The Prevalence of Temporomandibular Disorder in Iran: A Literature Review
Sajad Ghorbanizadeh, Kamran Azadbakht, Hamid Badrian, Nakisa Torabinia

TL;DR
This study reviews how common jaw joint disorders are in Iran, finding they affect more than half of the population.
Contribution
This paper provides a comprehensive meta-analysis of TMD prevalence in Iran using PRISMA guidelines and multiple databases.
Findings
The pooled prevalence of TMD in Iran is 56% (95% CI: 44-68%).
TMD is prevalent among children and students in some regions of Iran.
The study highlights the need for early examinations and education to prevent TMD.
Abstract
Temporomandibular joint disorder (TMD) will appear if there is a problem with the temporomandibular joint, bones, related muscles, or ligaments. This complication causes severe joint pain near the ears, head, neck, and jaws. TMD has been reported to affect 40 to 70% of adults. Based on previous studies, the present review aimed to determine the prevalence of TMD among the Iranian population. This review and meta-analysis was performed according to the PRISMA guidelines. All relevant studies published during 2000-2023 were retrieved by a systematic search in available international databases, including Web of Science, Science Direct, Scopus, PubMed, and Google Scholar, and domestic Persian databases, including SID, Magiran, and Iran Medex. Finally, 22 completely related studies were selected to investigate the main objective. The Comprehensive Meta-analysis (CMA) software was used for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
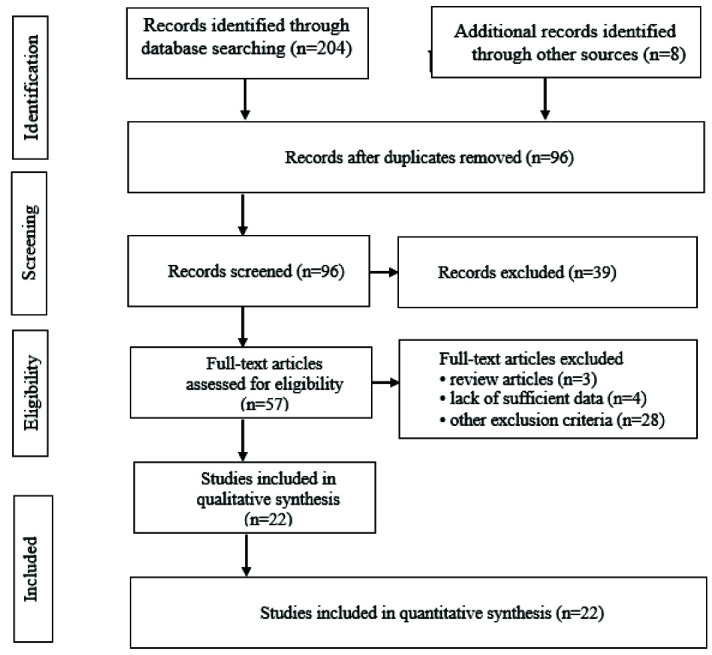 Figure 1
Figure 1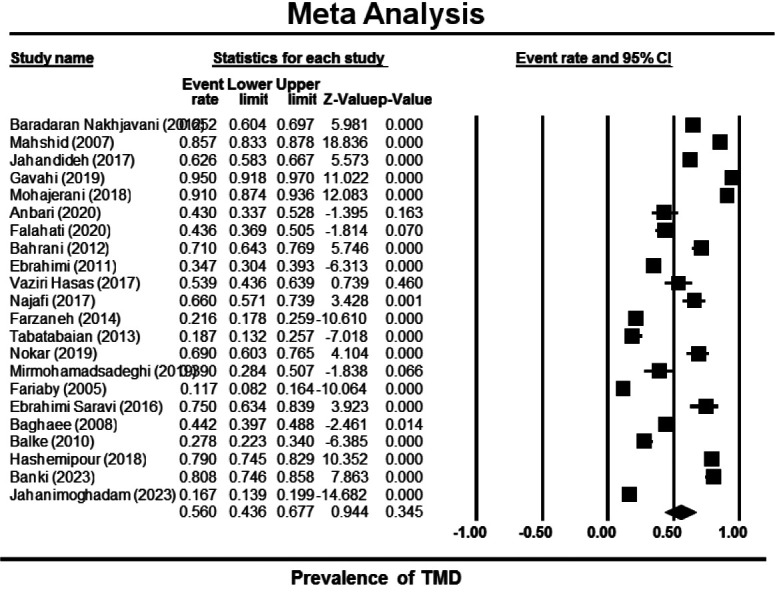 Figure 2
Figure 2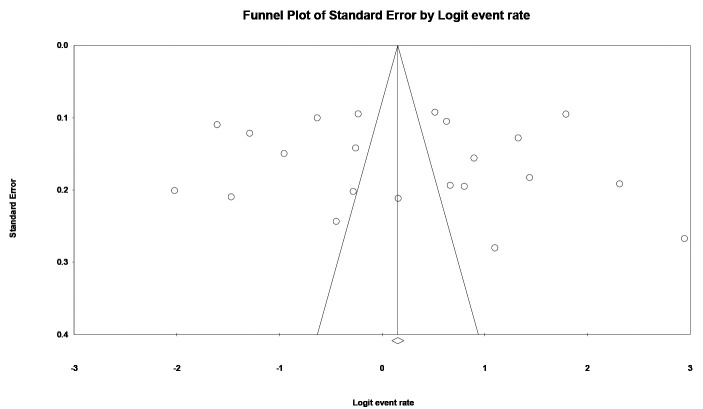 Figure 3
Figure 3| Authors (study year) | Research population | Study location | Age category (year) | Gender (sample, size, person) | Prevalence of TMD (%) | Other key results |
|---|---|---|---|---|---|---|
| Baradaran Nakhjavani | Elementary school students | Tehran | Range: 7-9 | Female (205) and male (195) | 65.2 | Class III occlusion, bruxism, and Deep Bite |
| Mahshid | Ordinary people | Tehran | Range: 18-77 | Female (839) and male (64) | 85.7 | Bruxism and trauma |
| Jahandideh | Patients referred to dentistry centers | Rasht | Range: 7-9 | Female (282) and male (218) | 62.6 | |
| Gavahi | Patients with mandibular fracture | Yazd | Range: 3-59 | Female (70) and male (225) | 95 | |
| 7-9 | ||||||
| Mohajerani | Patients referred to dentistry centers | Tehran | <27, 27-45, >45 (193) and male (141 | Female Three groups | 91 | |
| Anbari | Law students | Bandar-e- Anzali | Range: 18-25 | Female (67) and male (33) | 43 | Hidden anxiety |
| Falahati | Patients referred to dentistry centers | Isfahan | Mean: 33.8 | Female (101) and male (101) | 43.6 | Orthodontic treatment ( |
| Bahrani | Dental and non-dental students | Shiraz | Range: 18-30 | Female (100) and male (100) | Dental students: 80 | |
| Non-dental students: 62 | ||||||
| Ebrahimi | High school students | Mashhad | Range: 14-18 | Female (400) and male (40 | 34.7 | Clicking, muscle tenderness and temporomandibular joint (TMJ) tenderness |
| Banki | dental student | Golestan | Range: 18-28 | 98 male-95 females | 80.8 | Bruxism and trauma history |
| Nokar | Patients with TMD | Tehran | Range: 15-65 | Female (65) and male (58) | 69 | Occlusal factors playing a role in the etiology of TMD |
| Mean: 36.6 | ||||||
| Mirmohamadsadeghi | Patients with and without TMD chosen before the third molar surgery | Tehran | Range: 15-30 | Total female and male (71) | 39 | - |
| Mean: 24.3 | ||||||
| Fariaby and Mohammad (2005) [ | Elementary school students | Kerman | Range: 9-12 | Male (240) | 11.7 | Limitations in mouth opening, deviation in jaw opening |
| Ebrahimi Saravi | Patients referred to dentistry center | Sari | NR | Female (41) and male (27) | 75 | Among 68 patients, muscle pain |
| Jahanimoghadam | Elementary school students | Kerman | Mean: 9.18 | 327 male-273 female | 16.5 female- 16.9 male | Awake and sleep bruxism |
| Baghaee | Preschool children | Mashhad | 6 | Female (221) and male (231) | 44.2 | Clicking, crepitus, deviation |
| Balke | Attendees of medical healthcare centers | Mashhad and Zoshk | Urban: [range: 18-64, mean: 33.68± 10.31] | Female (171) and male (52) | Urban: 24.4 | Disc displacement |
| Rural: [range: 18-65, mean: 32.07± 10.83] | Rural: 31.7 | |||||
| Hashemipour | First- to-fourth-grade high school students | Kerman | Range: 14-18, Mean: 15.0±1.1 | Total female and male (368) | 79 | Pain in masticatory muscles, pain at mouth opening |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTemporomandibular Joint Disorders · Oropharyngeal Anatomy and Pathologies · Orthodontics and Dentofacial Orthopedics
Introduction
Temporomandibular joint (TMJ) is important for chewing, swallowing, speaking, and even breathing. In addition, TMJ is the only joint in the body that is made of the connection between two symmetrical joints that act in harmony [ 1 ]. Therefore, temporomandibular disorder (TMD) is a term that refers to problems with the masticatory system, which includes the TMJ, the musculoskeletal system, and the supporting bone. TMD has been reported to affect 40 to 70% of adults, while its prevalence in children with deciduous teeth and a mixed dental system reaches 16% and 90% [ 2
- 5 ].
TMD is a multifactorial disease with acquired and hereditary factors. The acquired factors include infection, injuries, surgery, radiation therapy, habits, tumors, etc. The hereditary factors consist of hemifacial microsomia, hemifacial atrophy, juvenile rheumatoid arthritis, oncology, muscle spasm, ectopic occlusal contact, stress, systemic disease, and immunological factors [ 5 ].
To diagnose the signs and symptoms of TMD, a complete medical and dental history is first obtained from the patient to discover any hereditary or acquired disorder. In addition, a history of trauma and pain should be provided. Then, the patient’s clinical examination begins with palpation of the posterior temporal, medial, and anterior muscles, a superficial and deep masseter, lateral pterygoid, sternocleidomastoid, superior trapezius, suboccipital and posterior neck muscles [ 5
- 7 ]. Then, several parameters are essential to be considered, which include touching the TMJ in the opening and closing position of the mouth, lateral movements, pain in touching, the presence of joint sounds, initial deviation in opening the mouth, jaw returning to the middle position (deviation), continuous deviation of the jaw to the end deflection, the patient’s degree of prevention, and occlusion [ 5 ].
The most common signs and symptoms of TMD are hamstring and TMJ pain, muscle dysfunction, joint sounds, headache, abnormal jaw movement, mouth opening, abrasions, and tingling [ 3 , 5 , 8
- 9 ]. It should be noted that the incidence of TMD symptoms increases with age increase [ 8 ]. Children, however, have difficulties describing pain and identifying its source, and the relationship between signs and symptoms is not clear in children [ 5 ].
Since TMD is the most common jaw disorder that affects the masticatory muscles, bony components of the TMJ, and soft tissue fragments of TMJ (especially the articular disc and ligament joints), it is important to survey this complication in society. In addition, no review study has been conducted on the prevalence of TMD in Iran, so it is necessary to conduct a systematic review to shed more light on this lacuna.
Materials and Method
Searched databases and search strategy
This study aimed to investigate the prevalence of TMD among the Iranian population. For this purpose, systematic searches of internationally available databases, including Web of Science, Science Direct, Scopus, PubMed, and Google Scholar, were performed between 2000 and 2021. In addition, databases with the Persian language, such as SID, Magiran, and Iran Medex, included Farsi keywords. Systematic reviews were performed using Mesh terms "Temporomandibular", "Joint", "Disorders", "Iran", "TMD", "TMJ", "Dental" and "Prevalence", "Occlusion", "Signs", "Symptoms ","Patients" and "Dental". For other databases, the same Mesh terms were used similarly. In addition, unofficial reports, articles in a letter-to-editor format, and unpublished articles and content posted on internet sites were removed from the list of downloaded files.
Inclusion and exclusion criteria
The inclusion criteria were studies whose abstracts and full texts were available, and studies not reporting the desired statistical parameters were excluded.
Study selection and data collection
After the electronic search of all databases, screening was done in three phases by the authors separately, including phases I, II, and III, to determine the eligibility of studies. In phase I, the titles and abstracts of articles were checked, and in phase II, studies with unrelated titles or not matching the included criteria were deleted. In phase III, the final selected full-text articles were evaluated to extract the desired results. Furthermore, the references of full-text articles were thoroughly evaluated to verify that no articles were missed for inclusion in the study (reference checking). In addition, the citations from the full-text articles were checked (citation tracing) to make sure that the search was thorough and successful. The two researchers independently examined the quality and risk of bias of studies, and the disagreements between them were resolved through discussion or consultation with a third researcher. Finally, 22 published articles were reviewed in the present study (Figure 1). The literature search for articles was done according to the PRISMA guidelines [ 10 ].
Flow diagram of study identification according to PRISMA
Data analysis
The Comprehensive Meta-analysis (CMA) software was used to analyze the data. After feeding the information of the articles into the CMA, the I^2^ and Qvalue tests were used to detect the heterogeneity of the studies. If the I^2^ index was high, the random model was used; otherwise, the fixed model was employed. Begg’s and Egger’s tests as well as the funnel plot were used to evaluate the dispersion bias.
Results
Study selection
In the initial search of international and domestic data bases until April 2021, 204 articles were retrieved. The manual search also yielded 8 articles. Of these, 116 articles were duplicates and excluded. After reviewing the title and abstract of the remaining 96 articles, 39 irrelevant articles were excluded. After the fulltext analysis of the remaining 57 articles, 35 articles were excluded.
Descriptive results
In this review, the results of 22 studies were extracted, which can be seen in Table 1. These results included the study year, research population, study location, age category, gender, sample size, and prevalence of TMD. In addition, other key results for each study are presented in Table 1.
Analytical results
The meta-analysis done on previous studies showed that the pooled prevalence of TMD in Iran is 0.56 (0.44-0.68) (Figure 2). According to the funnel plot, the distribution of published studies was symmetric, and also the Begg’s test indicated no bias in the study (p Value= 0.37) (Figure 3).
The results of previous studies on the prevalence of temporomandibular disorder (TMD) in Iran
Funnel plot of standard error
Discussion
The present metaanalysis investigated the prevalence of TMD in Iran. Most of the studies included in this meta-analysis showed that the prevalence of TMD in the Iranians is relatively high (56%). According to different studies, the prevalence of TMD has been investigated in students. The results of studies done by Baradaran Nakhjavani and Fardi (2012) in Tehran, Fariaby and Mohammadi (2005) in Kerman, and Baghaee et al. (2008) [ 11
- 13 ] in Mashhad showed the prevalence of TMD among elementary school students in the age range of 7-12 years was 11.7%-65.2%. This value, however, was 79% among high school students in the studies done by Ebrahimi et al. in Mashhad (2011) and Hashemipour et al. in Kerman (2018) [ 14
- 15 ]. Some studies have also focused on the prevalence of TMD in patients referred to dental centers. In the study of Jahandideh in Rasht (2017), the prevalence of TMD was 66.6% [ 16 ], while it was reported to be 91% by Mohajerani (2018) [ 17 ] and 14.4% by Sahebi and Bostani (2010) in Tehran [ 18 ]. The prevalence of TMD has also been reported to be 43.6% by Falahati in Isfahan (2020) [ 19 ] and 91% by Ebrahimi Saravi (2016) in Sari [ 20 ].
According to these results, it can be argued that TMD disorders are the main reason for the referral of more than 40% of adults to dental clinics. The variation in the results of various studies could be related to differences in sample size, the multifactorial nature of this problem, the role of different etiologic factors, and variable diagnostic methods for the evaluation of TMD.
The most common reported symptoms of TMD were unilateral or bilateral articular sound, jaw deviation, limitation of mouth opening, muscle tenderness, and pain in the maxillary joint [ 21
- 28 ].
In most similar studies, the prevalence of TMD was higher in women than in men. For example, in the studies of Kitsoulis et al. (2011) [ 29 ], Shetty et al. (2010) [ 30 ], Mohajerani et al. (2018) [ 17 ], In addition, Lasemi Saravi et al. [ 31 ] (2008) found that gender is an influential factor in TMD frequency.
According to the studies of Jahandideh et al. (2017), Lasemi Saravi et al. (2008), and Johansson et al. (2003), the prevalence of TMD was significantly higher in people with parafunctional habit than in those without this habit and also in people with a history of trauma than in people without a history of trauma [ 16 , 31
- 32 ]. Thus, parafunctional habits and trauma can be considered the risk factors for TMD.
Based on the results of the previous studies, the prevalence of TMD is relatively high among Iranian patients referred to dental centers. Therefore, planning the necessary education for people in the community, especially the high-risk individuals (older age group, people with oral parafunctional habits, and history of trauma, jaw dislocation, and loss of posterior teeth), can effectively prevent these TMJ complications. In addition, increasing dentists’ awareness of the clinical symptoms of this disorder can help differentiate TMD pain from a variety of headaches, earaches, and other neurological pains and help treat the patients.
Limitation
There was a problem accessing some databases and full-text article.
Conclusion
In general, the pooled prevalence of TMD in Iranians is 0.56 (0.44-0.68). Oral parafunctional habits and trauma can affect the incidence of TMD. The most common symptoms of TMD include joint sounds, jaw deviation when opening the mouth, muscle tenderness, and masticatory muscle pain.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Scrivani SJ Keith DA Kaban LB Temporomandibular disorders N Engl J Med 2008 359 269327051909215410.1056/NEJ Mra 0802472 · doi ↗ · pubmed ↗
- 2Okeson JP Management of temporomandibular disorders and occlusion-E-book 2019 8th ed Elsevier Health Sciences publication USA 117124
- 3Castelo PM Gavião MB Pereira LJ Bonjardim LR Relationship between oral parafunctional/nutritive sucking habits and temporomandibular joint dysfunction in primary dentition Int J Paediatr Dent 2005 15 29361566344210.1111/j.1365-263X.2005.00608.x · doi ↗ · pubmed ↗
- 4Mackie A Lyons K The role of occlusion in temporomandibular disorders--a review of the literature N Z Dent J 2008 104 545918672830 · pubmed ↗
- 5Pinkham J Casamassimo P Fields HW Pediatric dentistry: Infancy through adolescence 2005 5th ed St. Louis WB Saunders Co. 89661
- 6Conti AC Oltramari PV Navarro RD Almeida MR Examination of temporomandibular disorders in the orthodontic patient: a clinical guide J Appl Oral Sci 2007 15 77821908910510.1590/S 1678-77572007000100016 PMC 4327217 · doi ↗ · pubmed ↗
- 7Bonjardim LR Gavião MB Pereira LJ Castelo PM Mandibular movements in children with and without signs and symptoms of temporomandibular disorders J Appl Oral Sci 2004 12 39442136515010.1590/s 1678-77572004000100008 · doi ↗ · pubmed ↗
- 8de Souza Barbosa T Miyakoda L Sde Liz Pocztaruk R Rocha CP Gavião MB Temporomandibular disorders and bruxism in childhood and adolescence: review of the literature Int J Pediatr Otorhinolaryngol 2008 72 2993141818004510.1016/j.ijporl.2007.11.006 · doi ↗ · pubmed ↗