Recurrent uveitic macular edema managed with intravitreal faricimab injection
Negin Yavari, Dalia El Feky, Frances A. Anover, Khiem Nguyen, Azadeh Mobasserian, Quan Dong Nguyen, Christopher Or

TL;DR
A 63-year-old woman with recurring eye swelling due to a rare eye condition was successfully treated with a new drug called faricimab.
Contribution
This case suggests faricimab may be effective for treatment-resistant uveitic macular edema.
Findings
One dose of faricimab led to complete resolution of uveitic macular edema.
The effect was maintained for three months without recurrence.
The drug's dual action on angiopoietin-2 and vascular endothelial growth factor A may explain its success.
Abstract
To present a case of recurrent uveitic macular edema (UME) treated with intravitreal faricimab injection. Single case report from a tertiary referral center. A 63-year-old Caucasian female presenting with recurrent UME due to birdshot chorioretinopathy (BSCR) in both eyes. UME had been treated with multiple agents including intravenous methylprednisone, posterior subtenons and intravitreal triamcinolone acetonide injection, dexamethasone implant, mycophenolate mofetil, and adalimumab with limited improvement and development of intolerance. Moreover, optical coherence tomography also revealed recurrence of UME with subretinal fluid in both eyes. After treatment with one dose of intravitreal faricimab injection, complete resolution of UME was achieved and maintained for three months. The findings of this case hint towards the potential simultaneous effect of angiopoietin-2 blockade…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
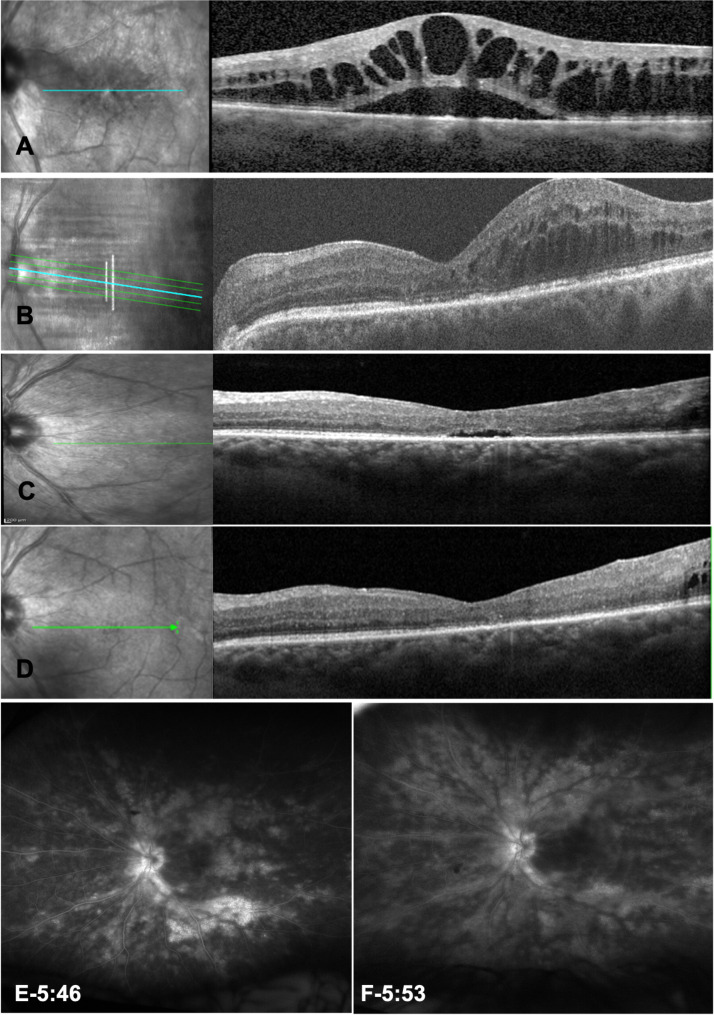 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Diseases and Behçet’s Syndrome · Retinal Diseases and Treatments · Retinal and Optic Conditions
Introduction
Uveitic macular edema (UME) is a frequent complication in uveitis patients and is a leading cause of significant visual impairment. In the Multicenter Uveitis Steroid Treatment (MUST) Trial, macular edema was present at enrollment in 40% of eyes with uveitis with a similar frequency for patients with intermediate uveitis, posterior uveitis, and panuveitis [1–3].
Despite the numerous available drugs for its treatment, at least a third of patients with UME fail to achieve satisfactory improvement in visual acuity [2]. For decades, the first-line treatment of noninfectious uveitis and macular edema have been corticosteroids administered orally, topically, or through either a periocular or intravitreal injection [2, 4]. In the MUST Trial, 62% of eyes with UME treated with systemic medications required regional corticosteroid injections for macular edema [3]. Moreover, it has been shown that intravitreal injection of corticosteroids is superior to other routes of injections [5]. However, risk of developing side effects including cataract, glaucoma, or drug intolerance require the addition of other groups of therapeutic drugs [5–7]. Alternative treatments that could be considered are oral corticosteroids, steroid-sparing immunosuppressives, anti-vascular endothelial growth factor (VEGF) injections, and biologic medications [6]. However, the Macular Edema Ranibizumab versus Intravitreal anti-inflammatory Therapy (MERIT) trial demonstrated that VEGF inhibition with ranibizumab was less effective than the dexamethasone implant in the treatment of UME [8]. Furthermore, many of these medications are used off-label for UME, and there is limited data on their effectiveness in reducing the edema [2, 6].
Faricimab is the first intravitreal therapy designed to simultaneously target VEGF-A and angiopoietin-2 (Ang-2) through a bispecific monoclonal antibody [9, 10]. This approach aims to stabilize retinal blood vessels and inhibit the VEGF drive [9, 10]. Faricimab has recently been approved for the treatment of diabetic macular edema (DME), neovascular age-related macular degeneration (nAMD), and macular edema associated with retinal vein occlusion [11]. However, its use and potential effects on UME are unknown.
We report a case of a patient with birdshot chorioretinopathy (BSCR) with retinal vasculitis, and persistent UME. The patient had multiple intolerances to other therapeutic options. Persistent UME was eventually treated with intravitreal faricimab, resulting in significant improvement in macular edema.
Case presentation
A 63-year-old Caucasian female came to the Uveitis Clinic at a tertiary eye center for the management of BSCR complicated by retinal vasculitis and UME. Other ocular history included laser-assisted in situ keratomileusis and posterior subtenons triamcinolone acetonide (PS-TAAC) injection once in both eyes with incomplete response. Her medical history includes history of pancreatitis. Upon examination, best corrected visual acuity (BCVA) was 20/60 in the right eye (OD) and 20/200 in left eye (OS). Intraocular pressure (IOP) was 13 and 14 in OD and OS, respectively. A full laboratory work was performed; all came back non-revealing except for human leukocyte antigen (HLA)-A29 positivity. Anterior segment examination showed no inflammation in the anterior chamber; however, the vitreous revealed 1 + haze in both eyes. Fundus examination revealed clinically significant macular edema in both eyes. Wide angle fluorescein angiography demonstrated diffuse leakage from macula, optic disc and retinal vessels with peripheral non-perfusion in both eyes. Moreover, optical coherence tomography (OCT) showed disrupted foveal contour with significant UME and subretinal fluid in both eyes.
The patient subsequently received three cycles of monthly intravenous methylprednisone infusions. Despite such treatment, macular and perivascular leakage persisted, leading to the initiation of adalimumab therapy. However, the patient experienced skin reactions at the injection sites and discontinued adalimumab, switching to mycophenolate mofetil 1500 mg twice daily. Since UME remained significant in both eyes, a suprachoroidal injection of TAAC was performed which improved the UME for three months, but the UME recurred (Fig. 1A) despite repeated suprachoroidal TAAC injections [12].
Fig. 1. Posterior imaging of the left eye at presentation and after faricimab injection. A) Optical coherent tomography revealed cystoid macular edema and subretinal fluid at presentation. B) Significant cystoid macular edema prior intravitreal faricimab injection. C) Mild cystoid macular edema one month after intravitreal faricimab injection. D) Resolution of cystoid macular edema three months after intravitreal faricimab injection. E) Diffuse leakage from the optic nerve, peripheral retinal vasculature, and macular edema at presentation. F) Decreased leakage within the macula and optic nerve with persistent leakage from the retinal vasculature after faricimab injection
Given the previous incomplete response to other therapies and patient’s refusal of intravitreal steroids due to potential side effects, an intravitreal faricimab was injected in the OS. After three months of follow up, the injection was well tolerated, and UME showed significant resolution in OCT (Fig. 1B-D) with BCVA of 20/60 in OD and 20/50 in OS, despite continued activity of BSCR demonstrated on fluorescein angiogram (Figure E-F). Within the next six months, UME recurred, and appropriate treatment was administered.
Discussion
Macular edema is the leading cause of vision loss in patients with uveitis [2, 13, 14]. Managing UME when there is no active uveitis presents significant difficulties and often requires exploring new treatment options [13, 14]. In this case, we presented a case of a 63-year-old Caucasian female with BSCR, retinal vasculitis, and UME, who received an intravitreal faricimab injection. Administration of intravitreal faricimab was associated with resolution of recurrent UME after one dose, and by 3 months, the patient maintained the benefit.
To date, there is no widely accepted treatment for managing UME. Traditionally, anti-inflammatory therapy such as corticosteroids is the primary approach for managing UME [14]. Corticosteroids administered orally, intravitreally, or via subtenon injection are used to treat UME due to their potential systemic anti-inflammatory effects, but their long-term use is associated with significant side effects. In cases where oral corticosteroids are not sufficiently effective or produce intolerable side effects, corticosteroid treatments can be delivered through periocular and/or intravitreal methods [13, 14]. Intravitreal corticosteroid injections, such as dexamethasone implants, have shown effectiveness in reducing macular thickness and improving visual acuity in patients with UME. The MERIT trial also demonstrated that dexamethasone implant was significantly better at treating persistent or recurrent UME compared to intravitreal ranibizumab or intravitreal methotrexate [8]. Another option would be the use of suprachoroidal triamcinolone acetonide which also showed improvement in visual acuity and macular edema [12]. Despite various treatment options, there are still patients with recalcitrant disease and recurrent macular edema necessitating repeat therapies and injections [13, 14].
Faricimab, a biphasic antibody targeting both VEGF-A and Ang-2, a novel agent for the treatment of DME, neovascular AMD and retinal vascular diseases, has demonstrated an overall favorable efficacy in randomized controlled trials [9, 10, 15]. No specific anti-VEGF treatment regimen for UME has been proposed in cases where the use of immunosuppressive therapies is limited. The MERIT trial evaluated ranibizumab as a treatment option for UME. Even though it showed efficacy in reducing UME, its efficacy was inferior to that of the dexamethasone implant [8]. By targeting both VEGF-A and Ang-2, faricimab may offer a broader approach to the treatment of retinal diseases, potentially making it more effective than ranibizumab, which only targets VEGF-A [10, 16].
It is well known that a major factor leading to the development of UME is the breakdown of blood-retinal barrier due to chronic inflammation, which involves multiple pathways [14], including inflammation-induced vascular instability, leakage and degradation of tight junction proteins by intracellular phosphorylation, which are partially mediated by VEGF [17]. Ang-2 also contributes to this process by destabilizing vascular endothelium and promoting inflammation [18]. In a study by Oshima et al., Ang-2 was shown to enhance VEGF sensitivity in retinal vessels, leading to extensive neovascularization. They suggested that blocking Ang-2 expression with VEGF blockade could be a potential treatment for retinal neovascularization [19]. Therefore, faricimab, not only inhibit vascular leakage by targeting VEGF-A, but also increases vascular stability by reducing inflammation through Ang-2 blockade [10, 11]. Moreover, the simultaneous inhibition of both VEGF-A and Ang-2 may lead to a potentially longer-lasting effect [20, 21].
Faricimab may be particularly beneficial in specific situations in the management of UME. Patients who require long term local therapy due to either recalcitrant macular edema or intolerance to other forms of therapy may benefit from extended dosing regimen using faricimab. The burden of multiple treatments for UME is multifaceted, involving significant economic costs, clinical challenges, and impacts on patients’ quality of life [2]. The potential extended durability of faricimab, as demonstrated in previous trials for AMD and DME, may be helpful in the management of UME and remains to be investigated [22, 23]. Moreover, faricimab can be considered as a therapy for patients who are at risk of developing steroid-related side effects including glaucoma or cataract [24, 25]. Since it does not cause increased intraocular pressure or accelerate cataract formation, faricimab can also be a better local therapy option for younger patients to avoid long-term complications of corticosteroid use [21]. However, it should be stated that faricimab may only treat the macular edema and the management of the underlying uveitis should still be emphasized.
The limitation of our report is that it is based on a single patient, which limits the generalizability of its findings. Without a comparison to other treatment options, it is difficult to assess the efficacy of faricimab when compared to existing treatments for UME. Therefore, further studies are required to clarify and validate the use of faricimab in the therapeutic regimen for the management of UME.
Conclusion
The index case report demonstrates the potential efficacy of intravitreal faricimab in the management of recalcitrant UME. However, further studies are required to elucidate its role in the management of UME.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lin D et al (2023) Synergistic effect of combined Sub-Tenon triamcinolone and intravitreal Anti-VEGF therapy for uveitic macular edema. Drug Design, Development and Therapy, pp 1055–106610.2147/DDDT.S 353251 PMC 900472935422612 · doi ↗ · pubmed ↗
- 2TENAYA, Investigators L (2024) TENAYA and LUCERNE: Two-Year results from the phase 3 neovascular Age-Related macular degeneration trials of faricimab with Treat-and-Extend dosing in year 2. Ophthalmology 10.1016/j.ophtha.2024.02.01438382813 · doi ↗ · pubmed ↗
- 3Khanani AM et al (2024) TENAYA and LUCERNE: Two-Year results from the phase 3 neovascular Age-Related macular degeneration trials of faricimab with Treat-and-Extend dosing in year 2. Ophthalmology 10.1016/j.ophtha.2024.02.01438382813 · doi ↗ · pubmed ↗