Post-exposure testing at healthcare facilities with SARS-CoV-2 transmission: A rapid review
Emmanuel E. Effa, Okokon Ita, Joshua Mwankon, Funmi Siyanbade, Francis Iwomi, Eleanor Ochodo, Gemma Villanueva, Martin M. Meremikwu

TL;DR
This rapid review found no strong evidence on whether post-exposure testing helps control SARS-CoV-2 spread in healthcare facilities during outbreaks.
Contribution
The study highlights the lack of evidence for testing effectiveness in healthcare settings with ongoing SARS-CoV-2 transmission.
Findings
Pooled prevalence of SARS-CoV-2 among residents was 38% and among exposed healthcare workers was 12%.
Mortality and hospitalization rates were 17% and 24%, respectively, but with very low certainty evidence.
No studies met inclusion criteria for systematic review, only case series were analyzed.
Abstract
Post-exposure severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) testing following health facility outbreaks may control the spread of infection. This study aimed to assess the impact of testing for SARS-CoV-2 infection on health outcomes during healthcare facility outbreaks. This review included studies conducted at skilled nursing facilities, a cancer centre, and a geriatric psychiatric facility. We followed the methods for conducting rapid systematic reviews, searched databases from December 2019 to August 2022, assessed the risk of bias using the modified Newcastle Ottawa scale, and graded the certainty of evidence using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach. We pooled the prevalence, mortality, and hospitalisation results as appropriate. Of the 3055 articles from database search, no study was eligible for inclusion as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
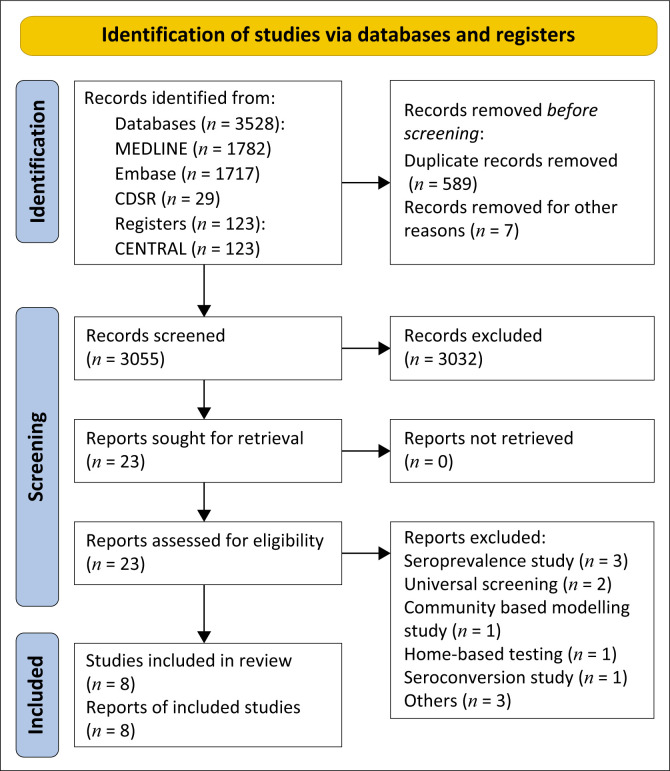 FIGURE 1
FIGURE 1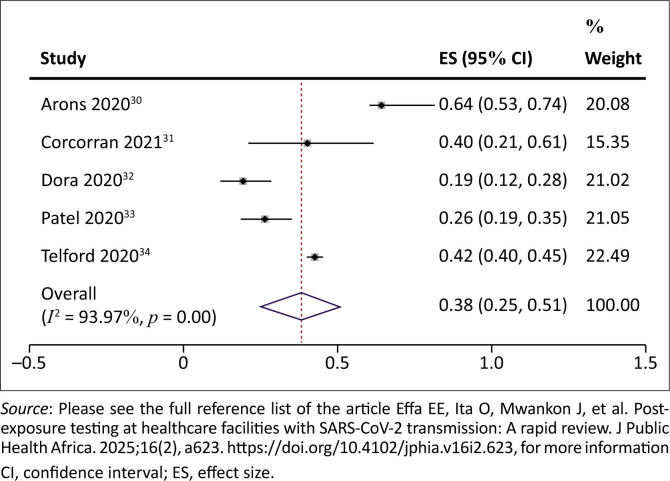 FIGURE 2
FIGURE 2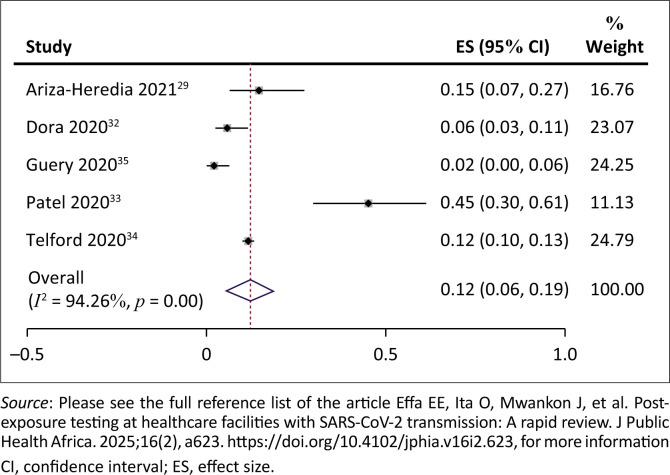 FIGURE 3
FIGURE 3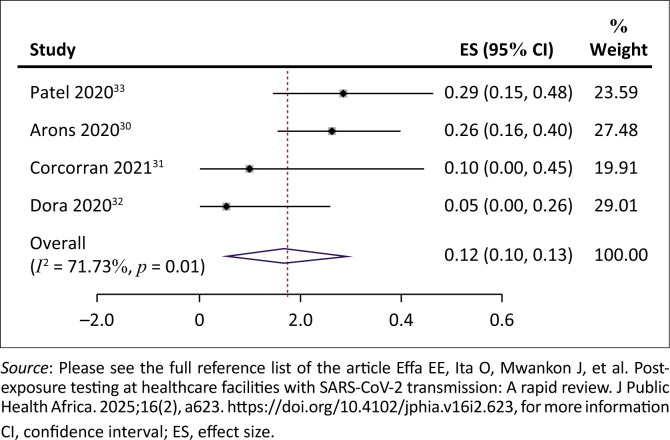 FIGURE 4
FIGURE 4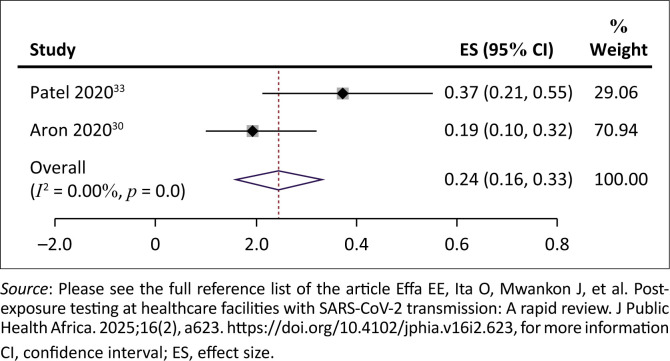 FIGURE 5
FIGURE 5| Study ID | Country | Study period | Setting or facility | Total no. of participants | Methods | Participants | Interventions | Duration of intervention | Outcomes reported | Sample | Notes |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ariza-Heredia 2021 | US | March 2020 – April 2020 | Cancer Centre | 63 | Case series | Healthcare workers | RT-PCR testing | 1 month | Proportion with COVID positive test | Nasopharyngeal sample | Symptomatic HCWs tested |
| Arons 2020 | US | March 2020 | Skilled Nursing Facility | 89 | Case series | Residents | RT-PCR testing and culture | 1 month | Point prevalence, time to onset of symptoms, Doubling time of infections | Nasopharyngeal and oropharyngeal samples | Symptomatic and asymtomatic testing |
| Corcorran 2021 | US | March 2020 – May 2020 | In-patient Geriatric Psychiatric Unit | 81 | Case series | Residents and healthcare workers | RT-PCR testing | 2 months | Prevalence of SARS-CoV-2 infection | Nasopharyngeal sample | 25 patients |
| Dora 2020 | US | March 2020 – April 2020 | Skilled Nursing Facility for Veterans | 232 | Case series | Residents and healthcare workers | RT-PCR testing | 1 month | Point prevalence, oxygen requirement, death, length of hospital stay | Nasopharyngeal sample | 96 residents and 136 HCWs |
| Guery 2020 | France | April 2020 | Medicalised Nursing Home | 136 | Case series | Healthcare workers | RT-PCR testing | 1 month | Point prevalence | Nasopharyngeal | single testing |
| Patel 2020 | US | March 2020 – April 2020 | Skilled Nursing Facility | 126 | Case series | Residents | RT-PCR testing | 1 month | Point prevalence, hospitalisation, death | Nasopharyngeal | single testing |
| Shimizu 2022 | Japan | April 2020 – June 2021 | Nursing Facility | 111 773 | Case series | Residents and HCWs | RT-PCR testing and loop-mediated isothermal amplification (LAMP) assays | 3 months | Incidence rate ratios, hospitalisation, admission days, death | Not indicated | 43 Long-term care facilities |
| Telford 2020 | US | March 2020 – May 2020 | Long-term Care Facilities | 1705 | Case series presented as response and preventive testing groups | Residents and Staff | RT-PCR testing | 4 months | COVID-19 cases, hospitalisations and deaths | Nasopharyngeal | Included LTCFs in which facility-wide COVID-19 testing was initiated before identification of a COVID-19 case. |
| S/N | Study ID | Selection | Ascertainment | Causality | Reporting | Overall risk | |
|---|---|---|---|---|---|---|---|
| - | - | 1. Does the patient(s) represent(s) the whole experience of the investigator (centre) or is the selection method unclear to the extent that other patients with similar presentation may not have been reported? | 2. Was the exposure adequately ascertained? | 3. Was the outcome adequately ascertained? | 4. Was follow-up long enough for outcomes to occur | 5. Is the case(s) described with sufficient details to allow other investigators to replicate the research or to allow practitioners make inferences related to their own practice | Low risk, Medium risk, High risk |
| 1 | Ariza-Heredia 2021 | 1 | 0 | 1 | 1 | 1 | Medium risk |
| Support for judgement | Both symptomatic and asymptomatic HCWs were tested | There was no baseline data reported before the intervention was carried out. | Cases were identified by real-time reverse transcription polymerase chain reaction testing. | 14 days after the last diagnosed case | A cluster of cases was defined as 2 or more cases of SARS-CoV-2– positive COVID-19 among HCWs who work in the same unit area at overlapping times. The identification of cases was carried out by testing symptomatic and asymptomatic HCWs with a reverse transcription polymerase chain reaction (RT-PCR) assay specific for SARS-CoV-2 | ||
| 2 | Arons 2020 | 0 | 1 | 1 | 1 | 1 | Medium risk |
| Support for judgement | Residents in nursing home after an outbreak. Only residents that assented to be tested. Sample size not reported | Tests were done following a confirmed outbreak in the skilled nursing facility. It is unclear how many participants included in the study were exposed. | One-step real-time reverse transcriptase-polymerase chain reaction (rRT-PCR) on all samples and symptom-based checklist. | Follow-up over 3 weeks | The data was obtained from residents that assented Results of positive SARS-CoV-2 tests obtained during postmortem examination or by outside healthcare providers during clinical evaluation of symptomatic residents and staff were provided to the CDC and PHSKC through March 26. | ||
| 3 | Corcorran 2021 | 1 | 1 | 1 | 1 | 1 | Low risk |
| All exposed patients and staff tested following SARS-CoV-2 infection in the facility | Two of the patients with SARS-CoV-2 symptoms were tested positive for the virus. | All samples were analysed using SARS-CoV-2 real-time RT-PCR assay or the Hologic SARS-CoV-2 real-time RT-PCR assay. | Repeat surveillance testing for SARS-CoV-2-positive patients was performed at 3- to 7-day intervals over 8 weeks. | All exposed (symptomatic/asymptomatic) persons tested and retested till negative. | |||
| 4 | Dora 2020 | 1 | 1 | 1 | 1 | 1 | Low risk |
| Support for judgement | All facility patients and staff screened for SARS-CoV-2 following outbreak | Baseline exposure risk screening was done prior to the outbreak. | Nasopharyngeal samples were tested for SARS-CoV-2 by RT-PCR. | Testing was done over 4 weeks (March 29–April 23). Rounds of testing were done. | Reporting disaggregated for patients and health workers | ||
| 5 | Guery 2020 | 1 | 1 | 1 | 1 | 1 | Low risk |
| Support for judgement | All 136 staff members, health workers, and administrative personnel (including auxiliary personnel) were tested. | Testing of staff members prompted following negative SARS-CoV-2 by RT-PCR but positive radiographic features in a patient | Nasopharyngeal RT-PCR tests | Testing was done over 2 days only. | Sufficient description of tested staff (all 136 staff members, health workers, and administrative personnel following a case) | ||
| 6 | Patel 2020 | 1 | 1 | 1 | 1 | 1 | Low risk |
| Support for judgement | SARS-CoV-2 testing was offered to all residents of outbreak Facility A, regardless of symptoms. In addition, testing was offered to 70 staff members who worked on the ward where the index case lived. | Combination of exposure and symptom screening of residents and staff in outbreak facility who specifically worked on the ward with index case | Nasopharyngeal swabs for SARS-CoV-2 via RT-PCR | Residents were followed for 30 days (from 15 March to 14 April 2020) but no planned retesting. | Sufficient description of tested residents and staff including a flow diagram | ||
| 7 | Shimizu 2022 | 0 | 1 | 1 | 1 | 0 | High risk |
| Support for judgement | The targets for screening were determined by the capacity of the testing facility and the expected spread of COVID-19 within the facility based on the epidemiological survey. This may have excluded some potential participants. | Screening tests were done on close contacts within one to 2 days after the confirmation of the first case in a nursing facility. Close contacts were not clearly defined. | PCR universal screening tests were performed at nursing facilities for the HCWs and users if a COVID-19 case was diagnosed within the facility. | Continuous tests were conducted over a period of 1 year. Re-infections were not indicated. | Definitions not consistently defined | ||
| 8 | Telford 2020 | 1 | 1 | 1 | 1 | 1 | Low risk |
| Support for judgement | Testing of residents and staff members at 15 long-term care facilities conducted in response to a confirmed SARS-CoV-2 infection | Testing was carried out 1–5 days after identification of the index case. Residents and staff for testing identified through symptom-based screening. | Samples were tested for SARS-CoV-2 by real-time reverse transcription–polymerase chain reaction (RT-PCR). | A 1-day testing event for consenting residents and staff members was held at each LTCF from March 31–May 18. Symptom-based screening was conducted for 4 weeks thereafter to identify subsequent cases | Test groups are categorised as ‘response group’ and ‘preventive group’. Some were tested by private companies while some included presented evidence of positive results. Unclear what sample and what laboratory. | ||
| Outcomes | Impact | No of participants (observational studies) | Certainty of the evidence (GRADE) |
|---|---|---|---|
| Prevalence of post-exposure SARS-CoV-2 infection among residents/in-patients (SARS-CoV-2 infection) assessed with: RT-PCR | The prevalence of SARS-CoV-2 infection among exposed residents of care homes/patients ranged from 19% to 64%. The pooled prevalence was 38% (95% CI = 25% – 51%; 2044 participants). | 5 | ⨁◯◯◯ |
| Prevalence of post-exposure SARS-CoV-2 infection among healthcare workers (SARS-CoV-2 infection among healthcare workers) assessed with: RT-PCR | The prevalence of SARS-CoV-2 infection among exposed healthcare workers ranged from 2% to 45%. The pooled prevalence of SARS-CoV-2 infection among exposed healthcare workers was 12% (95% CI = 6% – 19%; 2312 participants). | 5 | ⨁◯◯◯ |
| Case-fatality rate (mortality) | The case-fatality rate ranged between 5% and 29%. The pooled case-fatality rate was 17% (95% CI = 5% – 30%) | 4 | ⨁◯◯◯ |
| Hospitalisation | Three studies reported hospitalisation of COVID-19 patients. In Patel 2020, 13 (37%) of 35 SARS-CoV-2-positive cases were hospitalised. In Aron 2020, 11(19%) of 57 SARS-CoV-2-positive cases were hospitalised. The pooled rate of hospitalisation was 24% (95% CI = 16% – 33%; 2 studies, 92 cases) among SARS-CoV-2-positive residents Dora (2020) reported a median length of hospital stay as 6 days (interquartile range 5 days to 10 days). | 3 | ⨁◯◯◯ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and healthcare impacts · COVID-19 and Mental Health · Disaster Response and Management
Background
Coronavirus disease 2019 (COVID-19), an infection with the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus, has strained public health systems and healthcare facilities since its outbreak in December 2019. Globally, there have been approximately 600 million confirmed cases and 6.5 million deaths to date.^1^ Most of these deaths have occurred in the World Health Organization (WHO) regions of North America and Europe with disproportionately lower numbers in some low- and middle-income country regions. Among healthcare workers (HCWs), 152 888 infections and 1413 deaths were reported worldwide in the first year of the pandemic.^2^
Severe acute respiratory syndrome coronavirus 2 virus is spread within healthcare facilities through multiple routes ranging from respiratory droplets, personal items, private and public surfaces, as well as drainage systems.^3^ In addition, there is a higher risk of transmission on non-COVID wards when there is a delay in diagnosis in an exposed person and when HCWs lower their compliance with infection prevention and control (IPC) measures at nursing stations or tea rooms.^4^ Factors that may influence transmissibility following exposure, especially for at-risk individuals, include viral survival, dose-response rate, and the efficiency of spread from hands and surfaces to the respiratory tract. This is further influenced by the emergence of more transmissible variants of the SARS-CoV-2 virus variously described by the WHO as variants of interest (VOI) and variants of concern (VOC).^5^ The main VOC recently have been delta, omicron and omicron sub-variants. Of these, omicron and its sub-variants are reported to be more virulent, are more transmissible (even among the vaccinated), cause more severe disease, are more difficult to diagnose and treat and render public health and available social measures less effective.^5,6^ There are no currently circulating VOI, but previous ones such as epsilon, zeta, eta, theta, iota, kappa lambda and mu have posed increased community transmission risks and threats to global public health.^5^
Outbreaks of SARS-CoV-2 infections in healthcare settings have led to significant mortality among healthcare workers with a global population-based estimate of 115 500 deaths between January 2020 and May 2021,^7^ disruption of services and psychological effects on both patients and HCWs.^8^ Epidemiologic and genomic data suggest a higher likelihood of patient-to-patient transmission compared to staff-to-staff infections and that hospital-acquired infections result in more significant transmissions compared to community-acquired infections.^9^ Residents in long-term care facilities (LTCF) are a particularly vulnerable group to infection with, transmission of and mortality from SARS-CoV-2. In some regions of the world, LTCF residents experienced excess mortality from COVID-19 of between 30% and 40%.^10,11^ The risk of infection, transmission and severe outcomes is related to their older age, presence of chronic comorbidities, poor access to personal protective equipment (PPE), limited testing capacities, atypical symptoms and the recruitment of staff working at multiple facilities with the attendant risk of infection acquisition and spread within the facility.^12^
Public health containment strategies to limit the spread of the virus have included a combination of physical distancing, isolation of symptomatic persons, contact tracing, rapid mass population-based testing and vaccination.^13^ However, owing to the high transmissibility of the virus, especially recent variants in healthcare settings, IPC measures are necessary to prevent patients and HCWs from getting infected. These measures include universal masking for both patients and HCWs, hand hygiene practices, use of appropriate personal protective equipment by HCWs when giving care and screening before admission or procedures.^14^
Mitigation of the spread of SARS-CoV-2 within health facilities depends on the implementation of a combination of several WHO-recommended IPC strategies including: (1) standard, droplet and contact precautions; (2) cleaning and disinfection; (3) testing; and (4) engineering controls. Screening of patients and HCWs within a healthcare facility where there is a high risk of transmission of SARS-CoV-2 involves symptom-based screening and testing for the presence of the virus. However, the variability in the presymptomatic phases (persons who are symptom-free during a positive test but develop symptoms afterwards) and the high percentage of asymptomatic patients (persons with a positive test who never develop symptoms) make the use of symptom-based screening unreliable.^15^ Indeed, up to 30% – 45% of individuals infected with the virus have been reported to be asymptomatic.^16,17^
The detection of SARS-CoV-2 in infected persons is based on several molecular, immunoassay and imaging tests. Molecular tests detect viral ribonucleic acid (RNA) using manual or automated methods such as real-time reverse transcription polymerase chain reaction (rRT-PCR), which is one of several nucleic acid amplification tests (NAAT). Immunoassays are designed to detect viral antigens using immunodiagnostic techniques such as lateral flow assays (LFAs), also called rapid diagnostic tests (RDTs). Immunoassays also detect antibodies in those infected using serological techniques such as LFAs, enzyme-linked immunosorbent assays (ELISAs) or chemiluminescent immunoassays (CLIAs).^18,19^ Imaging tests include computerised tomography scan with specific SARS-CoV-2 abnormalities.^18^ However, the diagnostic accuracies of these tests are variable and depend on a number of factors including whether the exposed person is symptomatic or not.^18^
Prevention and control of outbreaks in healthcare settings rely on testing, which is a critical component of containment strategy for the COVID-19 pandemic. The availability of testing for exposed persons in healthcare settings should lead to quick identification of outbreaks, containment of spread and the proper institution of IPC measures such that vulnerable persons are protected from SARS-CoV-2 infection in the healthcare setting.
The WHO has developed guidance on testing of asymptomatic persons with a history of exposure to SARS-CoV-2-infected persons in various settings.^18,20,21^ In the course of the pandemic, recommendations for and against testing asymptomatic or exposed persons have been debated given the low diagnostic accuracies of available tests in asymptomatic and presymptomatic persons in various settings.^15^ The emergence of several more transmissible variants capable of causing more severe disease even among the vaccinated has led to the modification of rapid tests to improve their sensitivity.^22^ Despite this, the available point of care and RDTs have shown poor performance in detecting the virus in exposed and infected persons.^23^ This has necessitated the assessment of currently available evidence on the diagnostic effectiveness of testing exposed persons using available tests and the impact that may have on the outcomes of persons infected with the virus. Our objective was to assess the impact of testing for SARS-CoV-2 infection in people exposed to the infection in healthcare facilities on health outcomes.
Methods
The protocol for this review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) with the number CRD42022356551. We planned to include the following types of studies: randomised controlled trials, cluster and individual randomised controlled studies. Where RCTs were not found, we planned to include observational studies with a control group such as cohort studies (prospective or retrospective), case-control studies, controlled before-and-after study (CBA), historical control studies and interrupted time series (ITS). Ecological studies, clinical reports, outbreak reports and non-predictive modelling studies were to be excluded. However, in the absence of direct evidence, we have included case series that may provide indirect evidence.
Types of participants
We considered studies that included people in facilities with suspected or confirmed SARS-CoV-2 transmission with a history of exposure to contact with SARS-CoV-2 as follows: residents in long-term care homes, in-patients (hospitals, etc.) including primary care levels, secondary care levels, tertiary care levels, outpatient care facilities, HCWs in long-term care homes, in-patient and out-patient facilities.
Types of interventions
The interventions considered were testing upon exposure using any of the recommended diagnostic molecular or immunoassay (antigen or antibody) tests either as single tests or as a combination of tests such as rRT-PCR, LFAs, serological techniques such as LFAs, ELISAs or chemiluminescent immunoassays (CLIAs). The comparison was no testing upon exposure.
Types of outcome measures
The primary outcome measures were SARS-CoV-2 infection in the facility, the proportion of tested participants with a positive test and all-cause mortality. The secondary outcomes were the proportion of positive participants treated for SARS-CoV-2, time from exposure to testing, participant satisfaction measured using a validated tool, and any adverse events. As this was a diagnostic effectiveness and not diagnostic test accuracy (DTA) review, we aimed to include DTA studies only if they reported qualitative data on the cost and user acceptability of post-exposure testing and planned to extract and present a narrative report of such information.
Search methods for identification of studies
We searched the following databases from December 2019 to August 2022: The Cochrane Library – Central Register of Controlled Trials (CENTRAL) and Cochrane Database of Systematic Review, Medline (PubMed), EMBASE, the Effective Practice and Organisation of Care (EPOC), and LILACS. We also checked the reference lists of retrieved studies for additional reports of relevant studies. There was no language restriction. Full details of the search strategy are shown in Appendix 1. We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline and flow diagram to report the search and selection of studies.^24^
Data collection and analysis
Selection of studies
The results of the search were distributed to four of the co-authors (F.I., O.I., F.S., J.M.) for screening. A more experienced author (E.E.E.) cross-checked a sample (30%) of the excluded studies for accuracy. Full reports of potentially relevant studies were obtained for further assessment. Two authors (F.I. and F.S.) independently applied the inclusion criteria to the full-text reports using an eligibility form and scrutinised publications to ensure each study was included in the review only once. We did not contact the study authors for additional information. We resolved disagreements through consensus agreement with the review team. We listed the excluded studies and the reasons for their exclusion in a table.
Data extraction and management
One author (E.E.E.) independently extracted data using a specifically developed piloted data extraction form. A second author (F.S.) cross-checked the extracted data for accuracy. We extracted where available data related to population, country, setting (residents of long-term homes, hospitals, outpatient, in-patient), age (adults, children), type of sample collected, type of test (rRT-PCR, antigen, antibody), frequency of testing/duration of intervention, outcomes reported, vaccination status, comorbidities, previous infections and variants for all included studies. We resolved disagreements through discussion between all review authors.
For each outcome, we extracted the number of participants exposed and the number tested in each facility.
Assessment of risk of bias in included studies
We had planned to assess the risk of bias of each included study using the appropriate ‘risk of bias’ tool for RCTs and resolve any disagreements by discussion between review authors. However, as we found no included studies as defined in our protocol, we decided to draw some indirect evidence from the case series. As the included studies were mainly case series, we used the modified Newcastle Ottawa scale and its modifications with eight items categorised into four distinct domains as follows: selection, ascertainment, causality and reporting.^25^ We categorised studies as low, medium or high risk of bias. The assessment is summarised in the risk of bias of the included studies table.
Measures of treatment effect
As heterogeneity was expected considering the included study design, variability in the participants and facilities and the lack of a comparator arm, we used an inverse-variance random-effects model to estimate the pooled prevalence, all-cause mortality as well as hospitalisation rates for both residents and HCWs and presented these results as forest plots indicating the effect estimates with their corresponding confidence intervals. We assessed statistical heterogeneity using the I^2^ statistic. We were unable to investigate clinical heterogeneity because of the small number of included studies. We were also unable to explore publication biases by constructing a funnel plot as there were not enough studies contributing to each outcome.
Strategy for data synthesis
We have combined studies in a meta-analysis for prevalence (residents, patients, and HCWs separately), all-cause mortality and hospitalisation rates using a random effect model and generated forest plots using the meta-prop syntax^26^ in STATA version 13.^27^
Assessment of certainty of evidence
We assessed the certainty of the evidence using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach.^28^ We appraised the certainty of the evidence for the important primary outcomes of SARS-CoV-2 infection (here reported as prevalence) and all-cause mortality and a secondary outcome, hospitalisation, derived from the included studies (each outcome against five criteria: risk of bias, consistency, directness, precision and publication bias).
Ethical considerations
This article followed all ethical standards for research without direct contact with human or animal subjects.
Results
The initial search returned 3528 articles and an additional three studies by searching the reference lists of included full-text articles. After removing duplicates, 3055 records were screened for eligibility. Of these, 3032 were excluded. There were no studies that met our inclusion criteria necessitating our consideration of case series to provide supportive information to draw indirect evidence from. Of the remaining 23 articles, 8 were included after reviewing their full texts (Appendix 1). This is shown in the PRISMA flow diagram (Figure 1).
Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram.
Characteristics of included studies
All eight included studies were case series. Six of the included studies were conducted in the United States.^29,30,31,32,33,34^ with a total of 2296 participants. One each was conducted in France^35^ and Japan^36^ and included a total of 136 and 111 773 participants, respectively. All the studies took place between March 2020 and June 2021 with the duration of the studies being between 1 month and 4 months. Full details are in the table of characteristics of included studies (Table 1).
Setting
Most of the studies were conducted in long-term care and skilled nursing facilities. One study took place in a cancer centre,^29^ while another study was in a geriatric psychiatric centre.^31^
Participants
In four of the studies, testing of both residents and HCWs commenced upon identification of a case within the facility,^31,32,34,36^ while in the other four studies, testing targeted either residents or HCWs alone.
Intervention
Reverse transcriptase polymerase chain reaction testing was done for participants in all included studies using mainly nasopharyngeal samples. In addition, cultures were requested in one study,^30^ while loop-mediated isothermal amplification (LAMP) assays were done in another.^36^
In one study,^36^ the sample collected for testing was not indicated. Here, 43 long-term care facilities (LTCF) were included, and screening tests were done within 1–2 days after the confirmation of the first case. In another study^34^ involving participants in LTCFs, facility-wide COVID-19 testing was initiated before identification of a COVID-19 case in some of the facilities designated as ‘the preventive group’. We have only included data from ‘the response group’ where testing took place after an identified positive case. In only one included study was there data at baseline and 4 weeks after initiation of testing.^34^ In all studies, active case finding with testing was combined with transmission-based adjunctive IPC measures such as cohorting, isolation and heightened use of PPEs.
Outcomes
All studies reported at least one of the primary outcomes. The number of participants positive for COVID-19 was reported in variable ways at the start of the screening. Point prevalence was the most often reported measure and was seen in five of the included studies.^30,31,32,33,35^ Two studies reported a proportion of COVID-19 positive,^30,34^ while one study reported incidence rate ratios.^36^ However, no study reported a proportion of COVID-19-positive participants at a specific time point after testing began. Mortality was reported in four studies.^32,33,34,36^ Other outcomes reported included time to onset of symptoms, doubling time of infections, hospitalisation and oxygen requirement.
Risk of bias assessment and certainty of evidence
Five studies were classified as being of low risk of bias,^31,32,33,34,35^ two as medium risk of bias^29,30^ and one as high risk of bias.^36^ In the study with high risk of bias, the targeted participants for screening were determined by the capacity of the testing facility and the expected spread of COVID-19 within the facility based on an epidemiological survey.^36^ This may have excluded some potential participants. The details of the assessment are shown in the risk of bias table (Table 2). As all included studies were case series, the certainty of evidence for all assessed outcomes was rated as very low because of their inherent methodological limitations as shown in the summary of findings table (Table 3).
Primary outcomes
Severe acute respiratory syndrome coronavirus 2 infection in the facility
No studies were identified that evaluated the impact of testing upon exposure to SARS-CoV-2 infection in the facility. However, we identified five studies reporting point prevalence of the infection in the facility. The prevalence of SARS-CoV-2 infection among exposed residents of care homes/patients ranged from 19% to 64%. The pooled prevalence was 38% (95% CI = 25% – 51%; 5 studies, 2044 participants; I^2^ = 94%, very low certainty evidence) (Figure 2). The results were downgraded to low certainty evidence because at least one study^30^ was assessed to be at medium risk of bias; there was significant statistical heterogeneity of 94%, and the studies were all observational as none had a comparison ‘no testing’ arm (Table 3).
Prevalence of severe acute respiratory syndrome coronavirus 2 infection among exposed residents/patients.
The prevalence of SARS-CoV-2 infection among exposed healthcare workers ranged from 2% to 45%. The pooled prevalence of SARS-CoV-2 infection among exposed HCWs was 12% (95% CI = 6% – 19%; 5 studies, 2312 participants; I^2^ = 94%, very low certainty evidence) (Figure 3). The evidence for this was rated as low certainty because at least one study^29^ was assessed to be at medium risk of bias; heterogeneity was significant (94%), and the included studies lacked a comparison ‘no testing’ arm.
Prevalence of severe acute respiratory syndrome coronavirus 2 infection among exposed healthcare workers.
In the only study with data at baseline and 4 weeks after initiation of testing, the prevalence was 28.0% and 42.4%, respectively, for residents and 7.4% and 11.8%, respectively, for healthcare workers.^34^
All-cause mortality
No studies were identified that evaluated the impact of testing upon exposure on all-cause mortality. However, we identified four studies that reported this on mortality rate.^30,31,32,33^ It was unclear if this was SARS-CoV-2-specific mortality or all-cause mortality. The case-fatality rate ranged from 5% to 29%. The pooled case-fatality rate was 17% (95% CI = 5% – 30%; 4 studies; 121 cases; I^2^ = 72%, very low certainty evidence) (Figure 4). The results were downgraded because at least one study^30^ was assessed to be at medium risk of bias, included studies did not have a comparison ‘no testing’ arm, statistical heterogeneity was 72% and sample size of cases was very low (Table 3).
Mortality among severe acute respiratory syndrome coronavirus 2-infected residents/patients.
Secondary outcomes
None of the included studies explicitly reported on any of the secondary outcomes (proportion of positive participants treated for SARS-CoV-2, time from exposure to testing, participant satisfaction and adverse events) indicated in the protocol for this review.
However, three studies reported hospitalisation of SARS-CoV-2-positive residents of long-term care facilities. Hospitalisation was mostly described as admission to a formal hospital for additional care. In one study,^33^ 13 (37%) of 35 SARS-CoV-2-positive cases were hospitalised, while in another study,^30^ 11 (19%) of 57 SARS-CoV-2-positive cases were hospitalised. The pooled rate of hospitalisation was 24% (95% CI = 16% – 33%; I^2^ = 0%, very low certainty evidence) among SARS-CoV-2-positive residents (Figure 5). One study^32^ reported a median length of hospital stay as 6 days (interquartile range 5 days to 10 days). The results were downgraded because at least one study^30^ was assessed to be at medium risk of bias, included studies lacked a comparison ‘no testing’ arm and the sample size of cases was low.
Rate of hospitalisation among severe acute respiratory syndrome coronavirus 2-positive residents.
Discussion
In this rapid review on the effectiveness of deploying a testing strategy following an outbreak of SARS-CoV-2 infection in healthcare facilities to primarily mitigate spread, we found no eligible comparable studies to draw direct evidence from. We included case series in the review to provide indirect evidence to guide decisions. Although many of the included studies were of low risk of bias, they lacked any comparator arms leading to downgrading of the evidence to very low certainty across reported outcomes. Furthermore, all the studies were reported from high-income countries, so we cannot appropriately contextualise the findings. Lastly, most included studies have only provided baseline data which have been reported as prevalence but follow-up data to determine the effectiveness of the testing strategy is lacking.
The dynamics of transmission of SARS-CoV-2 in healthcare facilities has been affected by the emergence of new variants with differing transmissibility and the availability of vaccination.
Newer variants such as omicron and delta apart from being more transmissible are shed for longer periods after symptoms emerge.^37,38^ Indeed, emerging studies report no difference in virus shedding between vaccinated and unvaccinated individuals.^39^ These have implications for the timing of testing and periods of isolation of infected persons and may potentially disrupt service provision in places experiencing limitations in the number of health workers. The included studies were conducted at a time when vaccination was not available. Therefore, it is not possible to determine the relationship of the outcomes with vaccination status.
This review is limited by the inclusion of single-arm case series and the absence of results of testing from baseline and after the beginning of testing as well as the inclusion of data from only skilled nursing facilities where only elderly patients reside. The results cannot be generalised to regular hospitals with varying patient types.
Conclusion
There is no identified direct nor indirect evidence for the effectiveness or not of testing people in healthcare facilities where there is ongoing transmission of SARS-CoV-2 infection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO. Coronavirus (COVID-19) dashboard [homepage on the Internet]. 2022 [cited 2022 Aug 24]. Available from: https://covid 19.who.int/.
- 2Bandyopadhyay S, Baticulon RE, Kadhum M, et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob Health. 2020;5(12):e 003097. 10.1136/bmjgh-2020-003097 PMC 772236133277297 · doi ↗ · pubmed ↗
- 3Feng B, Xu K, Gu S, et al. Multi-route transmission potential of SARS-Co V-2 in healthcare facilities. J Hazard Mater. 2021;402:123771. 10.1016/j.jhazmat.2020.12377133254782 PMC 7446651 · doi ↗ · pubmed ↗
- 4Zabarsky TF, Bhullar D, Silva SY, et al. What are the sources of exposure in healthcare personnel with coronavirus disease 2019 infection?. Am J Infect Control. 2021;49(3):392–395. 10.1016/j.ajic.2020.08.00432795495 PMC 7419261 · doi ↗ · pubmed ↗
- 5WHO. Tracking SARS-Co V-2 variants [homepage on the Internet]. 2021 [cited 2022 Aug 24]. Available from: https://www.who.int/en/activities/tracking-SARS-Co V-2-variants/.
- 6Andrews N, Stowe J, Kirsebom F, et al. COVID-19 vaccine effectiveness against the Omicron (B.1.1.529) variant. N Engl J Med. 2022;386(16):1532–1546. 10.1056/NEJ Moa 211945135249272 PMC 8908811 · doi ↗ · pubmed ↗
- 7WHO. The impact of COVID-19 on health and care workers: A closer look at deaths. Health Workforce Department – Working paper 1 [homepage on the Internet]. Geneva: World Health Organization; 2021 [cited 2022 Aug 27]. Available from: https://apps.who.int/iris/bitstream/handle/10665/345300/WHO-HWF-Working Paper-2021.1-eng.pdf.
- 8Sun P, Wang M, Song T, et al. The psychological impact of COVID-19 pandemic on health care workers: A systematic review and meta-analysis. Front Psychol. 2021;12:626547. 10.3389/fpsyg.2021.62654734305703 PMC 8297953 · doi ↗ · pubmed ↗