted from this length to determine the working length. After creating a glide path with a K-file#15 and radiographic confirmation of the working length, teeth with initial files larger than #30 were excluded. Denco Blue rotary files (Denco, China) up to F3 were used for root canal shaping with 2 N/cm torque and 250 rpm speed as instructed by the manufacturer with an endomotor (NSK, Japan). In the process of root canal cleaning and shaping, 5.25% sodium hypochlorite was frequently used. In addition, the canal path was preserved and the patency was verified by using a K-file#10. The root canals were then rinsed with saline, followed by 17% EDTA (Meta BioMed, Chungju, Korea) for 1 minute, and a final rinse with saline was then performed.
Root canal obturation
The teeth were randomly assigned to three groups (n=12) as follows:
Negative control group
The root canals were not obturated in this group.
CLC group
This group underwent obturation with the CLC technique using gutta-percha (DiaFil TM, DiaDent, Korea) and AH-Plus sealer (Dentsply Maillefer, Ballaigues, Switzerland). A #30/2% tapered gutta-percha point with tug-back was selected as the master cone. If the tug back was not achieved or the #30/2% gutta percha did not have a stop, the tooth was excluded and replaced by another one. After radiographic confirmation of the optimal length of the master cone, the root canals were dried with paper points (Dentsply Maillefer, Ballaigues, Switzerland). The master cone was dipped in sealer and inserted into the canal to the working length. A spreader (Mani, Japan), reaching 2-3mm of the working length [ 15 ], was used and accessory gutta-percha points (one size smaller than the spreader) were used to fill the canal until the spreader could not penetrate into the canal by more than 2mm.
Excess gutta-percha was removed by an excavator, and a cold plugger was used to pack the root filling at the orifice for 5 seconds. Finally, the orifice was sealed with auto-polymerizing glass ionomer cement (GC, Japan).
CWVC group
ProTaper F3 gutta-percha (Dentsply Maillefer, Ballaigues, Switzerland) along with AH Plus resin sealer was placed in the canal, and its proper length was radiographically confirmed. It was cut 3-4mm above the working length by a plugger (Meta BioMed, Chungju, Korea) heated to 200°C to create an apical plug. Next, a radiographic image was obtained to ensure optimal quality of the apical plug. The sealer was applied again in the residual root canal space, and thermoplasticized gutta-percha was injected into the canal to fill the canal completely (FastPack; Eighteeth, China). Finally, the canal orifice was sealed with glass ionomer cement. After obturation, the teeth were incubated at 37° and 100% humidity to allow sealer setting.
All teeth kept for 24 hours in the incubator with 100% humidity and temperature of 37℃. All this procedure was carried out by a single experienced operator.
Micro-CT
The roots were scanned with a micro-CT scanner (Lotus, Behin Negareh, Iran) with 15µm pixel size, 80 kV voltage, 100 µA amperage, and 45 minutes time (per each root). To reconstruct 2D images, cross-sectional slices were obtained in the axial plane with 45-µm slice thickness perpendicular from the root apex towards the coronal region. The 2D images were reconstructed using Lotus in vivo ACQ software (Figures 1?? to 4). Negative group was used for the calibration of the micro-CT scanner. Empty spaces (voids) and filled areas were distinguished according to their density on 2D images, and were then reconstructed three-dimensionally using Lotus in vivo REC software; subsequently, their volume was calculated. The volume percentage (VP) of voids was calculated by dividing the volume of voids by the total volume of the root filling multiplied by 100, and reported separately in the different parts, and also the entire root length [ 14 ].
Micro-CT scan of the entire canal along with middle and apical third axial coronal sections in the cold lateral compaction (CLC) group
Micro-CT scan of the entire canal along with middle and apical third axial coronal sections in continuous warm vertical condensation (CWVC) group
Three-dimensional micro-CT scan of specimens in the cold lateral compaction (CLC) group
Three-dimensional micro-CT scan of specimens in the continuous warm vertical condensation (CWVC) group
Statistical analysis
Data were analyzed by SPSS version 20 (SPSS Inc., IL, USA). Accordingly, comparisons were made by one-way ANOVA, the Kruskal-Wallis, Mann-Whitney U, Bonferroni, Dunnett, Tukey, and independent t-tests at 0.05 level of significance.
Results
Table 1 presents the mean volume of voids and filled spaces, and the VP of voids in the CLC and WVC groups in the apical, middle, and coronal thirds.
Comparison of CLC and CWVC techniques regarding the mean volume of voids and filled areas and VP of voids separately in the apical, middle, and coronal thirds are shown in Table 2.
In the apical third, the mean volume of voids in the CLC group was significantly higher than that in the CWVC group (p= 0.006). The VP of voids in the CLC group was also significantly higher than that in the CWVC group (p= 0.001). The difference in the mean volume of filled space was not significant between the two groups (p= 0.478).
In the middle third, no significant difference was found between the CLC and CWVC groups in the mean volume of voids (p= 0.166), mean volume of filled space (p= 0.184), or the VP of voids (p= 0.248).
In the coronal third, no significant difference was found between the CLC and CWVC groups in the mean volume of voids (p= 0.273), mean volume of filled space (p= 0.419), or the VP of voids (p= 0.605).
Concerning the mean volume of voids and filled are-as and VP of voids in the entire root canal length, no significant difference was found between the CLC and CWVC groups in the mean volume of voids (p= 0.299), mean volume of filled space (p= 0.443), or the VP of voids (p= 0.755) in the entire root canal length (Table 3).
Discussion
This study compared the percentage of voids of single-canal maxillary second premolars by the CLC versus CWVC techniques using micro-CT. the mean volume and VP of voids in the root canals of maxillary second premolars were not significantly different between the CLC and WVC groups in this study. The lowest volume of voids was recorded in the apical third in the WVC group, which was significantly lower than that in the apical third in the CLC group. In addition, the mean volume and VP of voids in the apical third was significantly lower than the corresponding values in the middle and coronal thirds in the WVC group.
Several methods have been proposed for assessment of the quality of root canal obturation, such as the bacterial leakage model, dye penetration technique, fluid filtration technique, confocal laser scanning microscopy, radioisotope tracing, scanning electron microscopy, and cone-beam computed tomography.
Micro-CT is a novel highly accurate technique for reproducible assessment of specimens without their destruction [ 8
- 11 ]. A previous study compared micro-CT and histological analysis and revealed that micro-CT was capable of precise 3D reconstruction of root canal filling [ 12 ]. Micro-CT was developed in early 1980, as a non-invasive and non-destructive imaging modality to obtain 3D images. It operates based on convergence of X-ray beams on the specimen and their receipt by a sensor. The irradiated X-ray is then converted to digital images [ 13 ].
Keleş et al. [ 16 ] evaluated the obturation quality of oval-shaped canals filled by the CLC and WVC techniques using micro-CT. They found that the volume of voids was significantly higher in CLC group; however, the difference in this regard was not significant between the two groups in the apical third [ 16 ]. Their results were different from the present findings since in the present study, the mean volume and VP of voids were not significantly different between the two groups, but this difference was significant in the apical third. The difference between the two studies may be due to evaluation of different tooth types, and experience and expertise of the operators. Almohaimede et al. [ 17 ] compared the filling porosity of two different obturation techniques in 40 single-canal teeth using micro-CT. They compared CLC and continuous-wave techniques with gutta and AH Plus, and found that the volume of voids in the different thirds in the continuous-wave group was higher than that in the CLC group. The highest filling porosity was noted in the apical third in continuous-wave group but no statistically significant difference was found between different obturation techniques. Their results were similar to our study, with the difference that the lowest mean volume and VP of voids in the present study was recorded in the apical third of WVC group, and the two groups were not significantly different in this regard in other parts of the root. Amida et al. [ 18 ] compared the obturation sealability of CLC, GuttaCore®, and WVC technique using micro-CT. They used extracted maxillary central incisors and found the highest volume of voids in the apical third in all techniques. Although the GuttaCore® group showed fewer voids than the other two techniques, they all had similar sealing ability, and the GuttaCore® and CLC groups had no significant difference in the mean volume and VP of voids [ 18 ]. Their results, regarding no significant difference between the CLC and CWVC groups, were in agreement with the present findings. However, they reported the highest volume of voids in the apical third in all groups while the lowest volume and VP of voids were found in the apical third of CWVC group in the present study.
Both obturation techniques and both sealers produced voids, which is in accordance with the findings of Celikten et al. [ 19 ], who suggested that voids are mainly correlated with the root canal anatomy rather than the root canal filling material or technique.
The round shape of the canal may limit the penetration of the spreader in the apical part in the lateral compaction technique and prevent the insertion of the lateral gutta to the length of working. This problem does not exist in oval canals [ 20 ]. For this reason, maxillary premolar teeth, which have an oval canal, were selected for this study.
The VP of voids is commonly calculated to assess the quality of root filling [ 14 , 21 ] because bacteria and their byproducts can colonize the voids and compromise the success of the treatment. Thus, optimal seal in the entire root length is required [ 14 ]. The significantly lower mean volume and VP of voids in the apical part in WVC group may suggest the superiority of this technique to CLC in possible prevention of leakage of microorganisms in infected canals.
Considering the importance of cleaning, shaping, and appropriate obturation of the apical part to maintain seal and prevent re-contamination and presence of lateral canals, this area affects the treatment results; therefore, using the obturation method with the least amount of voids in this area is important [ 1 , 4 , 22 ].
Considering the lowest amount of voids in the apical part of the CWVC in our study, this technique will be important and effective.
The in vitro design of the study can be considered as a limitation, which confines the generalization of results to the clinical setting. Future studies are required to compare the results of micro-CT with the results of sealer dissolution and leakage in the long-term to find more reliable information regarding the long-term sealing ability of sealers and also about root fillings in different obturation techniques. Moreover, similar studies are required using silicone sealers in comparison with resin and calcium silicate-based sealers, and also different teeth with variable levels of root curvature. Crack formation should also be compared following root canal obturation with different techniques. Cone-beam computed tomography might be used for further investigations in this regard.
Conclusion
None of the tested obturation techniques could provide a void-free root filling. The CLC and CWVC techniques showed no significant difference regarding the mean and VP of voids in obturation of single-canal maxillary second premolars. The apical third in the CWVC group showed the lowest mean percentage of voids, which was significantly lower than that in the apical third of the CLC group.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Schilder H Filling Root Canals in Three Dimensions J Endod 2006 4 28129010.1016/j.joen.2006.02.00716554195 · doi ↗ · pubmed ↗
- 2Kontakiotis EG Tzanetakis GN Loizides AL A l 2-month longitudinal in vitro leakage study on a new silicon-based root canal filling material (Gutta-Flow) Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007 103 8548591744928810.1016/j.tripleo.2006.12.014 · doi ↗ · pubmed ↗
- 3Van der Sluis L Wu MK Wesselink P An evaluation of the quality of root fillings in mandibular incisors and maxillary and mandibular canines using different methodologies J Dent 2005 33 6836881602377810.1016/j.jdent.2005.01.007 · doi ↗ · pubmed ↗
- 4Whitworth J Methods of filling root canals: principles and practices Endod Topics 2005 12 224
- 5Collins J Walker MP Kulild J Lee C A comparison of three gutta-percha obturation techniques to replicate canal irregularities J Endod 20063 2 76276510.1016/j.joen.2005.10.00116861078 · doi ↗ · pubmed ↗
- 6Tasdemir T Yesilyurt C Ceyhanli KT Celik D Er K Evaluation of apical filling after root canal filling by 2 different techniques J Can Dent Assoc 2009 75 201ad 19356318 · pubmed ↗
- 7Cavenago BC Duarte MAH Ordinola-Zapata R Marciano MA Carpio-Perochena A Ed Bramante CM Interfacial adaptation of an epoxy-resin sealer and a self-etch sealer to root canal dentin using the System B or the single cone technique Braz Dent J 2012 23 2052112281468710.1590/s 0103-64402012000300004 · doi ↗ · pubmed ↗
- 8Hwang JH Chung J Na HS Park E Kwak S Kim HC Comparison of bacterial leakage resistance of various root canal filling materials and methods: Confocal laser‐scanning microscope study Scanning 2015 37 4224282611442110.1002/sca.21231 · doi ↗ · pubmed ↗