Quality improvement in neurosurgery: A systematic review
Mohamed M. Madan, Ahmed M. Alshereiqi, Noor M. Abdulla, Maryam Albreiki, Tariq Al-Saadi

TL;DR
This paper reviews quality improvement efforts in neurosurgery, finding that most studies focus on adult spinal cases and common interventions like new protocols and data analysis.
Contribution
The first systematic review of quality improvement in neurosurgery, highlighting gaps in cranial surgery and underused methods.
Findings
Most QI studies focused on adult neurosurgery and spine surgery, with limited attention to cranial-only cases.
Common interventions included new protocols, ERAS, data analysis, and modified checklists.
Few studies evaluated new technologies, prediction models, or staff education effectiveness.
Abstract
Quality improvement (QI) is crucial for advancing patient care and safety in surgical practices. Despite the presence of numerous systematic reviews on various types of surgeries, no current QI systematic review for neurosurgery is available, at least to the best of our knowledge. The present study thus aimed to explore existing QI frameworks, interventions and outcome measures, which are used to enhance patient care and efficiency in neurosurgery. For this purpose, a systematic review was conducted by identifying 75 articles using key words, such as ‘Quality’, ‘Control’, ‘Improvement’, ‘Neurosurgical’ and ‘Neurosurgery’ across various databases, including PubMed, Google Scholar, Scopus, Wiley, ScienceDirect and Microsoft Academic. Each article was assessed based on inclusion and exclusion criteria, without a time limit for selection. The analysis of the 75 publications revealed an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
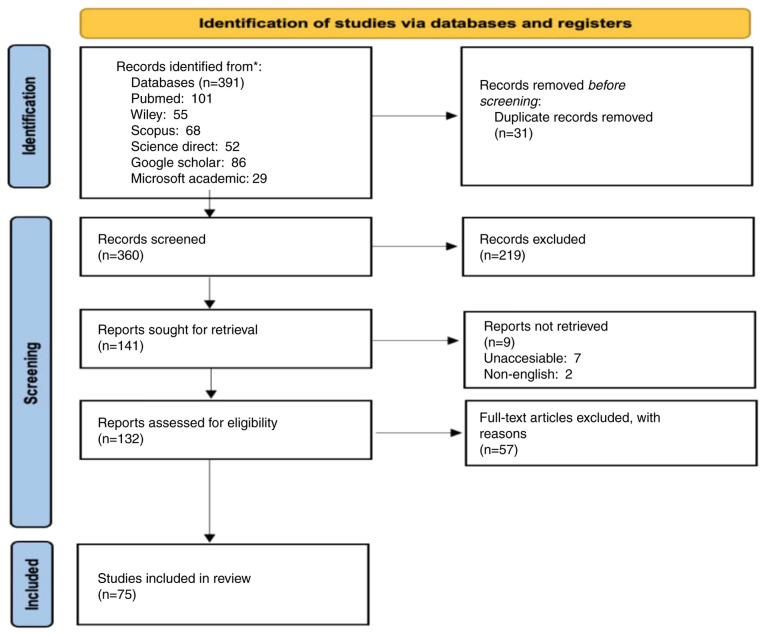 Figure 1
Figure 1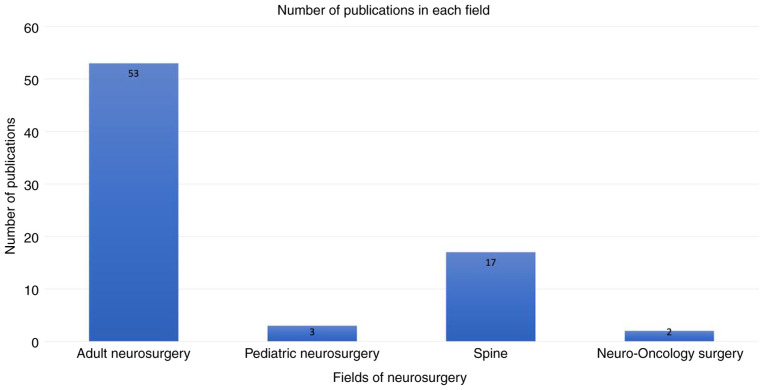 Figure 2
Figure 2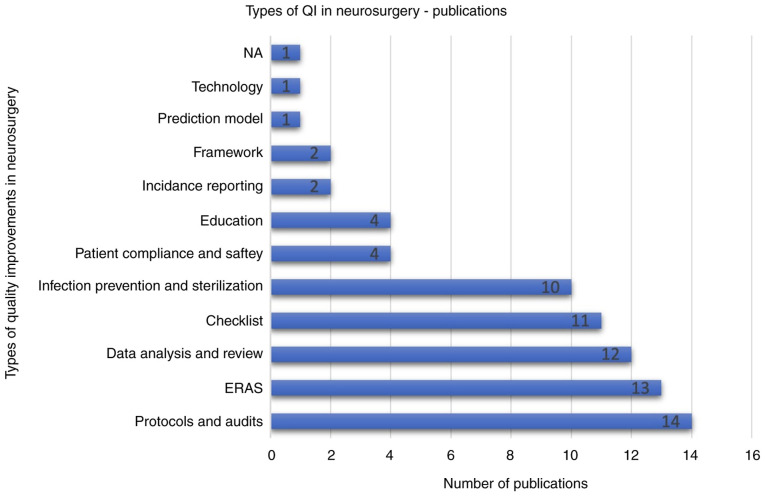 Figure 3
Figure 3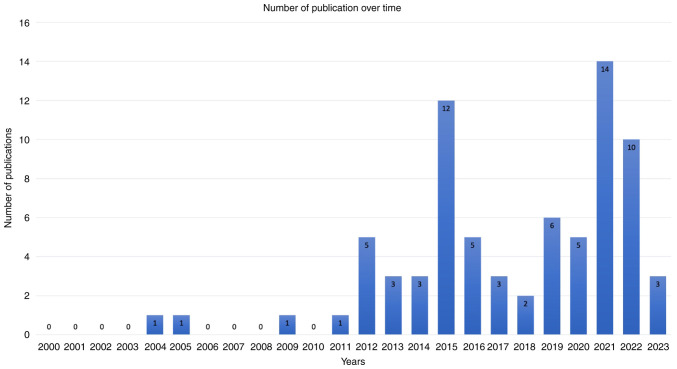 Figure 4
Figure 4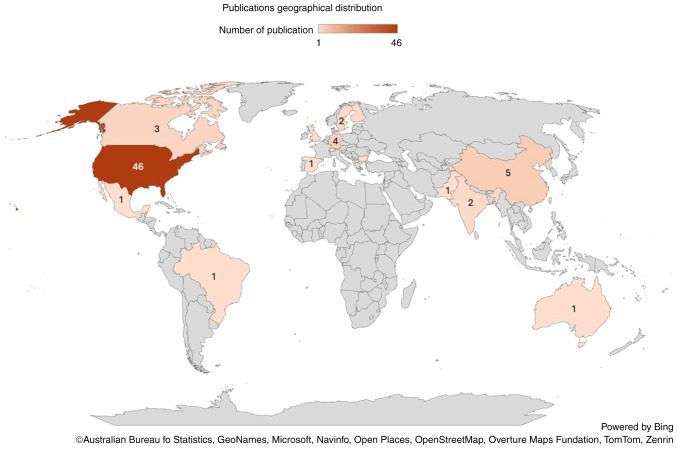 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac, Anesthesia and Surgical Outcomes · Spine and Intervertebral Disc Pathology · Surgical Simulation and Training
Introduction
Quality improvement (QI) is a critical aspect of advancing patient care, enhancing outcomes and ensuring the highest standards of safety and efficiency in surgical practices (1-4). Neurosurgery, with its inherent complexities and high risks, demands attention to detail and a persistent pursuit of excellence. Severe perioperative complications in neurosurgical patients can lead to considerable harm, morbidity, permanent disability, or even mortality. The recovery period following such procedures is frequently complex, requiring extended rehabilitation and the use of expensive specialized resources (2-5). The field has seen notable advancements over the years, driven by innovative surgical techniques, cutting-edge technology and a deeper understanding of neurological conditions (3). However, the complexity and risks associated with neurosurgical procedures require a robust framework for continuous QI. This involves systematically identifying areas for enhancement, implementing evidence-based interventions, and rigorously evaluating outcomes to ensure sustained improvements (5). In this context, QI initiatives aim to reduce complications, optimize patient recovery, and enhance overall surgical success rates, thereby elevating the standard of care for patients (6).
Despite the presence of numerous systematic reviews on various types of surgeries, such as otolaryngology-head and neck surgeries, cleft palate surgeries and laparoscopic surgeries (7-9), current systematic reviews for QI dedicated to neurosurgery have not been established, at least to the best of our knowledge. The present systematic review thus aimed to explore existing evidence, gaps in current practices and standardized QI measures utilized in neurosurgery.
Data and methods
For the present systematic review, articles were selected based on a set of predetermined key words, including ‘Quality’, ‘Control’, ‘Improvement’, ‘Neurosurgical’ and ‘Neurosurgery’. These key words were strategically selected to ensure a comprehensive search and capture all relevant studies within the scope of neurosurgical quality control and improvement. In order to gather the scientific publications, the key words were applied across six major internet search databases: PubMed, Google Scholar, Scopus, Wiley, ScienceDirect and Microsoft Academic. These databases were selected due to their extensive repositories and relevance to the field. Initially, a total of 391 scientific publications were retrieved from these databases. During the initial review, 31 articles were found to be duplicates and were subsequently removed, leaving a total of 360 unique papers for further screening (Fig. 1). The screening process was meticulous and involved a detailed examination of the relevance of each article to the inclusion and exclusion criteria set by the research team. In order to maintain the meticulousness of the screening process at a high level, all reviews and studies that tended to provide information on new interventions to improve the quality of services in neurosurgery were included; articles that discussed non-neurosurgical interventions and were not related to QI were excluded.
This process narrowed the selection down to 75 publications deemed most pertinent for inclusion in the systematic review. The selected scientific articles were found to fall between 2004 and 2023. Although there was no time frame restriction, there were no further articles located prior to that time frame. This 19-year period provided a comprehensive overview of the developments and trends in neurosurgical quality control and improvement. During the screening stage, only articles written in the English language were considered, resulting in the exclusion of two non-English publications. This decision was made to maintain consistency and ensure that all reviewed articles were accessible to the research team.
Results
The 75 publications (listed in Table I) (2,4,5,10-81) revealed an uneven distribution across four main fields of neurosurgery. Adult neurosurgery encompassed the largest proportion of 70.5%, accounting for 53 articles (2,4,5,13,14,16-23,26-29,31-33,35-40,45,48,50-55,57-65,67-70,72-77). This was followed by spine surgery with 17 articles (22.5%) (10-12,24,30,41-44,46,47,56,71,78-81), pediatric neurosurgery with three articles (4%) (15,25,34) and neuro-oncology exclusive studies with the lowest proportion of 3%, representing two articles (49,66) (Table I and Fig. 2). There was also a marked disparity in the distribution of targeted patients (n=621,293) across the different fields of neurosurgery. QI studies focusing on spinal-only cases comprised the vast majority of patients at 87.07% (n=540,955) (10-12,24,30,41-44,46,47,56,71,78-81), while cranial-only studies and combined cranial and spinal studies accounted for 0.21% of the total patients collectively (n=1,309) (2,4,5,13,14,16-23,26-29,31-33,35-40,45,48,50-55,57-65,67-70,72-77). Additionally, the unspecified category accounted for 12.72% (73,29) of patients (15,25,34,49,66) (Table II).
Different interventions were used to improve QI and enhance care in neurosurgery. Implementing new protocols and audits was the most common intervention with 14 articles (18.67%) (12,16,23,33,36,40,61,63,70,72-74,76,81). This was followed by enhanced recovery after surgery (ERAS) with 13 articles (17.33%) (27,39,42,49,57,71,80), data analysis of databases, registries, and literature with 12 articles (16%) (15,18,21,24-26,28,31,34,41,65,66), new or modified checklists implementation with 11 articles (14.67%) (2,19,32,35,37,50-52,54,55,79), and utilizing new sterilization devices or protocols with 10 articles (13.3%) (5,11,17,22,56,58,64,68,69,78). Less frequently addressed interventions were utilizing new technology, using a prediction model, improving incident reporting, increasing patient compliance, and educating the neurosurgical staff (10,13,14,20,29,30,38,53,59,60,75,77) (Fig. 3).
The study design varied within the 75 publications and covered the whole research design pyramid from systematic reviews, the most authentic and strongest research design, to case studies, the least authentic and weakest research design. The predominant design was systematic review studies with 24 articles (32%) (2,11,13,19,22,25,27,33,37,39,42,43,44,46,49,52,54,57-59,65-67,80), followed by randomized clinical trials with 11 articles (14.67%) (5,12,14,23,32,34,35,38,45,47,48), and prospective cohort studies with 10 articles (13.33%) (18,20,21,24,26,30,31,41,53,62). The least research designs used were prospective case-control studies with only one article (1.33%) (77), case reports with two articles (2.67%) (28,37), and correlation (10,29,36) and retrospective (40,64,71) studies with three articles (4%) each. Other types of studies, such as audit studies (4,16,17,61,63,73,74) and cross-sectional studies (15,50,51,56,60) were in between (Table III).
The articles spanned through a period of 20 years from 2004 to 2023, with gaps of no publications in 2006-2008 and 2010. Notably, 81% of the publications were from 2012 to 2023 (2,4,5,10-23,25-59,61-66,68,81). The year 2021 had the highest number of publications with 14 articles (18.66%) (4,16,20,22,27,29,38,42,45-47,50,75,80), followed by 2015 with 12 articles (16%) (5,10,13,18,21,26,31,37,54,56,66,70), and 2022 with 10 articles (13.3%) (15,17,39,40,48,49,58,61-63). Conversely, 2004, 2005, 2009 and 2011 had the fewest publications, with only one article each (24,60,67,77), followed by 2018 with two articles each (14,71). The average number of articles per year between 2004 and 2023 was 3.75 (Fig. 4). Geographically, the distribution of publications was also uneven. The majority originated from the USA (46 articles) (4,5,10,11,13-15,18-31,33,34,38,40,41,43,47,49,53,56,61-63,65,66,68-73,75,76,78,81), and Germany and China with four and five articles, respectively (35,39,48,58,59,64,74,77,79). Contributions from other countries were fewer (Fig. 5).
Discussion
QI in healthcare is crucial for various reasons: For enhancing the outcomes of patients, professional development, understanding healthcare challenges at local and national levels, and improving overall system performance. Given the inherent complexities and critical nature of neurosurgery, QI is exceptionally essential, rendering research in this area fundamental (26).
The results of the present study provide key insight into the QI initiatives within the field of neurosurgery. There is an uneven distribution of publications across the main subspecialties of neurosurgery: Adults, pediatrics, spine, cranial and neuro-oncology. This is similar to the findings of other studies and is due to the higher volume of procedures in one field more than the other and/or higher incidence of complications. The findings of the present study, similar to those of other research, also demonstrated a marked disparity in the distribution of targeted patients across the different fields of neurosurgery being more focused on spinal-only (82). The reason for this may be due to low morbidity rates and high efficacy in sustaining therapeutic outcomes of spinal surgery. As a result, this leads to an unintentional bias in the effort of QI research aimed to improve these outcomes and reduce post-operative complications (82). However, the limited attention given to other subspecialties, such as cranial procedures, is concerning. This imbalance is troubling as it may lead to disparities in the quality of care and patient outcomes across different neurosurgical fields. Future QI initiatives should aim to achieve a more equitable distribution of focus across all subspecialties to ensure comprehensive improvements in neurosurgical care (83).
The most common QI interventions are implementing new protocols, audits, ERAS, and data analysis from databases and registries. As was expected, it was found that these QI interventions reflected marked effectiveness in reducing operative complications and improving outcomes (84). However, other implementations may have a crucial impact on neurosurgical care and outcomes that have less QI research focus. For example, improving incident reporting, prediction models and new technologies. It may be beneficial for future studies to explore the impact of the less common interventions and to determine their impact across neurosurgical settings (6).
The findings presented herein highlight several key areas for future research and development in QI for neurosurgery specifically and healthcare in general. There is a need for more balanced attention across all neurosurgical fields particularly in areas, such as pediatrics and neuro-oncology. Expanding the diversity in QI interventions and exploring the efficacy of less common approaches will be crucial for developing comprehensive strategies, techniques and protocols that address the challenges of neurosurgical care.
The present study had some limitations, which should be mentioned. One of the notable limitations encountered during the study was the inability to access several articles due to paywalls. Despite efforts to obtain these publications, seven articles could not be accessed and were therefore excluded from the review. This limitation highlights a common challenge in academic research where financial barriers restrict access to potentially valuable information. Additionally, the scarcity of articles directly addressing the specific aims of this study posed another limitation. The targeted nature of the key words and the niche focus on neurosurgical quality control and improvement meant that there were relatively few articles available that fit the criteria precisely. As a result, it is possible that some relevant articles were not detected during the search process, potentially leading to an incomplete collection of data. This limitation underscores the importance of continued research and publication in this specialized area to build a more robust body of literature for future reviews.
In conclusion, QI studies enhanced care delivery for patients admitted to neurosurgery departments. The findings of the present study demonstrated that these studies were mainly focused on adult neurosurgery and primarily targeted patients who required spinal surgery. Furthermore, the most commonly employed methods to improve the quality of care include the implementation of new protocols, ERAS pathways, data analysis and new or modified checklists. Further research is required to bridge the gap by addressing QI initiatives in cranial surgery and evaluating the effectiveness of less-used modalities, such as new technologies and predictive models.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Backhouse A Ogunlayi F Quality improvement into practice BMJ 368m 865202010.1136/bmj.m 86532234777 PMC 7190269 · doi ↗ · pubmed ↗
- 2Westman M Takala R Rahi M Ikonen TS The need for surgical safety checklists in neurosurgery now and in the future-A systematic review World Neurosurg 134614628.e 3202010.1016/j.wneu.2019.09.14031589982 · doi ↗ · pubmed ↗
- 3Shirley E Advancements in neurosurgery and exploring innovations techniques Perspective 144512024
- 4Neal MT Richards AE Curley KL Lyons MK Launching a quality improvement project in neurosurgery: How to get started Interdiscip Neurosurg 251012062021
- 5Witiw CD Nathan V Bernstein M Economics, innovation, and quality improvement in neurosurgery Neurosurg Clin N Am 26197205201510.1016/j.nec.2014.11.00325771275 · doi ↗ · pubmed ↗
- 6Hughes RG Tools and strategies for quality improvement and patient safety. Patient Safety and Quality, 2008.21328781 · pubmed ↗
- 7Gettelfinger JD Paulk PB Schmalbach CE Patient safety and quality improvement in otolaryngology-head and neck surgery: A systematic review Laryngoscope 1313340202110.1002/lary.2853832057101 · doi ↗ · pubmed ↗
- 8Grue B Mc Guire C Hong P Bezuhly M Patient safety and quality improvement Initiatives in cleft lip and palate Surgery: A systematic review J Craniofac Surg 34979986202310.1097/SCS.000000000000909436730883 · doi ↗ · pubmed ↗