An unanticipated cause of worsening dyspnoea: mitral stenosis induced by cardiac myxoma
Deniz Mutlu, Hakan Yalman, Mehmet Semih Belpınar, Anıl Şahin, Zafer Akman, Davide Margonato

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
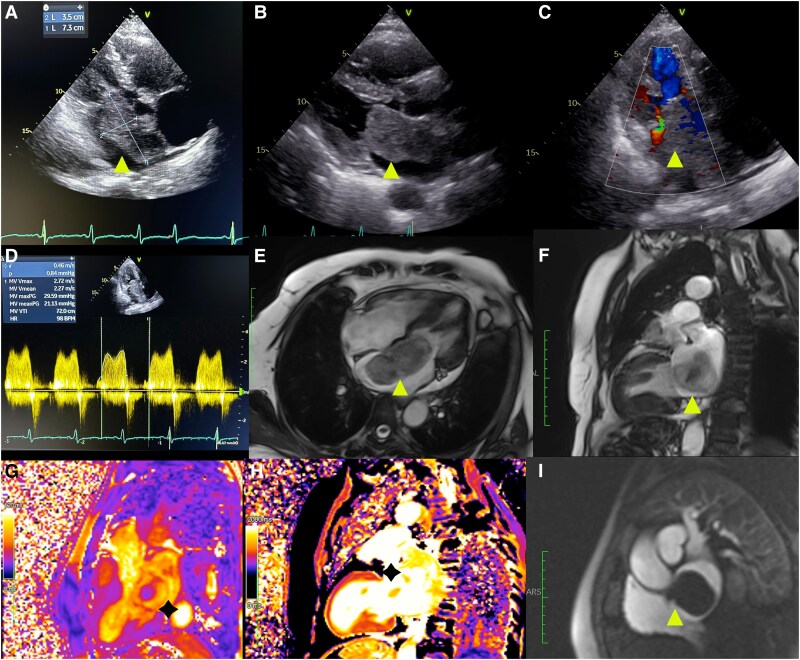 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Metal and Thin Film Mechanics · Cardiac Structural Anomalies and Repair
A 57-year-old female with hypertension presented with worsening dyspnoea, over the last 3 months. Physical examination was notable for crackles on the bilateral lower lung zones and pretibial oedema. Echocardiography demonstrated normal left ventricular function and a hyperechoic polypoid mass measuring 35 × 76 mm attached to the inter-atrial septum (IAS), prolapsing into the left ventricle during diastole and resulting in severe mitral stenosis (Figure 1A–D) and severe pulmonary hypertension (systolic pulmonary arterial pressure: 90 mmHg). Magnetic resonance imaging (MRI) confirmed the presence of a large mass with high signal intensity and heterogenous components attached at the level of fossa ovalis with a thin pedicle, obstructing mitral valve opening; these characteristics were highly suspicious for a diagnosis of cardiac myxoma (Figure 1E and F). The mass was surgically removed by clean dissection along the IAS, and histological examination was consistent with atrial myxoma. Post-operatively, the patient recovered well. On follow-up echocardiography 1-month after the procedure, no residual mass was detected in the left atrium, and patient’s symptoms markedly diminished at 9-month follow-up.
Cardiac myxomas are infrequent, with an incidence of 0.5 per million individuals per year. However, they can result in life-threatening complications such as obstructive symptoms, embolic phenomenon, and constitutional symptoms. Left atrium is the most common location, and it should be differentiated from a thrombus and other masses. MRI has an exceptional tissue characterization capability to determine mass origin and local invasion. Surgical excision is the preferred treatment modality, particularly in cases of symptomatic valve obstruction.