The Role of Parathyroid Hormone Level as a Predictor of Hypocalcemia After Total Thyroidectomy for Thyroid Cancer: A Cross-Sectional Study
Fernando Semanate, Wilmer Tarupi, Tatiana Fernandez Trokhimtchouk, Christian Palacios, Oscar Jaramillo

TL;DR
This study shows that measuring parathyroid hormone (PTH) levels can help predict hypocalcemia after thyroid cancer surgery.
Contribution
The study demonstrates PTH's moderate predictive power for hypocalcemia after total thyroidectomy.
Findings
25.5% of patients with hypoparathyroidism experienced hypocalcemia.
PTH levels were significantly associated with post-surgical serum calcium levels.
The odds of hypocalcemia were five times higher in patients with hypoparathyroidism.
Abstract
This study aimed to investigate the utility of measuring parathyroid hormone (PTH) levels as a predictor of hypocalcemia in a population of patients undergoing total thyroidectomy for thyroid cancer between 2016 and 2019. We conducted an observational, analytical, descriptive, cross-sectional investigation, assessing PTH levels as a predictor of hypocalcemia following thyroidectomy. Among patients with hypoparathyroidism, 25.5% experienced hypocalcemia, while 74.5% had normal serum calcium levels. The likelihood of hypocalcemia was five times higher in patients with hypoparathyroidism (OR: 5.43; 95% CI: 1.89-15.6), a statistically significant finding (p < 0.05). Additionally, PTH values at 24 hours post-surgery averaged 28.9 pg/mL (SD: 30.8 pg/mL), ranging from 0.01 to 235 pg/mL. Serum calcium levels averaged 8.31 mg/dL (SD: 0.74), with values ranging from 6.5 to 10.6 mg/dL. The study…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
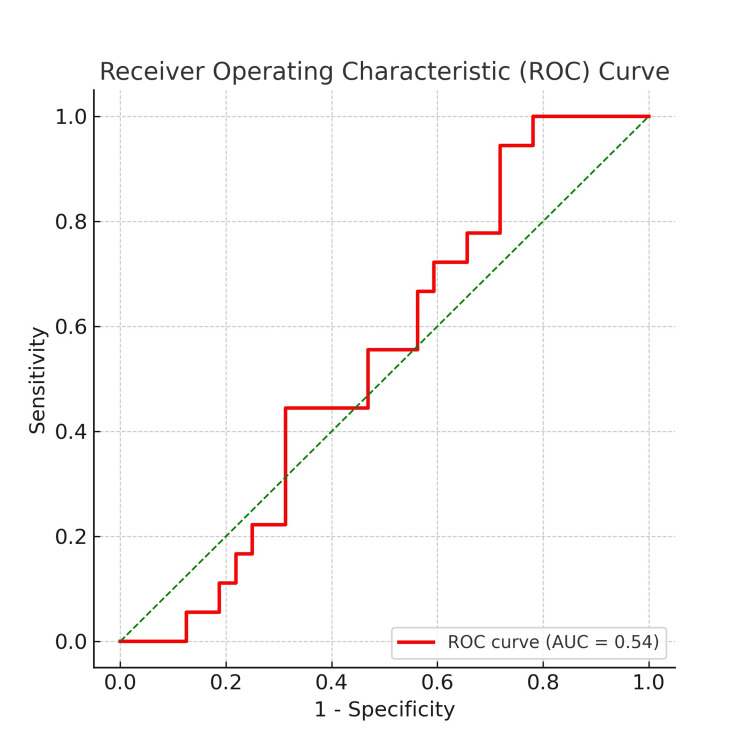 Figure 1
Figure 1| Age | Frequency (n) | Percentage (%) |
| Young adult (18-29 years) | 5 | 3.4 |
| Middle-aged adult (30-59 years) | 97 | 65.5 |
| Elderly adult (≥60 years) | 46 | 31.1 |
| Sex | ||
| Male | 23 | 15.5 |
| Female | 125 | 84.5 |
| Parathyroid hormone | Postoperative serum calcium level (mg/dL) | OR (95% CI) | Chi-square (χ²) | p-value |
| Low (<10 pg/mL) | Hypocalcemia (<7.5) (n = 12, or 25.5%) | 5.43 (1.89-15.6) | 10.52 | 0.001 |
| Normocalcemia (≥7.5) (n = 35, or 74.5%) | ||||
| Normal (≥10 pg/mL) | Hypocalcemia (n = 6, or 5.9%) | |||
| Normocalcemia (n = 95, or 94.1%) |
| Parameter | % | CI 95% |
| Sensitivity | 66.7 | 41.2-85.6 |
| Specificity | 73.1 | 64.5-80.3 |
| Positive predictive value | 25.5 | 14.4-40.6 |
| Negative predictive value | 94.6 | 87.0-97.6 |
| Positive likelihood ratio | 2.48 | 1.61-3.82 |
| Negative likelihood ratio | 0.46 | 0.24-0.88 |
| Diagnostic odds ratio | 5.43 | 1.89-15.6 |
| Model | Sum of squares | df | Mean square | F | Sig. |
| Regression | 4.880 | 1 | 4.880 | 9.436 | 0.003b |
| Residual | 75.513 | 146 | 0.517 | - | - |
| Total | 80.393 | 147 | - | - | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid and Parathyroid Surgery · Thyroid Cancer Diagnosis and Treatment · Parathyroid Disorders and Treatments
Introduction
A marked increase in the incidence of thyroid cancer has been evident worldwide over the past three decades. In Ecuador, Quito has reported some of the highest incidence rates globally, with 10.1 cases per 100,000 men and 47.0 cases per 100,000 women [1], placing it among the areas with the highest indicators globally [2].
Total thyroidectomy is the primary treatment for thyroid cancer, with postoperative hypocalcemia being one of its most common complications, occurring in up to 50% of cases. This complication results from direct trauma, devascularization, or unintentional removal of the parathyroid glands during surgery, leading to transient or permanent hypoparathyroidism [3].
The diagnosis of hypocalcemia is made with serum calcium values associated with clinical symptoms in up to 30% of cases. Typically, this pathological condition presents acutely after hospital discharge in emergency departments. Consequently, strategies have been developed for early, even subclinical, diagnosis, including measurement of total calcium, ionized calcium, and parathyroid hormone (PTH) levels [4].
Serum levels of PTH are regulated by a negative feedback loop. PTH is secreted by the parathyroid glands as serum calcium levels decrease, prompting bones to release more ionized calcium and stimulating the kidney and intestines to reabsorb it [5]. The release of PTH is reduced as serum calcium levels increase. The literature suggests that measuring PTH in the immediate postoperative period can predict hypocalcemia and guide calcium supplementation, potentially reducing hospital stays and complications [6,7].
The aim of this study is to analyze PTH levels as predictors of hypocalcemia in patients undergoing total thyroidectomy for thyroid cancer at a tertiary hospital in Ecuador, within a cohort studied from 2016 to 2019. Unlike previous studies that focused on early postoperative PTH measurements (two, four, or six hours), our study evaluates the utility of PTH levels at 24 hours post-surgery, as a predictor of hypocalcemia, which aligns with institutional protocols and allows for a more practical decision-making approach in resource-limited settings [8].
Materials and methods
Study design and population
We conducted a cross-sectional study to evaluate PTH levels as a predictor of hypocalcemia in patients undergoing total thyroidectomy for thyroid cancer at a tertiary hospital in Ecuador. The study spanned from 01 September 2016 to 31 July 2019. This time frame refers to data collection rather than patient follow-up, making a cross-sectional design more appropriate than a retrospective cohort study.
Inclusion and exclusion criteria
Patients diagnosed with thyroid cancer undergoing total thyroidectomy were included in the study. Eligible participants were adults aged 18-80 years, of both sexes. To ensure a representative sample, age groups were categorized as young adults (18-40 years), middle-aged (41-60 years), and elderly (61-80 years). Patients with preoperative hypocalcemia or hypoparathyroidism, individuals with chronic kidney disease or other metabolic disorders affecting calcium homeostasis, and cases with incomplete medical records were excluded from the study. The selection criteria ensured that the study population was homogeneous and that factors influencing calcium metabolism were controlled.
Sample size
A total of 148 patients met the predefined selection criteria and were included in the study.
Ethical approval
This study was approved by the Institutional Ethics Committee (IEC) of Sociedad de Lucha contra el Cáncer (SOLCA), Núcleo de Quito under approval number MSP-VGVS-2021-0193-0, approved on 21 May 2021, Additionally, approval was reaffirmed by Oficio N°073-2022 CEISH Quito, issued on 21 September 2022. Ethical approval was obtained retrospectively for the analysis of pre-existing medical records, following institutional and international guidelines for cross-sectional studies.
Data collection and statistical analysis
Descriptive statistics were presented as frequencies and percentages. Univariate analysis included measures of central tendency and dispersion for quantitative variables. Bivariate analysis was performed using the Chi-square test (χ²), with statistical significance set at p < 0.05. Receiver Operating Characteristic (ROC) curve analysis was employed to determine the diagnostic accuracy of PTH for predicting hypocalcemia. Statistical analysis was conducted using IBM SPSS Statistics for Windows, Version 23 (Released 2015; IBM Corp., Armonk, NY, USA). The ROC curve was used to evaluate the predictive value of PTH levels in identifying postoperative hypocalcemia risk.
Results
During the study period from 2016 to 2019, a total of 32,501 patients underwent thyroidectomy. Among them, 148 patients met the predefined selection criteria and were included in the study (Table 1).
In the fine-needle aspiration biopsy (FNAB) results, classified according to the Bethesda system, category V (Suspicious for Malignancy; n = 84, or 56.8%) and category VI (Malignant; n = 45, or 30.4%) were predominant. Total thyroidectomy was the standard surgical treatment for all patients, with central neck dissection performed in 43.9% of cases. Histopathological examination revealed papillary thyroid carcinoma in 64.9% of cases and follicular carcinoma in 35.1%.
Postoperatively, the mean PTH level at 24 hours was 28.9 pg/mL (SD: 30.8 pg/mL), while the mean serum calcium level was 8.31 mg/dL (SD: 0.74). Using a cutoff value of 10 pg/mL for PTH, hypoparathyroidism was diagnosed in 47 patients (31.8%). Hypocalcemia, defined by a serum calcium level below 7.5 mg/dL, was identified in 18 patients (12.2%). Clinical symptoms of hypocalcemia were evident in 12 patients (8.1%), all of whom received oral calcium and calcitriol.
PTH as a predictor of postoperative hypocalcemia
Table 2 shows that, among patients with hypoparathyroidism, 25.5% experienced hypocalcemia, while 74.5% had normal serum calcium levels. The likelihood of developing hypocalcemia was found to be five times higher in patients with hypoparathyroidism (OR: 5.43; 95% CI: 1.89-15.6), reaching statistical significance (p < 0.05).
Table 2: Parathyroid hormone as predictor of hypocalcemia in patients post-total thyroidectomyStatistical test used: Chi-square test (χ²); p < 0.05 considered significant
Building upon the data from Table 2, we computed parameters to evaluate the efficacy of PTH in predicting immediate postoperative hypocalcemia. Our analysis revealed a sensitivity of 66.7% (95% CI: 41.2-85.6) for this parameter. However, this value falls short of the threshold required for diagnostic testing, which necessitates a sensitivity of 95% or higher.
In terms of specificity, it was determined to be 73.1% (95% CI: 64.5-80.3). This parameter assesses the test's accuracy in correctly identifying patients without the condition. While the specificity value falls short of the ideal, it surpasses the sensitivity, suggesting that PTH determination may be somewhat more effective in ruling out postoperative hypocalcemia.
The positive predictive value (PPV), indicating the likelihood of hypocalcemia in patients with hypoparathyroidism, stood at 25.5% (95% CI: 14.4-40.6). This reinforces the earlier observation regarding sensitivity, particularly in cases where PTH levels are below 10 pg/mL.
Conversely, the negative predictive value (NPV), reflecting the probability of hypocalcemia absence in patients without hypoparathyroidism, reached 94.6% (95% CI: 87.0-97.6). This underscores the test's utility in excluding hypocalcemia.
The positive likelihood ratio (LR+) was calculated at 2.48 (95% CI: 1.61-3.82), while the negative likelihood ratio (LR-) was 0.46 (95% CI: 0.24-0.88). These values indicate the likelihood of hypoparathyroidism in patients with hypocalcemia (LR+) and the likelihood of normal PTH levels in patients without hypocalcemia. Overall, these results suggest that the test's performance in predicting post-total thyroidectomy hypocalcemia is modest (Table 3).
To further assess the predictive value of PTH levels in detecting postoperative hypocalcemia, we performed an ROC curve analysis (Figure 1). The ROC curve illustrates the relationship between sensitivity and 1-specificity, with an area under the curve (AUC) of 0.54, indicating a modest predictive ability of PTH levels for hypocalcemia. While a higher AUC value would suggest stronger discrimination between hypocalcemic and normocalcemic patients, the observed value suggests that PTH alone may not be a robust predictor and should be interpreted in conjunction with other clinical parameters. The ROC curve also highlights the trade-off between sensitivity and specificity at various cutoff points, reinforcing the need for further refinement in predictive modeling.
Receiver operating characteristic (ROC) curve
The present study also involved the development of a linear regression model to explore the relationship between PTH values and serum calcium levels 24 hours post-surgery. The model yielded an adjusted coefficient of correlation (adjusted R² = 0.054), indicating that only 5.4% of the variability in serum calcium levels at 24 hours can be attributed to fluctuations in PTH (standard error = 0.72).
Furthermore, Table 4 provides evidence of a statistically significant association between these variables (p = 0.03).
Discussion
The risk of developing hypocalcemia was found to be five times higher among those with hypoparathyroidism compared to those without it (OR: 5.43; 95% CI: 1.89-15.6, p < 0.05). Lončar et al. [9] detected a higher frequency of post-surgery hypocalcemia in patients with low PTH levels, with 15.1% of all included patients experiencing this complication. Similarly, other authors identified a higher incidence of hypocalcemia; out of 310 patients studied, 34% (n = 108) experienced hypocalcemia and required immediate oral calcium treatment post-surgery [10].
PTH has been described in the medical literature as a paraclinical study serving as a predictor of hypocalcemia after thyroidectomies. Hence, its effectiveness as a predictor was determined, reaching moderate sensitivity at 66.7%. However, other researchers, such as Del Rio et al. [11], found 100% sensitivity for a decrease of over 80% in PTH levels during the immediate postoperative period, necessitating early and effective treatment with a 98% reduction. Izquierdo et al. [12] defined optimal PTH cutoff values for predicting hypocalcemia, recommending its use despite its high economic cost. This recommendation was supported by Gutiérrez Fernández et al. [10], who reported 100% sensitivity, without false negatives, for various PTH cutoff values.
Regarding specificity, the reduction in PTH values reached a level of 87% in predicting hypocalcemia, while a reduction of up to 98% showed 98.6% specificity in determining the need for exogenous calcium supplementation. However, our ROC curve analysis revealed that the predictive utility of PTH for postoperative hypocalcemia was "moderate" (AUC = 64.5%; 95% CI: 48.4-80.5). Conversely, Triguero Cabrera et al. [13] found a "high" predictive power of PTH reduction for hypocalcemia.
While previous studies have assessed PTH at two, four, or six hours postoperatively, our study evaluates 24-hour PTH levels as a predictor of hypocalcemia. Literature indicates that a decrease in PTH levels within the first 24 hours, particularly among asymptomatic women, correlates with a sensitivity exceeding 61% in predicting hypocalcemia [14]. Additionally, researchers have found that a reduction of up to 80% in postoperative PTH values can achieve 100% sensitivity for predicting hypocalcemia, supporting the notion that later PTH measurement may enhance diagnostic accuracy [15]. In our institutional setting, PTH testing at 24 hours is the standard protocol, facilitating practical decision-making regarding calcium supplementation.
We conducted a linear regression model to determine the relationship between detected PTH values and serum calcium at 24 hours post-surgery, revealing that only 5.4% of the variance in calcium levels could be attributed to PTH reduction (adjusted R² = 0.054). Nevertheless, there was a statistically significant association between PTH and serum calcium levels in the immediate postoperative period, as demonstrated by analysis of variance (ANOVA) (p = 0.03) and linear regression analysis. These findings were consistent with those of Filho et al. [16], who observed a relationship between low PTH levels and post-thyroidectomy hypocalcemia.
In summary, although PTH shows promise as a predictor of post-thyroidectomy hypocalcemia, its diagnostic accuracy may vary depending on the study population and methodology, additional research is needed to elucidate the optimal cutoff values and timing of PTH measurements for predicting hypocalcemia accurately. Moreover, the inclusion of other factors, such as preoperative vitamin D levels, in future studies may further enhance predictive models for post-thyroidectomy hypocalcemia.
The study has several limitations. The small sample size limits the generalizability of the findings. Since this was a single-center study, the results may not reflect broader population trends. The high cost of PTH testing restricts accessibility in low-resource settings, which could impact the feasibility of routine implementation. Additionally, confounding factors, such as preoperative vitamin D levels, were not analyzed, which might have influenced calcium metabolism and the study outcomes.
Conclusions
Our study demonstrates a statistically significant correlation between PTH levels and postoperative serum calcium levels, albeit with "moderate" predictive power. We found that PTH levels at 24 hours post-surgery averaged 28.9 pg/mL (SD: 30.8 pg/mL), ranging from 0.01 to 235 pg/mL. Similarly, serum calcium levels averaged 8.31 mg/dL (SD: 0.74), with values ranging from 6.5 to 10.6 mg/dL. These findings reinforce the importance of monitoring for hypocalcemia in this patient population, given its frequency.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer incidence and mortality in Quito: information to monitor cancer control policies Colomb Med (Cali) Cueva P Tarupi W Caballero H 053202210.25100/cm.v 53i 1.4929 PMC 965107836415599 · doi ↗ · pubmed ↗
- 2The epidemiological landscape of thyroid cancer worldwide: GLOBOCAN estimates for incidence and mortality rates in 2020 Lancet Diabetes Endocrinol Pizzato M Li M Vignat J Laversanne M Singh D La Vecchia C Vaccarella S 2642721020223527181810.1016/S 2213-8587(22)00035-3 · doi ↗ · pubmed ↗
- 3Differential diagnosis and clinic of hyperparathyroidism Revista Española de Enfermedades Metabólicas Óseas Gilsanz Fernández C 7076182009
- 4Serum parathyroid hormone as predictor of hypocalcemia after thyroidectomy Revista Ecuatoriana de Medicina Eugenio Espejo Alban Tigre JL Montalvo M Zárate S Villarreal A Puente W Muñoz C Sanchez D 5672020 https://www.psiref.com/periodicals/99162072/revista-ecuatoriana-de-medicina-eugenio-espejo
- 5Secretory capacity of the parathyroid glands after total thyroidectomy in normocalcemic subjects J Clin Endocrinol Metab Anastasiou OE Yavropoulou MP Papavramidis TS Tzouvara C Triantafyllopoulou K Papavramidis S Yovos JG 234123469720122251179410.1210/jc.2012-1170 · doi ↗ · pubmed ↗
- 6Parathyroid hormone-related changes of bone structure Physiol Res Kužma M Jackuliak P Killinger Z Payer J 070202110.33549/physiolres.934779 PMC 888437934918524 · doi ↗ · pubmed ↗
- 7Use of the parathyroid hormone assay at H 6 post thyroidectomy: an early predictor of hypocalcemia J Endocrinol Invest Lacroix C Potard G Thuillier P 184520223421637110.1007/s 40618-021-01601-9 · doi ↗ · pubmed ↗
- 8Parathyroid hormone reduction predicts transient hypocalcemia after total thyroidectomy: a single-center prospective study Int J Endocrinol Mo K Shang J Wang K Gu J Wang P Nie X Wang W 7189857202020203280205610.1155/2020/7189857 PMC 7416261 · doi ↗ · pubmed ↗