Constitutional variants in PTEN: a frequent finding in patients with papillary tumors of the pineal region subtype B (PTPR-B) associated with isolated loss of chromosome 10
Steffen Hirsch, Ramin Rahmanzade, Kerstin Grund, Christian Sutter, Kathrin Schramm, Florian Selt, Jonas Ecker, Barbara C. Jones, Daniel Schrimpf, Martin Demmert, Ana S. Guerreiro Stücklin, Pablo Hernaiz Driever, Markus Mezger, Ines Brecht, Sasan D. Adib, Bastian Brummel

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
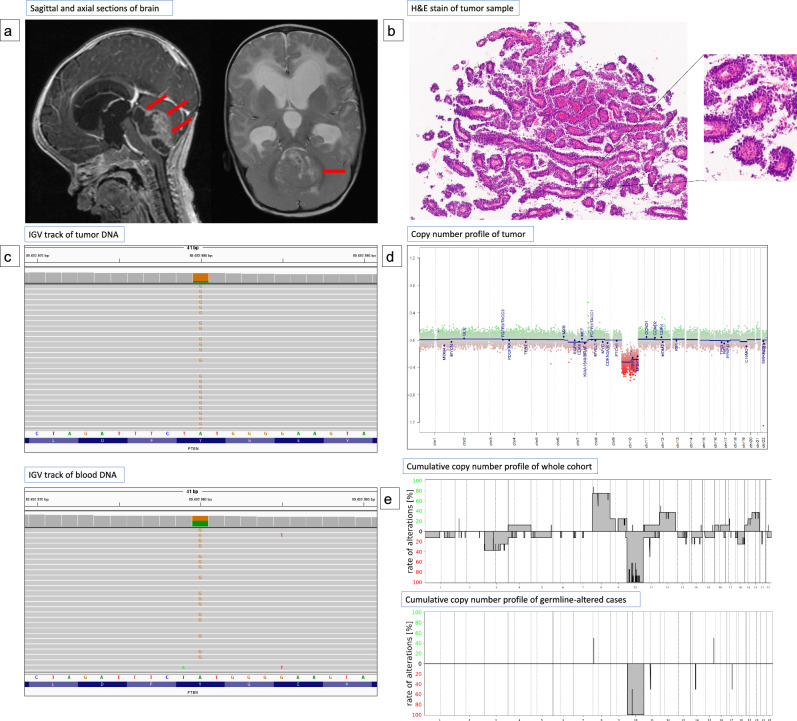 Figure 1
Figure 1- —Universitätsklinikum Heidelberg (8914)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Oncology and Treatments · Glioma Diagnosis and Treatment · Vascular Tumors and Angiosarcomas
Papillary tumors of the pineal region (PTPR) have been recognized as a distinct tumor type with characteristic histopathological features and a distinct DNA methylation profile [8, 9]. Recent studies have further elucidated the molecular and cytogenetic etiologies of PTPRs, revealing common chromosomal and genetic alterations that may contribute to our understanding of their origins and potential treatment strategies [1, 2, 5]. PTPRs can be divided into two distinct methylation subclasses, known as PTPR-A and PTPR-B. Tumors of both subclasses very frequently show loss of chromosome 10, with up to 25% of PTPR-B showing additional somatic alterations of PTEN [5–11]. The PTPR-B subgroup has recently been further classified into two distinct epigenetic subclasses, PTPR-B1 and PTPR-B2 with distinct copy number alterations and clinical courses. Tumors in the PTPR-B1 subclass frequently demonstrate loss of chromosomes 3 and 14 and are associated with a more favorable prognosis compared to those in the PTPR-B2 subclass [16].
We recently published a patient with PTPR and a constitutional variant in the PTEN gene [13]. However, to our knowledge, until now there was no information regarding the prevalence of constitutional PTEN variants among patients with PTPR-B.
To address this, we identified individuals with PTPR-B in four pediatric and young adult cancer patient registry cohorts: MNP2.0 (n = 1034), MNP Int-R (n = 806), PTT (n = 582), INFORM (n = 2909). All patients included in this analysis had been investigated by a multi-omics approach consisting of tumor DNA-methylation analysis (Illumina Infinium DNA methylation array) and paired tumor/blood sequencing using multi-gene panel (MNP2.0, MNP Int-R, PTT) or whole exome/whole genome sequencing (INFORM). Tumor copy number variation (CNV) profiles were generated using DNA methylation data. Germline sequencing data were analyzed and classified using virtual panels of established cancer predisposition genes, as previously reported [4, 13, 14]. All registries were approved by the local ethics committee.
We identified ten patients with PTPR-B in our cohorts (f/m: 6/4; age at diagnosis: 0–24 years, mean: 8 years). The demographic, clinical and molecular findings of patients are summarized in Table 1. Germline sequencing showed a constitutional heterozygous pathogenic or likely pathogenic (P/LP) PTEN variant in five individuals. Variants were either truncating (n = 4) or missense within the phosphatase domain (n = 1). Those with germline variants were significantly younger at diagnosis than those without germline variants (mean age at diagnosis 2.2 vs 14.2 years, p = 0.014). All patients with PTEN germline variant were under 5 years of age, while all patients without PTEN germline variant were 6 years or older. All patients with germline variants and available clinical information showed clinical signs of PTEN hamartoma tumor syndrome (PHTS; Table 1). In one patient (#6), PHTS was already known at the time of PTPR diagnosis.Table 1. The demographic, clinical and diagnostic findings of patients with PTPR-BIdentifierClinical informationSomatic alterationsSequencing#RegistrySexAge at diagnosis (years)Clinical signs of PHTSDNA methylation classCNV at diagnosisCNV at relapseVariant(NM_000314.4)VAF ControlVAF TumorACMG class1PTT2.0f3.2Macrocephaly, thyroid disease, trichilemmoma, fibromaPTPR-B2n/aIsolated loss of Chr. 10c.1023delTp.(Phe341Leufs3)0.350.78pathogenic2PTT2.0m24.0n/aPTPR-B1Loss of Chr. 3, 10, 14q, 22q;gain of Chr. 8, 16, 20n/aNo variant detectedn/an/an/a3MNP2.0f14.0n/aPTPR-B1Loss of Chr. 10;gain of Chr. 8, 9, 12, 19n/ac.634 + 1G > C p.?00.5n/a4MNP2.0m0.6unknownPTPR-B2Isolated loss of Chr. 10n/ac.80-1_80del p.?0.50.58likely pathogenic5MNP2.0f16.0n/aPTPR-B2Loss of Chr. 10;gain of Chr. 8n/aNo variant detectedn/an/an/a6INFORMm4.0Macrocephaly, thyroid disease, haemangioma, fibroma, developmental delay, autism spectrum disorderPTPR-B1Loss of Chr. 3, 10Isolated loss of Chr. 10c.604delp.(Thr202Leufs19)0.560.73likely pathogenic7INFORMf11.0n/aPTPR-B2n/aLoss of Chr. 3, 10, 18;gain of Chr. 8, 12No variant detectedn/an/an/a8INFORMf6.0n/aPTPR-B2n/aLoss of Chr. 10;gain of Chr. 4, 8, 9, 11,12c.394G > Tp.(Gly132Cys)00.74n/a9MNP Int-Rf0.6MacrocephalyPTPR-B2n/aIsolated loss of Chr. 10c.464A > Gp.(Tyr155Cys)0.440.82pathogenic10INFORMm2.6Macrocephaly, developmental delayPTPR-B2Isolated loss of Chr. 10Loss of Chr. 10;gain of Chr. 8, 13, 17c.634 + 5G > C p.?0.50.84pathogenicAbbreviations: ACMG American College of Medical Genetics, n/a not available, PHTS PTEN hamartoma tumor syndrome, CNV copy number variation, VAF variant allele fraction^^Case previously published [13]
We compared DNA methylation data from our cohort with a reference set of 172 PTPR tumors that were confidently classified as PTPR-A or PTPR-B (match score > 0.90) based on a previously published classification algorithm [2] from the internal database of the Neuropathology Department, Heidelberg University. Using a t-SNE analysis of the combined cohort we validated findings from a recent study that identified two epigenetic subclasses (PTPR-B1 and PTPR-B2) within PTPR-B at a larger scale (Supplementary Figs. 1 and 2) [16]. Notably, four out of five patients with constitutional P/LP PTEN variants clustered within the PTPR-B2 subclass.
Copy number analysis of tumor samples showed loss of chromosome ten including PTEN in all cases and additional copy number changes (e.g. loss of chromosome 3, gain of chromosome 8) in six cases. Loss of chromosome 10 was the only chromosomal alteration in the CNV profile of 4 out of 5 individuals with a constitutional P/LP PTEN variant, while tumors from patients lacking constitutional PTEN alterations exhibited a broader spectrum of chromosomal alterations. Figure 1 provides an overview of the radiological, histopathological, and molecular findings for patient # 9 (Fig. 1a–d) and additionally compares the cumulative CNV profiles of the entire cohort (n = 10) with those of the patients with constitutional P/LP PTEN variants (Fig. 1e). Only one patient with constitutional P/LP PTEN variant (#6) was identified to show additional CNVs (loss of chromosome 10 and 3) in the tumor analysis at diagnosis, interestingly this is the same patient mapping to the PTPR-B1 subclass and the oldest patient in our cohort with a constitutional variant. At recurrence the tumor exhibited an isolated loss of chromosome 10.Fig. 1a Sagittal contrast-enhanced and axial T2-weighted magnetic resonance (MR) sections of a 7-month-old child (# 9) depicting a large pineal mass and hydrocephalus b Hematoxylin and eosin (H&E) staining reveals characteristic papillary architecture, frequent mitoses, and necrosis (not shown), suggesting Papillary Tumor of the Pineal Region (PTPR). c Next-generation sequencing (NGS) of control DNA (bottom panel) identified a heterozygous constitutional pathogenic PTEN variant showing loss of heterozygosity in tumor DNA (top panel). d DNA methylation analysis showed isolated loss of chromosome 10 in copy number profile. e Histogram illustrating the frequency of chromosomal alterations in the overall cohort (n = 10, top) compared to those with constitutional PTEN variants (n = 5, bottom)
Our findings reveal the frequent occurrence of constitutional P/LP PTEN variants in pediatric PTPR-B, underscoring the gene’s pivotal role in tumor development. Additionally, isolated loss of chromosome 10 appears to be intricately linked with these germline alterations, suggesting that loss of PTEN function may be sufficient for tumorigenesis in this subset. These genetic insights may also have profound implications for therapeutic strategies, Targeting the PI3K/AKT/mTOR pathway may be possible in these patients. At present there is not enough data regarding the safety and efficacy of mTOR pathway inhibition in patients with PHTS and further pre-clinical and clinical evidence is required [3].
This work expands the spectrum of CNS tumors associated with PHTS that had previously been limited to benign tumors like Lhermitte Duclos disease. We suspect that PHTS is underdiagnosed in patients with PTPR as many signs or symptoms of PHTS may be falsely attributed to tumor or treatment effects. For example, macrocephaly may exclusively be attributed to hydrocephalus at tumor presentation, developmental delay may be considered to be secondary to the space-occupying lesion and thyroid disease may be considered an adverse effect of radiotherapy.
Currently, no data are available on the prevalence of PTPR among patients with PTEN hamartoma tumor syndrome. Even within the spectrum of PHTS, PTPRs are very likely a rare event. A recent review of the literature identified only 25 patients with intracranial tumors, including one case with an unspecified tumor of the pineal region [10, 12]. Imaging studies should be considered with a low threshold if symptoms consistent with an intracranial space-occupying lesion are present in young patients with PHTS.
Our findings warrant validation in larger cohorts, especially as the availability of clinical and follow-up information is limited in our registries. Larger cohorts may also allow to identify a subgroup of PHTS patients at an increased risk of developing PTPR.
As discussed above signs and symptoms of PHTS may not be recognized as such or may not yet be present at time of tumor diagnosis. Early detection of a tumor predisposing syndrome like PHTS is important, given the implications for the further management of the patient and potentially other family members [15, 17]. We propose that genetic counseling and potentially evaluation for constitutional PTEN variants should be considered in all patients with PTPR-B2 with isolated loss of chromosome 10 or a young age at diagnosis.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary Fig. 1: Unsupervised, non-linear t-distributed stochastic neighbor embedding (t-SNE) projection of DNA methylation array profiles from 182 PTPR tumor samples including cohort tumors (n = 10), a reference set of PTPR-A tumors (n = 52), and PTPR-B tumors (n = 120). The analysis recapitulates the recently proposed epigenetic subclasses of PTPR-B (PTPR-B1 and -B2) with distinct copy number profiles at a larger scale. Furthermore, 4 out of 5 patients with constitutional PTEN variants clustered within PTPR-B2. (PNG 117 KB)Supplementary Fig. 2: Cumulative summary of copy number variations (CNVs) across methylation subgroups highlights distinct CNV profiles for PTPR-B1 and PTPR-B2. Consistent with previous findings, tumors in the PTPR-B1 subgroup frequently exhibit chromosome losses in chromosomes 3 and 14. (PDF 179 KB)