The incidence and outcomes of traumatic cauda equina syndrome in Victoria, Australia
Xenia Zubenko, Susan Liew, Sandra Reeder, Yi Yang, Ali Humadi, Belinda Gabbe

TL;DR
This study examines the incidence and long-term effects of traumatic cauda equina syndrome in Victoria, Australia, finding that most patients experience lasting health issues.
Contribution
The study provides the first detailed analysis of traumatic CES incidence and outcomes in Victoria using a registry-based cohort.
Findings
The incidence rate of traumatic CES ranged from 0.56 to 2.51 per million per year.
Most patients reported ongoing health issues on the EQ-5D scale at all follow-up time points.
47% of participants had not returned to work 24 months after injury.
Abstract
Little is known about the incidence, management or long-term outcomes of traumatic cauda equina syndrome (CES), with few cohort studies. The purpose of this study is to establish the incidence and long-term outcomes of traumatic CES in Victoria, Australia. This study is a registry-based cohort study, and people with a diagnosis of traumatic CES from 2010 to 2022 were recruited from the Victorian State Trauma Registry. An incidence rate was calculated by dividing the amount of new cases each year by the estimated population in Victoria. Demographic, injury and hospital admission details were extracted from the Victorian State Trauma Registry. Routine follow-up occurred at 6, 12- and 24- months postinjury, with a focus on health-related quality of life outcomes using the EuroQol EQ-5D scale, level of disability using the World Health Organization Disability Assessment Schedule (WHODAS)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
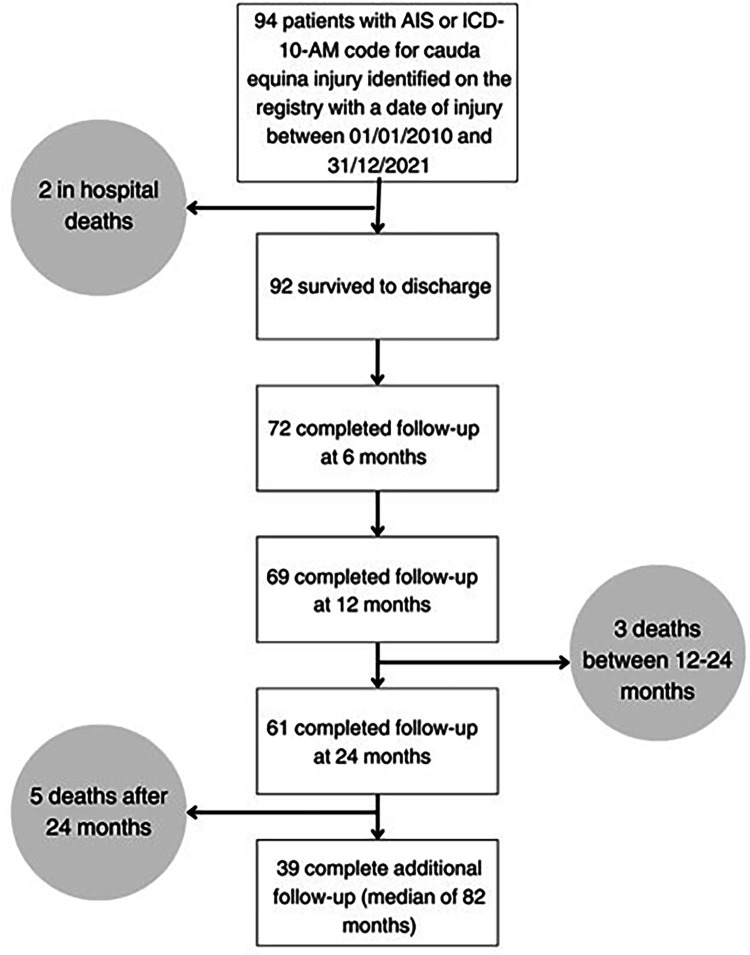 Figure 1
Figure 1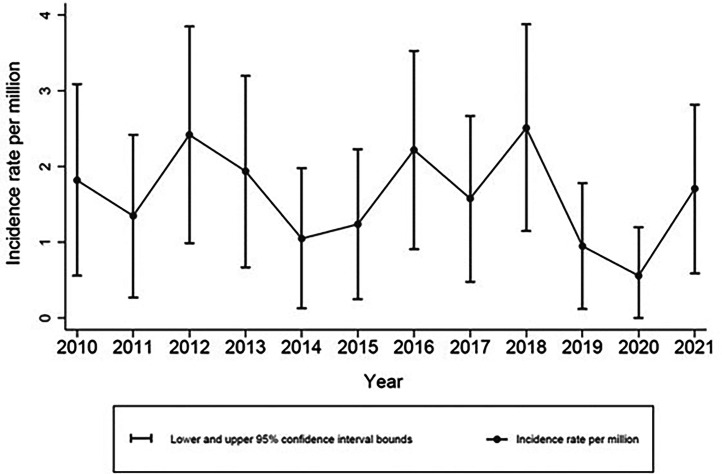 Figure 2
Figure 2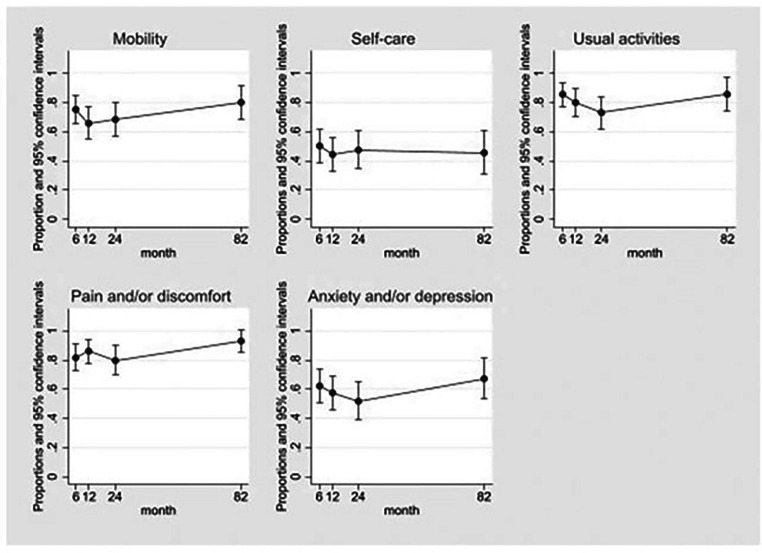 Figure 3
Figure 3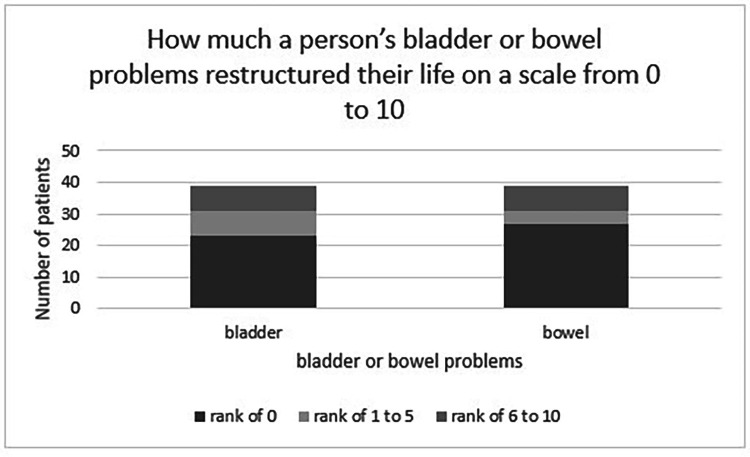 Figure 4
Figure 4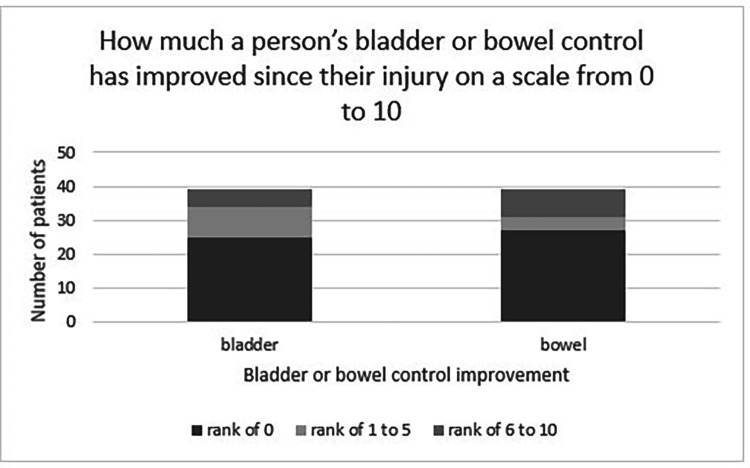 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPelvic and Acetabular Injuries · Spine and Intervertebral Disc Pathology · Spinal Fractures and Fixation Techniques
Introduction
The cauda equina is the continuation of the spinal nerve roots after the spinal cord terminates at the L1-2 vertebral level, innervating the pelvis, perineum, lower limbs, bowel, bladder and reproductive organs.1^,^2 Cauda Equina Syndrome (CES) occurs when the cauda equina spinal nerve roots are compressed or disrupted, causing a constellation of clinical features, such as bowel, bladder and sexual dysfunction, as well as sensory and motor changes. Whilst CES can have a variety of aetiologies, traumatic CES occurs when this syndrome arises after a traumatic injury.3 While the incidence rate of traumatic spinal cord injury in Australia is reported as between 21 and 32 per million per year, the incidence rate of traumatic CES is unknown.4 Traumatic CES has been described in case reports and case series as causing long term neurological sequelae.5^,^6 A few cohort studies exist, with a primary focus on ambulation outcomes following injury to the cauda equina. A retrospective study by Brouwers et al.7 comparing outcomes at varying levels of spinal cord injury had a subgroup of 306 patients with traumatic CES, and described improvement in ambulatory, bowel and bladder outcomes between discharge and at 1 year follow up. Similar improvement in ambulation, bowel and bladder outcomes were demonstrated between admission and hospital discharge by a prospective cohort study by Attabib et al.,8 consisting of 214 patients with traumatic CES. The bowel and bladder outcomes in both papers were reported using the Spinal Cord Independence Measure Score (SCIMS), with Attabib et al. also using the Functional Independence Measure (FIM) Score, which are tools that measure a person's ability to independently manage their bowel or bladder. Neither the FIM score or the SCIMS score directly measure the level of neurological dysfunction, rather reflecting a person's ability to independently manage their symptoms. Furthermore, the SCIMS sphincter subscore reports bladder, bowel and respiratory outcomes as a single outcome, obscuring the nature of recovery of each organ system independently. Overall, the prognosis of bowel and bladder outcomes remain unclear beyond 1 year after injury, with no truly appropriate scoring system being used to capture neurological recovery in this patient population. Despite being a life-long injury, little is known about recovery in the long-term. The aims of this study were to establish the incidence rate of traumatic CES in Victoria, Australia, and to describe the long-term outcomes of this injury.
Methods
Setting
Victoria is the second most populous state in Australia, with a population of 6.8 million.9 The Victorian State Trauma System was established in the year 2000, and includes 138 trauma receiving hospitals, with 3 hospitals considered as major trauma services.10 Ambulance transport and retrieval is provided by Ambulance Victoria, with patients triaged to trauma hospitals according to established guidelines.11 The Victorian State Trauma Registry, established in 2001, is a population-based trauma registry which routinely collects data about all major trauma patients managed in the trauma system.12
Participants and procedures
The study population included people aged 16 years and over with an Abbreviated Injury Scale (AIS), or the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (ICD-10-AM), code for cauda equina injury, and a date of injury from January 2010 to December 2021 (inclusive) (Table 1). To assign an AIS code for CES, the treating team must diagnose the patient with CES, alongside surgical, radiographic or autopsy evidence.13 The ICD-10-AM code is assigned by health coders, based on the diagnosis established by the treating team from the patient clinical health records.14 Whilst no set criteria is used in the Victorian setting to diagnose CES, it is often diagnosed based on a constellation of clinical features including bowel, bladder, sexual, sensory and motor changes presenting in the setting of possible spinal injury and supporting radiographic evidence.3 Ethics approval for this project was granted both by the Alfred Hospital Human Research Ethics Committee (project number 165/23) and Monash University Human Research Ethics Committee (project number 37956).Table 1AIS and ICD-10-AM injury codes.Table 1:AIS Cauda equina injury codes630600.3Cauda equina contusion, NFS.630602.3Cauda equina contusion with transient neurological signs but NFS as to fracture/dislocation.630604.3Cauda equina contusion with transient neurological signs with no fracture/dislocation.630606.3Cauda equina contusion with transient neurological signs with fracture.630608.3Cauda equina contusion with transient neurological signs with dislocation.630610.3Cauda equina contusion with transient neurological signs with fracture and dislocation.631620.3Incomplete cauda equina syndrome but NFS as to fracture/dislocation.630622.3Incomplete cauda equina syndrome with no fracture or dislocation.630624.3Incomplete cauda equina syndrome with fracture.630626.3Incomplete cauda equina syndrome with dislocation.630628.3Incomplete cauda equina syndrome with fracture and dislocation.630630.4Complete cauda equina syndrome but NFS as to fracture/dislocation.630632.4Complete cauda equina syndrome with no fracture/dislocation.630634.4Complete cauda equina syndrome with fracture.630636.4Complete cauda equina syndrome with dislocation.630638.4Complete cauda equina syndrome with fracture and dislocation.ICD-10-AM Cauda equina injury codesS34.3Injury of cauda equina.AIS, Abbreviated Injury Score; ICD-10-AM, International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification; NFS, not further specified.
Demographic characteristics, injury event details, hospital stay variables and patient-reported outcomes were extracted from the registry. Participants’ residential address postcodes were classified as either metropolitan or regional, as determined by the Accessibility/Remoteness Index of Australia (ARIA), and assigned an Index of Relative Socio-Economic Advantage and Disadvantage (IRSAD), with one reflecting the most disadvantaged areas, and 5 representing the most advantaged areas.15^,^16 The Charlson Comorbidity Index (CCI) assigns a numerical value to a patient's mortality risk, based on whether they have any existing comorbid diseases, with a score of zero indicating no comorbidities, and higher scores equating to a higher risk of dying from their respective comorbidities.17 ICD-10-AM diagnosis codes were mapped to CCI conditions to calculate the CCI. The Injury Severity Score (ISS), ranging from 1 to 75 reflects the severity of a patient's injuries, with a score over 12 considered major trauma.18
Patient reported outcomes are routinely collected via telephone interview by registry staff at 6-, 12- and 24-months post injury. Several attempts are made before participants are considered lost to follow-up. Proxies are used in cases where participants are unable to complete the interview or where it is the participant's preference. Routine linkage with the Victorian Registry of Deaths, Births and Marriages is undertaken to identify postdischarge deaths. At the routine 6-, 12- and 24-months follow-up, the EuroQol 5-level 5-dimension questionnaire (EQ-5D-5L), the World Health Organization Disability Assessment Schedule 2.0 (WHODAS) and return to work outcomes are collected.
The EuroQol EQ-5D-5L is a widely used quality of life measure, which examines the domains of mobility, self-care, usual activities, pain and/or discomfort, and anxiety and/or depression.19 Participants respond as experiencing no, slight, moderate, severe or extreme problems to each domain. The registry used the 3-level version (EQ-5D-3L) prior to July 2018. Therefore, for this study, the 5L was mapped to the 3L version. Responses to each dimension are used to create unique health states. Each unique health state is given a utility score, based on societal values as to which health states are considered worse than others, with Australian specific tariffs applied.20 A negative utility score represents a state worse than death, a score of zero represents a health state equivalent to death and one represents perfect health.21 Return to work or study outcomes are also routinely collected by the registry for people who were previously working or studying prior to their injury. These include whether the person has returned to work/study (yes/no), whether they have returned to the same organizations or workplace (yes/no) and whether they are working in the same role at that organization (yes/no).
The WHODAS is an outcome measure examining 6 disability dimensions, including: cognition, mobility, self-care, social interaction, general life activities and social participation. People are asked to score 12 questions that pertain to the last 30 days. Item scores are summed to provide an overall score between zero and 48. The total WHODAS score was categorised as “<10”, and “10+”, with the latter category representing more severe disability.22
In addition to the existing outcomes data captured by the registry, an additional telephone interview was carried out over May and June 2023 to collect the EQ-5D-5L, and bladder and bowel outcomes. Bladder and bowel outcomes are not routinely collected by the registry at the 6-, 12- and 24-months routine follow-up. People previously lost to follow-up at the 3 previous time points were not contacted. Six contact attempts were allowed before a person was considered lost to follow-up.
An existing Multiple Sclerosis bowel and bladder outcomes tool, developed by the National Multiple Sclerosis Society Consortium of Multiple Sclerosis Centers, was adapted in the absence of a bowel and bladder outcome tool specifically designed for CES.23 People were asked how many times a week they were fecal/urinary incontinent, how many times they almost lost control of bowel or bladder, the number of times they had to alter activities due to bowel or bladder problems, and the number of times they were constipated. People were also asked to rate from a scale of 0 (no restructuring) to 10 (most severe restructuring), how much they had restructured their life due to bowel and bladder symptoms. People were also asked to rate on a scale of 0 (no change) to 10 (all issues resolved) how much their bowel and bladder control has improved since injury.
A form created in REDCap was used to collect the additional telephone interview questionnaire and data by registry staff.24^,^25 Stata Version 17 (StataCorp, College Station, TX) was used for statistical analysis. All analysis was performed in the Monash Secure eResearch Platform (SeRP).
Data analysis
The data were summarized using descriptive statistics. The incidence rate was calculated by dividing the number of new traumatic CES cases each year by the number of people aged 16 years and above who lived in Victoria at the 30th of June for that year, sourcing Victorian population figures from the estimated resident population as calculated by the Australian Bureau of Statistics.26 For each incidence rate, 95% confidence intervals were calculated.
For categorical variables, frequencies and percentages were used. Continuous variables were summarized using the mean and standard deviation (SD) if normally distributed, or median and interquartile range (IQR) otherwise. Mixed effects regression modelling was also used to model EQ- 5D outcomes over time to account for the correlation between multiple responses from the same individual (repeated measures). Predicted proportions and 95% confidence intervals at each time point postinjury were calculated. Due to the relatively small study cohort, multivariable modelling was not done.
Results
Cohort overview
Ninety-four people with traumatic CES were recorded on the Victorian State Trauma Registry in the timeframe; 92 survived to hospital discharge (Fig. 1). Of the 94 people, 67% were male, and the median age was 41 years. The most common causes were road traffic crashes and high falls (>1 m) (Table 2). Concomitant lumbar fracture was more prevalent than sacral fracture, and 61% of patients received spinal decompression surgery during their initial hospital stay. The incidence ranged from 0.56 per million per year to 2.51 per million per year between the years of 2010 and 2021, with the rate of injury staying similar over time (Fig. 2).Fig. 1. Flowchart of patient follow-up.Fig 1:Table 2. Demographics table of N=94 patients.Table 2:VariableN (%)Age category17-39 y46 (49%)40-59 y25 (27%)60+ y23 (24%)SexMale63 (67%)Female31 (33%)Level of education attained*Did not complete high school25 (36%)Advanced diploma18 (26%)Completed high school11 (16%)University16 (23%)Metropolitan or regional area of residence†Metropolitan area63 (70%)Regional area27 (30%)Socioeconomic Status (IRSAD)‡1 (most disadvantaged)10 (11%)217 (19%)317 (19%)424 (27%)5 (least disadvantaged)22 (24%)Charlson Comorbidity Index weight (CCI)062 (66%)121 (22%)>111 (12%)Self-reported disability prior to injury§No62 (81%)Yes15 (19%)Cause of injuryRoad trauma33 (35%)High falls29 (31%)Low falls21 (22%)Other11 (12%)Injury Severity Score > 12No26 (28%)Yes68 (72%)Concomitant sacral fractureNo71 (76%)Yes23 (24%)Concomitant lumbar fractureNo16 (17%)Yes78 (83%)Any spinal decompression surgery during hospital stay║No32 (34%)Yes57 (61%)Length of hospital stay<7 days25 (27%)7-13 days28 (30%)14-20 days15 (16%)21-27 days12 (13%)>27 days14 (15%)Intensive care unit stayNo ICU stay74 (79%)ICU stay20 (21%)Discharge destinationRehabilitation55 (59%)Home27 (29%)Hospital for Convalescence6 (6%)In hospital death2 (2%)Other4 (4%)CCI, Charlson Comorbidity Index; ICU, intensive care unit; IRSAD, Index of Relative Socio-economic Advantage and Disadvantage.⁎n=24 missing.†n=4 missing.‡n=4 missing.§n=17 missing.║n=5 missing.Fig. 2. The incidence rate of traumatic CES in Victoria 2010–2021.Fig 2:
Health status and return to work
Of the survivors, 78% completed follow-up at 6 months, 75% at 12 months, 69% at 24 months and 46% at the additional follow-up (Fig. 1). The additional follow-up took place at a median time of 6.8 years (82 months), with an IQR of 4.8 to 11.1 years.
Within the EQ-5D dimensions, problems with pain and/or discomfort were more prevalent across the time points. Whilst a higher percentage of participants experienced problems at the additional follow-up compared to at 24 months in most dimensions (Table 3), there was no clear evidence of change on the EQ-5D items over time (Fig. 3).Table 3EQ-5D and return to work outcomes at follow-up.Table 3:Follow-up time pointTotal respondents (N)6 moN=7212 moN=6924 moN=58Median of 6.8 yN=39EQ-5D dimensionsMobility No problems17 (24%)25 (36%)20 (34%)8 (21%) Some degree of problems55 (76%)44 (64%)38 (66%)31 (79%)Self-care No problems35 (49%)39 (57%)31 (53%)22 (56%) Some degree of problems37 (51%)30 (43%)27 (47%)17 (44%)Usual activities No problems10 (14%)14 (20%)15 (26%)5 (13%) Some degree of problems62 (86%)55 (80%)43 (74%)34 (87%)Pain and/or discomfort No problems13 (18%)10 (14%)12 (21%)3 (8%) Some degree of problems59 (82%)59 (86%)46 (79%)36 (92%)Anxiety and/or depression* No problems27 (38%)30 (43%)29 (51%)16 (41%) Some degree of problems44 (62%)39 (57%)28 (49%)23 (59%)EQ-5D mean utility scoreUtility score mean0.440.500.52(95% Confidence Interval)(0.35, 0.53)(0.42, 0.59)(0.43, 0.62)Return to work outcomes †Returned to work17 (38%)18 (43%)19 (53%)Did not return to work28 (62%)24 (57%)17 (47%)Missing values:⁎N=1 did not answer the anxiety and/or depression section at 6 months and at 24 months.†In the return to work outcomes, N=27 did not respond at 6 months, N=27 did not respond at 12 months and N=25 did not respond at 24 months.Fig. 3EQ-5D dimensions adjusted predictions mixed effect regression modelling graphs.Fig 3:
The EQ-5D utility score improved over time, suggesting overall health perception improved between 6 and 24 months (Table 3). The percentage of people scoring more than 10 on the WHODAS increased between 6 and 24 months, with 65% at 6 months, 59% at 12 months and 68% at 24 months. Forty-seven people were working for income or studying prior to injury, with return to work rates increasing over time; 47% had not returned to work 24 months postinjury (Table 3).
Bowel and bladder outcomes
At the additional follow-up, patients reported severe bladder continence issues, with 6 people reporting daily loss of bladder control, 9 reporting almost losing control of bladder daily, and 6 reporting having to alter their activities on a daily basis due to bladder problems. Overall, less people experienced residual bowel sphincter problems than with bladder sphincter problems, with 8 patients experiencing persistent bowel incontinence compared to 14 patients experiencing persistent bladder incontinence (Table 4).Table 4. Frequency of bladder and bowel problems experience by patients during the week at a median of 6.8 years postinjury.Table 4:Not at allAt least once per wkBladder outcomesNo. of times lost control of bladder or had an accident N (%)25 (64%)14 (36%)No. of times almost lost control of bladder or had an accident N (%)19 (49%)20 (51%)No. of times altered activities because of bladder problems N (%)32 (82%)7 (18%)Bowel outcomesNo. of times they experienced constipation N (%)23 (59%)16 (41%)No. of times lost control of bowels or had an accident N (%)31 (79%)8 (21%)No. of times almost lost control of bowels or had an accident N (%)27 (69%)12 (31%)No. of times altered activities because of bowel problems N (%)32 (82%)7 (18%)
On a scale from zero to 10, 69% of patients reported their bowel symptoms as impacting their life as zero compared to 59% who reported their bladder symptoms as impacting their life as zero (Fig. 4). However, in the group that did report restructuring of their life, there was a higher degree of severity, as 6 people reported 10 out of 10 severity in either bowel or bladder impacts. Most respondents scored their improvement on bladder symptoms (64%) and bowel symptoms (69%) over time as zero (no improvement), whereas 3% reported full resolution of bladder symptoms, and 10% of bowel symptoms (Fig. 5).Fig. 4. Bowel and bladder impact on a person's life graph.Fig 4:Fig. 5. Bowel and bladder symptom improvement since injury graph.Fig 5:
Discussion
The study in this article was the first study to examine quality of life, return to work, bowel, and bladder outcomes of traumatic CES over the long-term, and enable the calculation of its incidence. A low incidence rate confirms CES as a rare injury. The epidemiological profile of the people was consistent with major trauma in Victoria and the literature.[5], [6], [7]^,^[27], [28], [29], [30], [31], [32], [33], [34], [35], [36], [37], [38], [39], [40], [41], [42], [43], [44], [45], [46], [47], [48], [49], [50], [51], [52], [53], [54] Despite low energy mechanisms not being extensively reflected in the literature, the study in this article revealed that 22% of people recorded a low fall as the cause of injury.[55], [56], [57] Another key finding was that concomitant lumbar fracture was more prevalent than sacral fracture.
Problems within each of the EQ-5D domains remained prevalent at a median of 6.8 years postinjury. Whilst we observed little evidence of improvement over time within the EQ-5D dimension of self-care, a retrospective study by Brouwers et al.,7 featuring a cohort of traumatic CES patients, described a significant improvement in self-care 1-year post injury using the SCIMS. In our study, 79% reported difficulty with mobility at the additional follow up with no clear improvement over time, which contrasts to retrospective cohort studies by Brouwers et al. and Attabib et al., demonstrating motor function improvement over time between baseline and at 12-months postinjury and hospital discharge respectively.7^,^8
The low number of participants precluded adjustment for confounders and subgroup comparison. It is possible that participants at the additional time point had more severe problems, prompting their participation in additional follow-up. Improvement in utility scores over a 24-month period may indicate people learning to live with their injury despite ongoing problems. While the proportion of patients who had returned to work or study increased at 24 months postinjury, 47% had not returned to work. The return to work outcomes is similar to the prevalence described in a meta-analysis of return to work outcomes following spinal cord injury published in 2022, with a reported prevalence of 45.8%.58
It is clear a certain proportion of people still experienced issues with bowel and bladder at a median follow-up of almost 7 years. Whilst most participants in our study report no improvement in bowel (69%) or bladder (64%) function over time, this contrasts to findings by other studies showing bowel and bladder improvement over time.7^,^8 Direct comparison to these studies is challenging, as the tools used to measure bladder and bowel outcomes focus on management, rather than quantifying sphincter dysfunction. A traumatic CES subgroup from a cohort study by Brouwers et al. used the Spinal Cord Independence Measure Score, and described an improvement in the sphincter and respiratory management subscore at 12-months compared to baseline, which reports bowel, bladder and respiratory management together as a single outcome measure.7 Another traumatic CES cohort study comparing outcomes between admission and hospital discharge by Attabib et al.8 used the Functional Independence Measure score, and showed improvement at discharge in a person's ability to manage their bladder and bowel.
The study in this article is a unique contribution to the literature, in that it is one of very few cohort studies to investigate traumatic cauda equina syndrome as a stand-alone injury. The use of multiple follow-up time points enabled a more comprehensive account of trends in outcomes over a substantial length of time, and a median additional follow-up time close to 7 years is a substantially longer period of follow-up than previous traumatic CES studies to our knowledge. The use of a detailed and specific bowel and bladder questionnaire, whilst not specific to traumatic CES and was adapted from a Multiple Sclerosis tool, enabled an accurate reflection of sphincter challenges experienced by people, which may be understated using other tools in previously published studies. This study is also the first of this size to include overall quality of life measurements and return to work outcomes for this cohort of patients. To our knowledge, this is the first population incidence rate reported of this syndrome due to traumatic cause.
Despite being a small cohort, this study encapsulates the entire adult population with traumatic CES over the years of 2010-2021 in Victoria, Australia. However, the incidence rate may be an underestimate, with potentially missed cases due to the absence of a universal diagnostic criteria for CES where it is at the discretion of the treating team to make a diagnosis, upon which the AIS and ICD-10-AM codes are based.3^,^59 Furthermore, late or missed diagnoses of traumatic CES, of which there a several case reports in the literature, may also not be included in the registry.43^,^44^,^57^,^60 The use of the EQ-5D scale and subsequent ability to generate utility scores provides a standardized method to measure global health outcomes. In regards to data reliability, the registry data has a high level of completeness with an opt-out rate of less than 0.4 percent, with strict validation rules, trained coders and reference manuals. Whilst the bowel and bladder questionnaire were based on a validated tool used to quantify outcomes in patients with Multiple Sclerosis, reliability and validity checks were not done on this tool for this study. A limitation of the study described in this article was the notable loss to follow-up, raising the potential for responder bias in the final interview. Another limitation of this study was that certain outcomes were not explored, such as sexual dysfunction and sensory changes, with these outcomes being reported in the literature.44^,^48^,^53^,^61^,^62
Conclusion
This cohort study showed that the incidence of traumatic CES in Victoria was low, and closely mirrors the broader trauma cohort in Victoria. It was revealed that most people experienced long-term sequelae following their injury. Further multijurisdictional cohort studies and qualitative research may be done to further investigate this injury.
Funding
The Victorian State Trauma Registry (VSTR) is funded by the Department of Health, State Government of Victoria and the Transport Accident Commission. Belinda Gabbe was supported by a 10.13039/501100000925National Health and Medical Research Council of Australia Investigator Grant (ID 2009998).
Declaration of Competing Interests
One or more of the authors declare financial or professional relationships on ICMJE-NASSJ disclosure forms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Berg EJ Ashurst JV.Anatomy, back, cauda equina Stat Pearls [Internet]2024 Stat Pearls Publishing Treasure Island (FL)
- 2Krassioukov A Elliott S.Neural control and physiology of sexual function: effect of spinal cord injury Top Spinal Cord Injury Rehabilit 231201711010.1310/sci 2301-1PMC 534050429339872 · doi ↗ · pubmed ↗
- 3Lavy C Marks P Dangas K Cauda equina syndrome—a practical guide to definition and classification Int Orthopaed 462202216516910.1007/s 00264-021-05273-1PMC 878278334862914 · doi ↗ · pubmed ↗
- 4New PW Baxter D Farry A Estimating the incidence and prevalence of traumatic spinal cord injury in Australia Arch Physical Med Rehabilit 9612015768310.1016/j.apmr.2014.08.01325218255 · doi ↗ · pubmed ↗
- 5Aresti N Murugachandran G Shetty R.Cauda equina syndrome following sacral fractures: a report of three cases. Case reports J Orthopaed Surg 202201225025310.1177/23094990120200022422933690 · doi ↗ · pubmed ↗
- 6Schildhauer TA Chapman JR Mayo KA.Multisegmental open sacral fracture due to impalement: a case report J Orthopaed Trauma 192200513413910.1097/00005131-200502000-0001115677931 · doi ↗ · pubmed ↗
- 7Brouwers E Meent HV Curt A Recovery after traumatic thoracic and lumbar spinal cord injury: the neurological level of injury matters Spinal Cord 58920209809873237194010.1038/s 41393-020-0463-1 · doi ↗ · pubmed ↗
- 8Attabib N Kurban D Cheng CL Factors associated with recovery in motor strength, walking ability, and bowel and bladder function after traumatic cauda equina injury J Neurotrauma 38320213223293290748310.1089/neu.2020.7303 PMC 7826419 · doi ↗ · pubmed ↗