Liquid biopsy in head and neck cancer patients: blood, saliva, or both ?
Valentina De Pascale, Federica Ganci, Fabrizio Leone, Valentina Manciocco, Flaminia Campo, Anastasia Mercurio, Alina Catalina Palcau, Claudio Moretti, Frauke Goeman, Sara Donzelli, Giulia Orlandi, Federica Orrù, Renato Covello, Paola Muti, Sabrina Strano, Antonello Vidiri

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
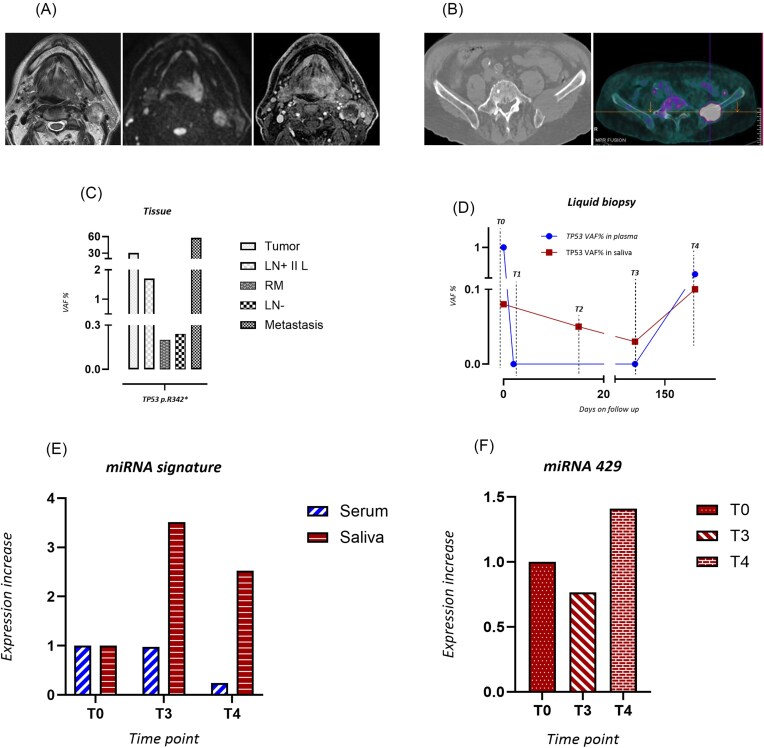 Figure 1
Figure 1- —Ministry of Health10.13039/100009647
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Tumors Diagnosis and Treatment · Head and Neck Cancer Studies · Cancer Genomics and Diagnostics
Dear Editor,
Head and neck squamous cell carcinoma (HNSCC) is the sixth most common cancer worldwide, with a constantly growing incidence. HNSCC comprises a group of heterogeneous tumors that originate from the upper digestive region. Tobacco, alcohol abuse, and human papillomaviruses (HPV) infection are the major etiologic agents for HNSCC. Local relapse and metastasis are major causes of mortality, accounting for 50% of cases. Distant metastasis of head and neck cancers are present in ∼10% of HNSCC patients. Diagnosis of distant metastasis is assoc
iated with unfavourable prognosis, with a median survival of ∼10 months [1]. Despite recent advances, multimodality approaches are still not effective in eradicating HNSCC. Liquid biopsy has recently emerged as a very powerful tool that has re-shaped the management of cancer patients worldwide [2–4]. HNSCC patient-derived nucleic acids can be monitored in biological fluids such as blood and saliva, thus suggesting liquid biopsy–molecular approaches as unique tools to refine diagnostic evaluation and therapy allocation. Through minimally invasive procedures, liquid biopsy allows early diagnosis, detection of minimal residual disease, and real-time monitoring of recurrence, metastases, or therapeutic responses [2, 5]. Indeed, the identification and the tracking over time of tumor aberrations released into the body fluids may enable the discovery of novel, non-invasive prognostic and diagnostic biomarkers that can provide an early prediction of disease progression in a timely and cost-effective fashion [6]. Timely prediction of relapse in HNSCC patients is a major challenge that might improve patient survival unprecedently. Liquid biopsy, being only minimally invasive, could be applied to serially monitor surgically resected HNSCC patients in a timely manner to anticipate either relapse or distant metastasis. Furthermore, in the adjuvant setting for HNSCC patients the use of liquid biopsy to monitor the response to treatment will be a unique non-invasive and safe tool with important implications for patients with poor quality of life.
TP53 mutation is the most frequent genetic alteration (70%–80%) of HPV-negative HNSCC patients. MicroRNAs (miRNAs) are small non-coding and highly stable RNA molecules that are easily detectable in the body fluids of a wide range of cancer patients including those with HNSCC. Precise and serial quantification of circulating analytes in body fluids is a critical step toward clinical application of liquid biopsy in cancer patient management. Digital PCR (dPCR), with its high precision and sensitivity, is the most promising technology for this purpose to accurately detect and quantify rare DNA and RNA sequences in the presence of abundant targets [7].
In the present study we sought to simultaneously profile TP53 mutations and miRNA expression in multiple liquid biopsy samples from one metastatic HNSCC patient, thereby tracing the related molecular evolution over time. A 69-year-old Caucasian male, p16 and HPV negative, heavy smoker (30 cigarettes/day for 35 years), non alcohol user was referred to our Institute for a cancer lesion (pT4aN3bG3) of the oropharynx (left base of tongue) (Fig. 1A). The patient underwent subtotal glossectomy and neck dissection and was subjected to adjuvant radiotherapy and systemic treatment with weekly cisplatin. A metastatic lesion at the skeletal level (left iliac wing) was identified 3 months after the end of treatment (Fig. 1B). Pembrolizumab treatment for the metastatic lesion lasted for 1 month as the patient's health condition rapidly deteriorated leading to death. We aimed create a portrait of the patient molecularly at diagnosis and throughout his clinical evolution. To this end, we collected the following patient tissues and body fluids: (i) tissues from the primary tumor, metastatic lymph node, and metastatic lesion at left iliac wing; (ii) representative lymph nodes and resection margins histologically tumor free; (iii) plasma samples collected at different time points [i.e. the day before and after surgery (T0 and T1), 5 days after the end of adjuvant treatment (T3), and during clinical follow-up (T4)]; and (iv) serum and saliva samples collected at pre-surgery (T0), at 5-days post treatment (T3), and during follow-up (T4). To monitor patient molecular evolution, we initially assessed the mutational profile of the primary tumor by whole-exome sequencing (WES) analysis. Most of the pathology units including that at our institute perform Next Generation Sequencing (NGS) approaches using targeted panels with a wide range of genes. While this approach is certainly easier to apply than WES, it may suffer in providing medical oncologists with a limited knowledge of the tumoral mutational landscape of a given cancer patient. This might have an impact not only on first line therapy, but also with regard to resistance and metastatic dissemination, in which any genetic alterations—even undruggable—need to be considered in the design of a specific therapeutic approach. Whole exome sequencing (WES) is getting very close to clinical application for both turnaround time and costs, thereby guiding the implementation of an increasingly precise oncological treatment. Specifically, among the mutated genes, we observed a TP53 p. R342* mutation (c.1024C > T). Of note, the same TP53 mutation was also detected in histologically tumor-free tissues, metastatic tissue, and in both saliva and plasma by dPCR analysis (Fig. 1C and D). Unexpectedly, all histologically tumor-free tissues (such as resection margins and negative lymph nodes), previously declared histologically negative for tumor cells, exhibited the presence of TP53 p. R342*, with a Variant Allele Frequency (VAF) > 1% (Fig. 1C). These findings might suggest either minimal residual disease that was not macroscopically and microscopically evident or the presence of preneoplastic clones predisposed to evolve into cancer cells upon adjuvant therapy. Interestingly, we detected the TP53 mutation p. R342* in circulating tumor DNA (ctDNA) plasma samples collected before surgery (T0, VAF 1%) and 2 months before clinical evidence of skeletal metastatic lesion development (T4, VAF 0.3%). TP53 p. R342* was not detected in the plasma collected 1 day after surgery and immediately after the end of radiotherapy, probably due to an effect of surgical and systemic treatments (Fig. 1D). Finally, the presence of TP53 p. R342* at low VAF was also detected in saliva samples (T0 to T3), while an increased VAF was observed 2 months before the histological diagnosis of metastasis (T4) (Fig. 1D). Based on this evidence, a salivary swab might be a more informative, sensitive, and predictive source to incicate the presence of residual neoplastic cells than plasma. One potential explanation for the higher cancer recurrence predictivity of saliva than plasma might reside in the close anatomical association between saliva and cancerous lesions [8]. Thus, in adopting a liquid biopsy approach, it is important to consider the primary cancer site and to analyze the closest body fluid to the tumor lesion. The presence of TP53 p. R342* in all analysed salivary samples might also indicate an increased risk of late locoregional recurrence. Indeed, we observed a suspected emi-tongue lesion that was not clinically established because of the patient's death. However, the detection of either residual tumor cells or pre-malignant lesions by TP53 mutation analysis remains a challenge because of the difficulty in identifying a specific clinically relevant VAF cut-off. To overcome the limitations of a TP53-based analysis, we looked for additional biomarkers, such as circulating miRNAs. Indeed, a miRNA signature able to predict poor outcome in patients with HNSCC in tissues and liquid biopsy samples was assessed [9]. Circulating levels of miR 21–3p, miR 21–5p, miR 96–5p, and miR 429 were evaluated in both serum and salivary swabs by dPCR. Notably, we found that miRNA signature expression was increased in salivary swabs collected immediately after radiotherapy (T3) and peaked up 2 months before clinical evidence of metastasis development (T4), when compared to the sample collected at T0 (Fig. 1E and F). We did not find a similar and concomitant increase of miRNA signature in serum; thereby supporting the hypothesis that biomarker modulation can be detected earlier in saliva than in serum, as saliva is the closest body fluid to the localization of the primary tumor (Fig. 1E). Of note, the increased expression of the miRNAs signature in body fluids matched with the higher VAF of TP53 p. R342*. As for miRNA-429, which was previously recognized as an exclusive biomarker of the salivary matrix, being absent in serum samples, its expression correlated with the trend observed for TP53 p. R342* circulating mutation (Fig. 1F).
Collectively, we document that: (i) a combined liquid biopsy approach is feasible; and (ii) it allows accurate detection of both genetic and non-genetic alterations which cumulatively foster and predict either local tumor relapse or metastasis. Prospectively, liquid biopsy might hold important prognostic and therapeutic implications for HNSCC patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pisani P, Airoldi M, Allais A et al. Metastatic disease in head & neck oncology. Acta Otorhinolaryngol Ital. 2020;40:S 1–86.32469009 10.14639/0392-100X-suppl.1-40-2020 PMC 7263073 · doi ↗ · pubmed ↗
- 2Markou A, Tzanikou E, Lianidou E The potential of liquid biopsy in the management of cancer patients. Semin Cancer Biol. 2022;84:69–79. 10.1016/j.semcancer.2022.03.013.35331850 · doi ↗ · pubmed ↗
- 3Malapelle U, Pisapia P, Pepe F et al. The evolving role of liquid biopsy in lung cancer. Lung Cancer. 2022;172:53–64. 10.1016/j.lungcan.2022.08.004.35998482 · doi ↗ · pubmed ↗
- 4Pantel K, Alix-Panabières C Minimal residual disease as a target for liquid biopsy in patients with solid tumours. Nat Rev Clin Oncol. 2025;22:65–77. 10.1038/s 41571-024-00967-y.39609625 · doi ↗ · pubmed ↗
- 5Zhou H, Zhu L, Song J et al. Liquid biopsy at the frontier of detection, prognosis and progression monitoring in colorectal cancer. Mol Cancer. 2022;21:86. 10.1186/s 12943-022-01556-2.35337361 PMC 8951719 · doi ↗ · pubmed ↗
- 6Wang Y, Springer S, Mulvey CL et al. Detection of somatic mutations and HPV in the saliva and plasma of patients with head and neck squamous cell carcinomas. Sci Transl Med. 2015;7:293ra 104. 10.1126/scitranslmed.aaa 8507.PMC 458749226109104 · doi ↗ · pubmed ↗
- 7Castro-Giner F, Gkountela S, Donato C et al. Cancer Diagnosis Using a Liquid Biopsy: Challenges and Expectations. Diagnostics. 2018;8:31. 10.3390/diagnostics 8020031.29747380 PMC 6023445 · doi ↗ · pubmed ↗
- 8Shanmugam A, Hariharan AK, Hasina R et al. Ultrasensitive detection of tumor-specific mutations in saliva of patients with oral cavity squamous cell carcinoma. Cancer. 2021;127:1576–89. 10.1002/cncr.33393.33405231 PMC 8084899 · doi ↗ · pubmed ↗