Antibiotic Resistance to Pseudomonas Aeruginosa in the Saliva of Candidates of Bone Marrow Transplantation
Maryam Zahed, Mojtaba Safvat, Abdollah Bazargani, Janan Ghapanchi, Zahra Ranjbar

TL;DR
This study examines antibiotic resistance in Pseudomonas aeruginosa from saliva samples of bone marrow transplant candidates, finding high resistance to certain antibiotics.
Contribution
The study identifies specific antibiotic resistance patterns in Pseudomonas aeruginosa among immunocompromised patients, guiding more effective treatment strategies.
Findings
Pseudomonas aeruginosa showed 100% resistance to Penicillin and Oxacillin in tested patients.
Vancomycin demonstrated the highest effectiveness with 20% susceptibility.
No significant correlation was found between resistance and patient age, gender, or disease type.
Abstract
Opportunistic infections such as Pseudomonas aeruginosa, colonized from the oral cavity, are common in candidates of bone marrow transplantation. Therefore, it is important to prescribe appropriate antibiotics for this group of debilitated patients. In this study, we aimed to investigate the antibiotic resistance to Pseudomonas aeruginosa encountered in candidates of bone marrow transplantation referred to Imam Reza Clinic, Namazi Hospital, and Amir Hospital, Shiraz, Iran. This cross-sectional study was performed on 30 patients with leukemia and lymphoma. To identify Pseudomonas species, saliva samples were collected and cultured in a blood agar medium. Considering the present therapies, we examined the antibiotic sensitivity of Penicillin, Oxacillin, Gentamicin, Tetracycline, Cefepime, Ciprofloxacin, Imipenem, Ceftazidime, Cefotaxime, Erythromycin, Trimethoprim, Sulfamethoxazole, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
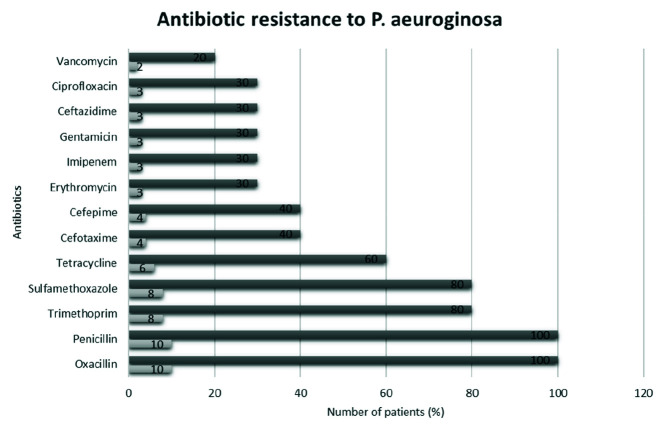 Figure 1
Figure 1| Antibiotics | Age of each patient | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 8 | 11 | 14 | 23 | 30 | 46 | 64 | |||||||||
| N | (%) | N | (%) | N | (%) | N | (%) | N | (%) | N | (%) | N | (%) | ||
| Erythromycin | 0 | 0% | 0 | 0% | 1 | 10% | 1 | 10% | 1 | 10% | 0 | 0% | 0 | 0% | 0.267 |
| Oxacillin | 2 | 20% | 1 | 10% | 1 | 10% | 1 | 10% | 2 | 20% | 1 | 10% | 2 | 20% | - |
| Imipenem | 1 | 10% | 1 | 10% | 0 | 0% | 0 | 0% | 0 | 0% | 0 | 0% | 1 | 10% | 0.514 |
| Penicillin | 2 | 20% | 1 | 10% | 1 | 10% | 1 | 10% | 2 | 20% | 1 | 10% | 2 | 20% | - |
| Tetracycline | 0 | 0% | 0 | 0% | 1 | 10% | 0 | 0% | 2 | 20% | 1 | 10% | 2 | 20% | 0.125 |
| Trimethoprim | 2 | 20% | 1 | 10% | 1 | 10% | 1 | 10% | 1 | 10% | 0 | 0% | 2 | 20% | 0.333 |
| Gentamicin | 1 | 10% | 0 | 0% | 1 | 10% | 0 | 0% | 0 | 0% | 0 | 0% | 1 | 10% | 0.514 |
| Ceftazidime | 1 | 10% | 0 | 0% | 0 | 0% | 0 | 0% | 1 | 10% | 0 | 0% | 1 | 10% | 0.827 |
| Cefotaxime | 0 | 0% | 1 | 10% | 0 | 0% | 0 | 0% | 2 | 20% | 0 | 0% | 1 | 10% | 0.244 |
| Cefepime | 0 | 0% | 1 | 10% | 0 | 0% | 0 | 0% | 2 | 20% | 0 | 0% | 1 | 10% | 0.442 |
| Sulfamethoxazole | 2 | 20% | 1 | 10% | 1 | 10% | 1 | 10% | 1 | 10% | 0 | 0% | 2 | 20% | 0.333 |
| Ciprofloxacin | 1 | 10% | 0 | 0% | 0 | 0% | 1 | 10% | 0 | 0% | 0 | 0% | 1 | 10% | 0.514 |
| Vancomycin | 0 | 0% | 1 | 10% | 0 | 0% | 0 | 0% | 1 | 10% | 0 | 0% | 0 | 0% | 0.333 |
| Total Number of patients in each group of age | 2 | 20% | 1 | 10% | 1 | 10% | 1 | 10% | 2 | 20% | 1 | 10% | 2 | 20% | Total 10 (100%) |
| Antibiotics | Gender | ||||
|---|---|---|---|---|---|
| Male | Female | ||||
| N | (%) | N | (%) | ||
| Erythromycin | 1 | 10% | 2 | 20% | 0.490 |
| Oxacillin | 5 | 50% | 5 | 50% | - |
| Imipenem | 2 | 20% | 1 | 10% | 0.490 |
| Penicillin | 5 | 50% | 5 | 50% | - |
| Tetracycline | 2 | 20% | 4 | 40% | 0.197 |
| Trimethoprim | 4 | 40% | 4 | 40% | 1.000 |
| Gentamicin | 1 | 10% | 2 | 20% | 0.490 |
| Ceftazidime | 2 | 20% | 1 | 10% | 0.490 |
| Cefotaxime | 3 | 30% | 1 | 10% | 0.197 |
| Cefepime | 2 | 20% | 2 | 20% | 1.000 |
| Sulfamethoxazole | 4 | 40% | 4 | 40% | 1.000 |
| Ciprofloxacin | 1 | 10% | 2 | 20% | 0.490 |
| Vancomycin | 2 | 20% | 0 | 0% | 0.114 |
| Antibiotics | Disease | |||
|---|---|---|---|---|
| Lymphoma | Leukemia | |||
| N | (%) | N | (%) | |
| Erythromycin | 1 | 10% | 2 | 20% |
| Oxacillin | 4 | 40% | 6 | 60% |
| Imipenem | 2 | 20% | 1 | 10% |
| Penicillin | 4 | 40% | 6 | 60% |
| Tetracycline | 1 | 10% | 5 | 50% |
| Trimethoprim | 4 | 40% | 4 | 40% |
| Gentamicin | 2 | 20% | 1 | 10% |
| Ceftazidime | 1 | 10% | 2 | 20% |
| Cefotaxime | 1 | 10% | 3 | 30% |
| Cefepime | 1 | 10% | 3 | 30% |
| Sulfamethoxazole | 4 | 40% | 4 | 40% |
| Ciprofloxacin | 1 | 10% | 2 | 20% |
| Vancomycin | 1 | 10% | 1 | 10% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Bacterial Identification and Susceptibility Testing · Antimicrobial Resistance in Staphylococcus
Introduction
Cancers are one of the biggest global health problems after cardiovascular disease, traumatic events, and major crises in the world [ 1 ]. The prevalence of leukemia and lymphoma in Iran is significantly high [ 2 ]. Acute leukemia is responsible for more than 10,000 deaths per year despite improved treatment regimens and new cytostatic drugs [ 3 ] and infection is one of the most serious complications and the leading cause of death in patients with acute leukemia [ 4
- 5 ]. Opportunistic infections are common in individuals with leukemia and lymphoma due to immunodeficiency caused by immature leukocytes or chemotherapy and the use of broad-spectrum antibiotics [ 6
- 7 ]. In the early stages of leukemia and lymphoma, leukopenia may occur as a result of bone marrow suppression and extensive proliferation of white blood cells (WBCs). Agranulocytosis, pancytopenia, and leukopenia also occur, which are commonly the result of drug toxicity. In addition, cyclic neutropenia, a periodic decrease in neutrophils, is also seen in association with leukemia, lymphoma, or drug therapy [ 6 ].
Pseudomonas aeruginosa (P. aeruginosa) is present in the normal flora of the intestine and the surface of human skin and it is an important pathogen in these locations. It is an opportunistic bacterium involved in a variety of acute and chronic urinary tract infections, respiratory system infections, inflammation of the skin, soft tissue infections, bacteremia, bone and joint infections, various gastrointestinal infections, and systemic infections, especially in patients with severe burns. This bacterium is mainly found in people with host defense deficiencies such as cancer, human immunodeficiency virus (HIV) and cystic fibrosis (CF) and it is a significant cause of death in such patients [ 8 ]. This microorganism is also abundant in a variety of water resources, especially in environments such as hospitals [ 9 ] and health care centers [ 9
- 10 ]. It is shown that the oral cavity can be a reservoir for P. aeruginosa in debilitated patients [ 10
- 11 ]. Tonsillar crypts, tongue, and gingiva can be considered a reservoir for this bacteria [ 11
- 12 ]. Moreover, patients positive with subgingival P. aeruginosa are reported to show a higher percentage of periodontal sites with suppuration on probing, greater periodontal attachment loss, and much more aggressive forms of periodontitis [ 11 ].
Infections caused by this pathogen are often difficult to treat due to multiple drug resistance and sometimes, more advanced antibiotic drug regimens are required leading to numerous side effects. In fact, over the past few years, P.aeruginosa has shown increasing resistance to many antimicrobial drugs, including Carbapenems and β-lactam antibiotics that are widely used in clinical practice [ 13 ]. Moreover, not only prophylactic treatments such as mouthwashes do not sufficiently reduce the bacterial load in the mouth and larynx but also they cannot prevent aspiration pneumonia in at-risk patients, especially in cases with underlying pathologies such as blood malignancies [ 14 ]. Therefore, oral examination is still necessary to improve treatment strategies, especially for patients with hematologic malignancies.
Previous studies have shown an increase in P. aeruginosa resistance to routine antibiotics [ 10 , 15
- 17 ], especially Penicillin [ 15 ]. Ten-year cross sectional studies have also shown an increase in resistance to antibiotics such as Co-amoxiclav (Amoxicillin / Clavulanic acid), Tetracycline, and Imipenem [ 18
- 19 ].
Since patients with leukemia and lymphoma are prone to opportunistic infections such as P.aeruginosa, and given that this bacterium can be isolated from the saliva, this study aimed to evaluate the antibiotic resistance of P. aeruginosa in the saliva of candidates of hematopoietic stem cell transplantation (HSCT) in Shiraz, Iran. It is important to prescribe appropriate antibiotics to prevent antibiotic resistance in these patients.
Materials and Method
This cross-sectional study was performed in May-December 2019 on 30 patients with a history of leukemia or lymphoma, candidates of bone marrow transplantation referred to Imam Reza Clinic, Namazi Hospital, and Amir Hospital, Shiraz, Iran. In the study group, 30 patients with history of lymphoma and leukemia were included after signing an informed consent form. The sample size was chosen according to a previous study [ 20 ]. All patients had finished their chemotherapy course and they were not on any medications at the time of the study. Patients who had not used systemic corticosteroids for the past 2 months or topical corticosteroids for the past 2 weeks were included. Patients with diabetes, acquired immunodeficiency syndrome (AIDS), systemic diseases affecting the immune system (including autoimmune diseases and thyroid diseases), and patients who had used mouthwashes and antibiotics in the past month were excluded from the study.
Ethical Considerations
The study was in accordance with the declaration of Helsinki and approved by the Ethics Committee of Shiraz University of Medical Sciences. (IR.SUMS. DENTAL.REC.1399.124)
Sample Collection
Participants were abstained from eating and drinking for half an hour before sampling. A total of 3cc of non-stimulating saliva was collected. Their saliva samples were sent to the microbiology laboratory in a transport environment through a cold chain. Samples were cultured in blood agar medium and incubated at 37°C for 24 hours. To separate P. aeruginosa blood agar culture, gram staining, catalase and oxidase tests were used.
Microscopic Gram Staining and Biochemical Tests
The microscopic examination of the bacterial isolates cells was carried out using an inoculation loop to transfer a part of a young colony. The colony was mixed with a drop of water and then spread on the surface of a slide and left to dry, then fixed with heat over a gentle flame and stained with gram stain and examined under the microscope where the shapes and arrangement of bacterial cells were observed. In addition, the colors that result from the interaction of bacteria with the dye were examined.
Biochemical tests were done, such as the catalase test to determine the ability of the isolates to produce the catalase enzyme that breaks down hydrogen peroxide into water and oxygen gas, and the oxidase test to evaluate the ability of bacterial colonies to produce the oxidase enzyme. These tests were all conducted according to standard methods [ 21 ].
Antibiotic Resistance
To determine the pattern of antibiotic susceptibility and resistance of Pseudomonas isolates, a disk diffusion test (Kirby-Bauer) was used. Considering the present therapies, a variety of antibiotics including Penicillin, Oxacillin, Gentamicin, Tetracycline, Cefepime, Ciprofloxacin, Imipenem, Ceftazidime, Cefotaxime, Erythromycin, Trimethoprim, Sulfamethoxazole, and Vancomycin were examined to determine antibiotic sensitivity. The microbial suspension was first prepared for all collected strains and then cultured on Mueller-Hinton agar medium (Merck, Germany) with a sterile swab, after which antibiotic discs were implanted with sterile forceps. The plates were incubated at 35°C for 24-48 hours. Then the diameter of growth halos was measured with a ruler and its interpretation was performed according to the recommendations of the Clinical and Laboratory Standard Institute (CLSI) table. Disks quality control was checked using ATCC 27853 strain [ 2 ].
Statistical Analysis
Statistical analysis was performed by chi-square test (χ^2^) with Statistical Package for the Social Sciences (SPSS Inc.; Chicago, IL, USA) version 18. The results were presented in the form of descriptive statistics in terms of relative frequency. The correlation analysis was based on p Values, and p Value < 0.05 was considered significant.
Results
From 30 bone marrow transplant candidates, 12 were suffering from lymphoma and 18 were leukemic patients. 10 cases (4 lymphomas and 6 leukemic patients; 33.33%) were positive for P. aeruginosa and their resistance pattern was evaluated. The pattern of P. aeruginosa antibiotic resistance in all patients is presented in Figure 1. P. aeruginosa was resistant to Penicillin and Oxacillin (100%) in all cases, followed by Trimethoprim and Sulfamethoxazole (80%). The best performance was seen in Vancomycin (20%).
The distribution pattern of P. aeruginosa antibiotic resistance in candidates of bone marrow transplant
Antibiotic resistance in relation to age, gender, and type of disease is presented in Tables 1?-3, respectively. According to Table 1, there was no significant relationship between age and antibiotic resistance of this bacteria (p> 0.05). In the case of Penicillin and Oxacillin, all patients were resistant to these antibiotics. Concerning gender, there was no significant relationship between this variable and antibiotic resistance of P. aeruginosa (p> 0.05) (Table 2). In addition, there was no significant relationship between the type of disease and antibiotic resistance of the bacteria (p> 0.05) (Table 3).
Discussion
This study aimed to evaluate the pattern of P. aeruginosa antibiotic resistance among bone marrow transplant patients. The results showed no significant relationship between the three factors of age, gender, and type of disease (leukemia and lymphoma) for the pattern of P. aeruginosa antibiotic resistance among bone marrow transplant patients. However, a complete resistance of Penicillin and Oxacillin was observed against this bacterium. Cefepime and Trimethoprim had 80% resistance and Vancomycin showed the best performance with only two cases (20%) of resistance.
Resistance to antimicrobials is a serious problem for human health worldwide. This has been associated with increased patient mortality, delays in hospitalization, and increased costs [ 22 ]. In recent years, this problem has arisen due to the rapid proliferation of Metallo-β-lactamases that mediate resistance to Carbapenems (such as Imipenem) among gram-negative bacilli [ 23 ]. In 2017, for the first time, the World Health Organization (WHO) published a list of drug-resistant bacteria that were in atrocious need of new antibiotics. In this list, P. aeruginosa was ranked at the critical level having resistance to Carbapenem. Antibiotic resistance kills almost 700,000 people a year worldwide and some experts predict that this number will reach to 10 million by 2050 [ 24 ].
A 2019 study by Jarlier et al. [ 15 ] showed an 8.9% prevalence of P. aeruginosa in 30 different countries, with significant percentages of resistance to third-generation Cephalosporins, Carbapenems, and Fluoroquinolones. In another study, it is shown that patients who were infected more than once with P. aeruginosa were younger than those who were infected only once. These patients spent more days in the hospital and the intensive care unit (ICU). They underwent biopsy and transplantation; they were exposed to invasive medical devices, and were diagnosed with cystic fibrosis and kidney disease. They also took antibiotics other than Penicillin for longer periods [ 16 ]. In addition, more recurrences of gram-negative bacterial infections in the hospital were associated with a higher risk of drug-resistant infections [ 17 ]. For patients with recurrent P. aeruginosa infections, the risk of drug resistance was increased by 23% compared to any previous hospital infection. Moreover, approximately 15% of these infections became drug-resistant afterwards and 44% remained drug-resistant [ 17 ].
Besides, infection with gram-negative bacteria is found to be common after hematopoietic stem cell transplantation (HSCT) and organ transplantation and it is associated with high mortality rates [ 24
- 25 ]. Infections can also affect the life quality of such patients [ 26
- 27 ]. In Satlin and Walsh’s study 2017 [ 28 ], the results showed that P. aeruginosa was increasingly found in the bloodstream of HSCT patients and the prognosis of subjects infected with these bacteria was worse than patients infected by more susceptible bacteria.
Concerning the history of antibacterial resistance for this bacterium, we can refer to the study of Ramos et al. [ 18 ], which was conducted in Brazil over a period of 10 years (1998-2008). This study examined the presence of Pseudomonas resistance to Tetracycline and β-lactams in the oral cavity of patients with gingivitis, periodontitis, healthy individuals, and patients with complete prosthetics. Out of 15 positive samples, 86.7% were resistant to Co-amoxiclav, 73.3% Tetracycline and 13.3% Imipenem. These results show less resistance compared to our report (60% Tetracycline and 30% Imipenem). This difference cannot directly indicate an increase in resistance after a decade because other studies show a noticeable difference in the same period. [ 19 , 29 ] Another ten-year study from 2002 to 2011 at the Tunis Bone Marrow Transplant Center [ 19 ], 210 isolates of P. aeruginosa showed 32.8% resistance to Imipenem and/or Ceftazidime. The rate of resistance per 1000 days of illness increased from 2.07 to 2.21 [ 19 ]. This result is similar to the result (30%) obtained from our study.
Oliveira et al. [ 29 ] conducted a study in 2004 at 13 hematopoietic stem cell transplant centers in 10 Brazilian cities. A total of 411 patients with various types of cancer including myeloma and lymphoma were examined. Their results showed that 22% of isolates belonged to P. aeruginosa. Despite the results of our study, P. aeruginosa isolates were resistant to Imipenem (4/5), Ceftazidime (5/5), Ciprofloxacin (4/5), and Cefepime (5/5). One of the risk factors mentioned for multidrug resistance gram-negative bacteria was previous exposure to third-generation Cephalosporins and attending a specific transplant center.
A retrospective study by Agarwal and Larson [ 16 ] from 2012 to 2017 was conducted to assess the incidence of microbiological characteristics and risk factors associated with bacteremia in children candidates of hematopoietic stem cell transplantation. All Pseudomonas species isolated from the bloodstream showed resistance (1 case as multiple resistance and 4 cases as Carbapenem-resistant). A study in Libya [ 30 ] evaluated the antimicrobial susceptibility of P. aeruginosa in 46 patients admitted to the Burn and Plastic Surgery Center from 2013 to 2014. These patients had previously shown resistance to Ertapenem, Imipenem, and Meropenem. When comparing this study to our study, very high resistance of isolates of gram-negative bacilli against Carbapenem and multiple resistances in all isolates, including Gentamicin 45 (98%), Ceftazidime 42 (91%), Cefepime 39 (85%), and Ciprofloxacin 45 (98%) were observed [ 30 ].
A study of drinking water samples from various environments, including health centers in 2017 [ 31 ] reported that although Imipenem was still considered a front-line antibiotic against P. aeruginosa, the persistent increase in resistance was detected. This study emphasizes the role of purines as an effective factor in Carbapenem resistance in gram-negative bacteria [ 31 ]. In addition, another study identifies mutations that, among other reports, indicate a new resistance mechanism that may play a role in Imipenem resistance for P. aeruginosa [ 32 ].
Combination therapy can help maximize bacterial killing, minimize resistance, or both [ 33 ]. In the study of Kraiem et al. [ 30 ], only Colistin showed excellent performance against P. aeruginosa. However, the data showed that the center's staffs prevent the use of Colistin in the treatment of serious infections due to concerns about nephrotoxicity. The results of a similar study showed that a combination of Colistin and Amikacin might be effective in the treatment of Metallo-β-lactamases of Carbapenem-resistant gram-negative bacilli in serious life-threatening infections [ 29 ]. Although limited cases of Colistin resistance has been interpreted, the beginning of its resistance development has been announced [ 34 ]. An important issue that is being mentioned in literature nowadays is the effect of chemotherapy on enhancing antibiotic resistance. It is hypothesized that cancer chemotherapeutic compounds can damage bacterial DNA, which in turn enhances the bacterial mutation rate. Antibiotic resistance occurs after mutation of bacterial core genes. [ 35 ] Meunier et al. [ 35 ] showed that chemotherapy accelerates evolution of the microbiota and drive the emergence of antibiotic-resistant mutants from bacterial commensals in patients in an in vitro study. This matter also emphasizes the importance of antibiotic resistance studies in this group of patients.
It is worthy to mention that salivary samples were chosen in this study due to smaller sample fraction, good patient compliance, easy collection (without specialized equipment or personnel), easy storage and transportation, cost effectiveness, greater sensitivity, and correlation with levels in blood [ 35
- 36 ]. In addition, as mentioned previously, this bacterium is isolated from the oral cavity and the saliva can be a non-invasive biomarker that can predict the susceptibility to pulmonary P. aeruginosa [ 11
- 12 , 36 ].
Moreover, it can be stated that the results obtained from most of the studies [ 15
- 16 , 19 , 29
- 30 ] mentioned were in line with the results of the present study. In some cases, differences in percentages may be rooted in differences in the number of study samples. One of the limitations of our study was the small sample size due to the COVID-19 pandemic, which did not allow further data to be collected. Besides, other factors such as site of sampling, which was saliva in the present study, can play a role in the different results seen with other studies. In most studies, open wounds and mucus were common sites of sample collection. The lack of a significant relationship between antibiotic resistance and age, gender, or type of disease was predictable due to the small statistical population. Future studies with larger sample sizes are suggested.
Conclusion
The results of this study show the ineffectiveness of the Penicillin family against P. aeruginosa. Tetracycline and Sulfamethoxazole also did not show promising results. Cefotaxime, Gentamicin, Ceftazidime, and Cipro-floxacin and Cefepime were less resistant in the present study than in other studies. This may indicate the therapeutic potential of these drugs in Iran. Further research is needed to achieve more reliable results for previously mentioned antibiotics. None of the articles reviewed mentioned Trimethoprim and Vancomycin. The poor performance of Trimethoprim requires further study. However, Vancomycin along with its noticeable performance makes it more valuable for further research and use.
Data Availability
The data supporting the findings of this study are available upon reasonable request from the corresponding author. However, restrictions were applied to the public availability of these data, because of the patient's confidentiality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Qin TJ Mi YC Feng SZ Li DP Wei JL Yang D Letal Clinical study on fluoroquinolone prophylaxis in neutropenia patients with acute leukemia Natl Med J China 2007 87 1389139317785058 · pubmed ↗
- 2Abdollahi A Hakimi F Doomanlou M Azadegan A Microbial and antibiotic susceptibility profile among clinical samples of patients with acute leukemia Int J Hematol Stem Cell Res 2016 10 6169 PMC 488815027252805 · pubmed ↗
- 3Dores GM Devesa SS Curtis RE Linet MS Morton LM Acute leukemia incidence and patient survival among children and adults in the United States, 2001-2007 Blood 2012 119 34432208641410.1182/blood-2011-04-347872 PMC 3251235 · doi ↗ · pubmed ↗
- 4Delavigne KBérard E Bertoli S Corre J Duchayne E Demur Cetal Hemophagocytic syndrome in patients with acute myeloid leukemia undergoing intensive chemotherapy Haematologica 2014 99 474802414299810.3324/haematol.2013.097394 PMC 3943310 · doi ↗ · pubmed ↗
- 5Saini L Rostein C Atenafu EG Brandwein JM Ambulatory consolidation chemotherapy for acute myeloid leukemia with antibacterial prophylaxis is associated with frequent bacteremia and the emergence of fluoroquinolone resistant E. Coli BMC Infect Dis 2013 13 172380025610.1186/1471-2334-13-284PMC 3694510 · doi ↗ · pubmed ↗
- 6Aota K Kani K Yamanoi T Momota Y Ninomiya M Yumoto Hetal Management of tooth extraction in a patient with ELANE gene mutation-induced cyclic neutropenia: A case report Medicine (Baltimore). 2019 98 e 173723157488510.1097/MD.0000000000017372 PMC 6775366 · doi ↗ · pubmed ↗
- 7Wingard JR Hsu J Hiemenz JW Hematopoietic stem cell transplantation: An overview of infection risks and epidemiology Infect Dis Clin North Am 2010 24 2572722046626910.1016/j.idc.2010.01.010 · doi ↗ · pubmed ↗
- 8Balasubramanian D Schneper L Kumari H Mathee K A dynamic and intricate regulatory network determines Pseudomonas aeruginosa virulence Nucleic Acids Res 2013 41 1202314327110.1093/nar/gks 1039 PMC 3592444 · doi ↗ · pubmed ↗