A novel hybrid approach to treatment of multiple mesenteric aneurysms in a patient with celiac artery occlusion from Suspected chronic median arcuate ligament syndrome
Prashanth S. Iyer, Vamsi K. Potluri, Jennifer L. Worsham, Christine L. Shokrzadeh, Zulfiqar Cheema, Charlie Cheng, Michael B. Silva

TL;DR
A new hybrid treatment approach is described for managing multiple mesenteric aneurysms in a patient with celiac artery occlusion.
Contribution
A novel hybrid treatment method is introduced for managing aneurysms in the presence of celiac artery occlusion.
Findings
Endovascular coiling and covered stent placement are alternatives to open repair for visceral artery aneurysms.
Celiac artery occlusion or compression complicates endovascular management, requiring a novel hybrid approach.
Abstract
The management of visceral artery aneurysms is evolving with endovascular coiling and covered stent placement used as alternatives to open repair. Celiac artery occlusion or compression complicates ablative endovascular management. The purpose of this report was to discuss the etiology of this uncommon phenomenon and describe a novel hybrid approach to treatment.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
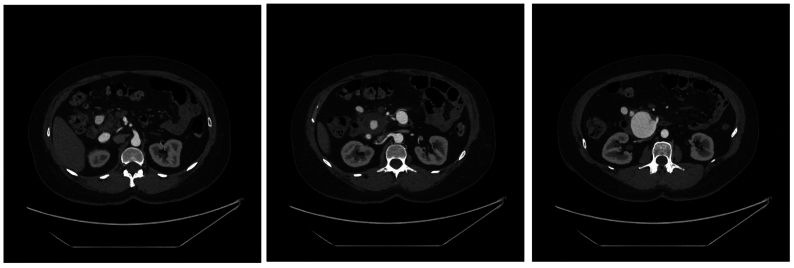 Figure 1
Figure 1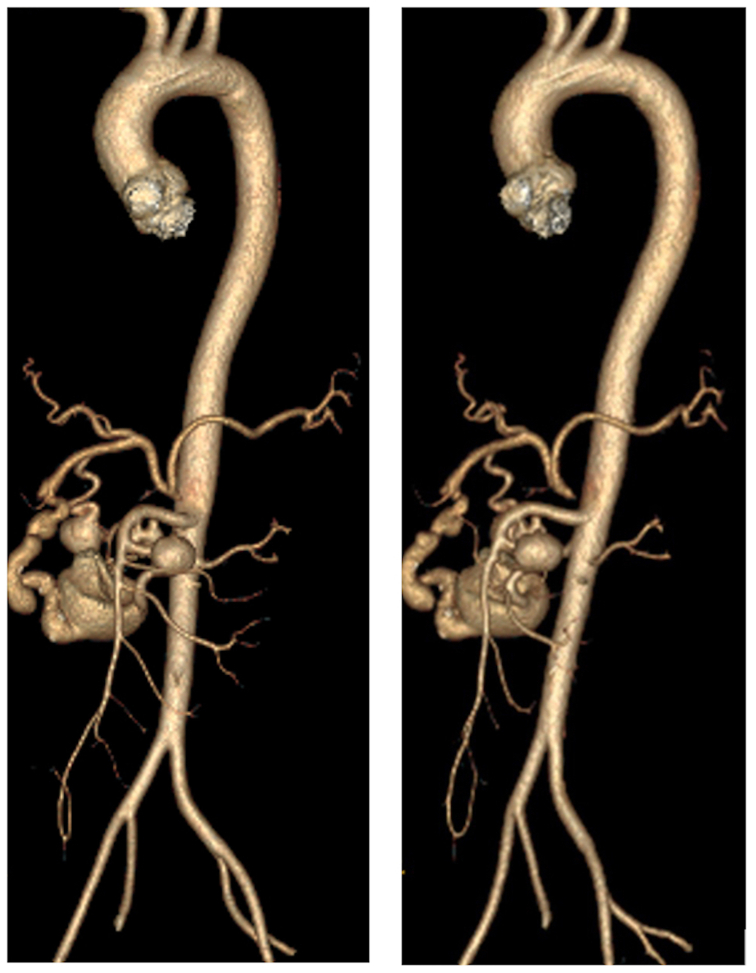 Figure 2
Figure 2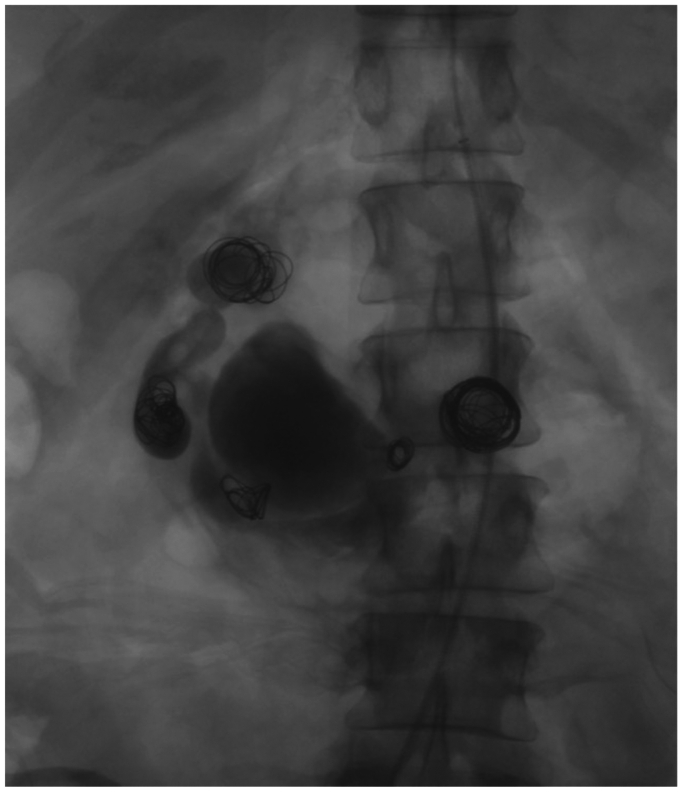 Figure 3
Figure 3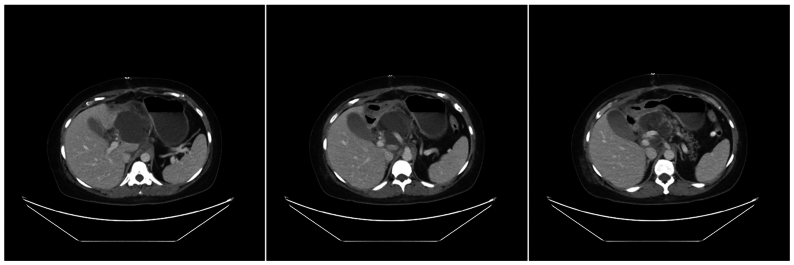 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Vascular anomalies and interventions · Aortic aneurysm repair treatments
Splanchnic artery aneurysms, defined as aneurysms of the celiac trunk, superior mesenteric artery, inferior mesenteric artery, and their respective branches, are rare and potentially life threatening. The incidence of splanchnic artery aneurysms is between 0.1% and 2.0% of all aneurysms.1, 2, 3, 4 Aneurysms of the pancreaticoduodenal arcade and the gastroduodenal artery are more likely to rupture and warrant an aggressive approach to treatment. Owing to the rarity of this condition, there is no consensus in the literature about precise indications for the repair of splanchnic artery aneurysms or the best type of surgical treatment.2^,^5 We describe the successful treatment of a patient with celiac occlusion and multiple aneurysms of the gastroduodenal and pancreaticoduodenal arteries using a hybrid approach with open aorto-hepatic artery bypass followed by intra-operative endovascular transcatheter coil embolization of the mesenteric artery aneurysms.
Case report
Informed consent was obtained from this patient before publishing this report. A 50-year-old woman with a past medical history of hypertension, hyperlipidemia, and a 10-year smoking history presented with three days of worsening epigastric pain. She was found to have an elevated lipase and was initially treated for acute pancreatitis. A computed tomography (CT) scan of the abdomen showed a nonatherosclerotic celiac occlusion with an element of extrinsic compression and five mesenteric aneurysms, with the largest aneurysm measuring 4.6 cm off the gastroduodenal artery. Additionally, the patient mentioned a remote history of postprandial abdominal discomfort and weight loss secondary to this recurring pain. Although the patient did not have a diagnosis of median arcuate ligament syndrome, the CT scan findings combined with this history is consistent with symptomatic median arcuate ligament syndrome, although this diagnosis cannot be confirmed retrospectively. She had no history of stroke or transient ischemic attack, myocardial infarction, claudication, or any other symptomatic evidence of atherosclerotic disease. There is no family history of aneurysms.
CT angiography of the thorax, abdomen, and pelvis with three-dimensional reconstruction was then obtained to further identify the anatomy of her mesenteric aneurysms (Figs 1 and 2).Fig 1. Axial cross sections of abdominal computed tomography (CT) scan with contrast shows multiple mesenteric aneurysms involving branches of the superior mesenteric artery, gastroduodenal artery, and pancreaticoduodenal arcade.Fig 2. Three-dimensional reconstruction of computed tomography (CT) angiography demonstrating one aneurysm of the gastroduodenal artery (4.6 cm), two of the superior mesenteric artery (1.7 cm, <1.0 cm), and two of pancreaticoduodenal arcades (1.3 cm, 1.5 cm) with concurrent celiac occlusion.
To rule out a mycotic aneurysm, a tagged white blood cell scan was completed with no remarkable findings. Typically, CT angiography is preferred over a white blood cell scan to diagnose a mycotic aneurysm owing to the variable sensitivity of the latter.6 However, in this case, the patient's recent episode of pancreatitis made it difficult to discern the etiology of the inflammation. A mesenteric arteriogram was obtained to better characterize the patient's anatomy and aneurysmal disease for operative planning. The angiogram demonstrated that the hepatic artery was perfused through collateralization from the superior mesenteric artery and retrograde flow through the gastroduodenal artery. Most of the patient's mesenteric aneurysms were in this pathway.
Given the patient's overall clinical presentation and number of aneurysms, we elected a surgical intervention. Although the patient was having an active episode of acute pancreatitis, making open surgery difficult, we believed the aneurysms were a contributing factor to the patient's abdominal pain and they could be the cause of her persistent pancreatic leak owing to compression and inflammation. Furthermore, given the size of the aneurysms—almost 5 cm in some places—rupture was a consideration. Finally, consideration was given to excluding each aneurysm; however, anatomical elimination of all collateral branches from the seven aneurysms risked devascularizing significant portions of circulation to the bowel.
An endovascular approach was attempted to stent the celiac artery and maintain splanchnic circulation during possible transcatheter coil embolization of the aneurysms. However, transfemoral and transbrachial attempts to recanalize the celiac occlusion were unsuccessful; there was no residual orifice for insertion of the endovascular device owing to a flush occlusion, so the procedure was converted to an open surgical repair. We proceeded to create an aortohepatic bypass between the supraceliac aorta and the common hepatic artery before ligation of the gastroduodenal artery. Although a vein would have been an ideal conduit for the bypass, the patient had no suitable vein, so a polytetrafluorethylene graft was chosen for its material characteristics and expedience. We then took an endovascular approach to treatment by gaining arterial access via the ligated gastroduodenal artery and occluded the aneurysm sacs using a total of 9 interlocking coils (Boston Scientific, Marlborough, MA). A GELFOAM (Pharmacia and Upjohn Co, Kalamazoo, MI). Thrombin slurry was also injected into the largest aneurysm (4.6 cm) to further occlude blood flow. A postoperative angiogram demonstrated flow through the patent aortohepatic bypass graft with preservation of splanchnic circulation and occlusion of the aneurysms (Fig 3). Given the emergent nature of the surgery, the postoperative period was unsurprisingly complicated by worsening of her pancreatitis. She was found to have a peripancreatic fluid collection on a postoperative CT scan (Fig 4), into which a drain was placed by interventional radiology. The fluid was infected with Serratia marcescens and had high levels of amylase and lipase; it was thought to be a pancreatic abscess secondary to her severe episode of acute postoperative pancreatitis. She was discharged on levofloxacin with the drain in place, and the drain was later removed in clinic with a repeat CT scan showing complete resolution of the peripancreatic fluid collection. This initial postoperative course was followed by return of appetite and 2 years of weight gain necessitating laparoscopic gastric sleeve surgery, which occurred without complication and resulted in appropriate weight loss. She is now 5 years out from initial surgery and remains asymptomatic. Her graft remains patent by mesenteric duplex and CT scan.Fig 3. Pos-intervention stagnation of contrast through all mesenteric aneurysms.Fig 4. Axial cross sections of postoperative abdominal computed tomography (CT) scan with contrast shows peripancreatic fluid collection, involving portion of aortohepatic bypass graft.
Discussion
Visceral aneurysms are rare but can be potentially fatal if they rupture. Unfortunately, given their rare nature, data on how to diagnosis and manage these aneurysms is scarce and primarily based on case reports.7 For gastroduodenal and pancreoduodenal aneurysms, the Society for Vascular Surgery strongly recommends intervening on all aneurysms regardless of size. The preferred intervention is coil embolization with liquid embolic agents.8 If coil embolization is not possible, the aneurysms should be treated with a covered stent or stent assisted coil embolization. If the patient has a suitable anatomy, flow-diverting, multilayer stents are an option, although they have not been well-studied.8 If flow cannot be maintained with an endovascular option, open surgical reconstruction is recommended.8 Finally, in patients with concomitant stenosis or occlusion, celiac artery reconstruction is recommended.8
The association between celiac artery stenosis or occlusion and aneurysms of the gastroduodenal and pancreaticoduodenal arteries has previously been reported in the literature. Corey et al5 reports that 24 of 36 aneurysms (66%) of these arteries were associated with severe celiac artery stenosis. Also, in a separate study de Perrot et al,9 five of six patients (83%) with aneurysms in these arteries have concurrent celiac artery stenosis or occlusion. The proposed pathophysiology behind this phenomenon is secondary to increased blood flow through these thin-walled arteries, because they serve as collateral circulation to perfuse organs typically supplied by the celiac trunk.5^,^9, 10, 11
Although endovascular therapy is becoming a more attractive option as it is further refined, data are limited on its efficacy compared with open bypass.12 A study conducted by Sharafuddin et al13 on 27 patients with total occlusions of mesenteric arteries found that 80% of patients were free of ischemic symptoms after 1 year using endovascular stenting and angioplasty and concluded that endovascular recanalization of mesenteric artery occlusion is both feasible and successful. Only 3 of these 27 patients suffered from celiac artery stenosis. In contrast, Ahanchi et al12 conducted a study on 121 patients to determine the efficacy of stenting of mesenteric arteries and found that only 18% of patients with celiac artery stenosis had primary patency after one year after treatment using balloon expandable stents, whereas freedom from bypass was 93% after 4 years. They concluded that celiac artery stenosis does not respond well to endovascular stenting. Their hypothesis was that the decrease in primary patency observed with celiac artery stenting was potentially influenced by poor anatomic location and the dynamic forces of respiration combined with the fixed ligament attachments of the diaphragm.
The management of visceral artery aneurysms is evolving with endovascular coiling and covered stent placement used as alternatives to open repair. Although open surgical treatment of digestive artery aneurysms offers good long-term results in terms of patency,14 postoperative risk of complication remains significant; Ghariani et al2 found that postoperative complications from open surgical repair were mainly respiratory (18%), digestive (18%), and renal (13%). Fankhauser et al15 reported on 176 patients with endovascular treatment of visceral artery aneurysms and found that initial intervention was successful in 98% of patients, with no complications from any percutaneous procedure; they concluded that minimally invasive management of visceral artery aneurysms, including coil embolization and endoluminal GELFOAM (Pharmacia and Upjohn Co) thrombin injection an can be used as effective treatment with a high success rate and low recurrence and morbidity.
Conclusions
Aneurysms of the visceral arcade connecting the superior mesenteric and celiac artery circulation may be associated with increased flow from dynamic changes associated with celiac artery compression or occlusion. Considering these recommendations and studies, we present a safe but durable solution with our hybrid approach to management.
Funding
None.
Disclosures
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stanley J.C.Wakefield T.W.Graham L.M.Whitehouse W.M.Jr.Zelenock G.B.Lindenauer S.M.Clinical importance and management of splanchnic aneurysms J Vasc Surg 319868368403701947 · pubmed ↗
- 2Lakin R.O.Kashyap V.S.Splanchnic artery aneurysms Cronenwett J.L.Johnston K.W.Rutherford’s vascular surgery 8th ed.2014 Elsevier Saunders 22202235
- 3Carr S.C.Pearce W.H.Vogelzang R.L.Mc Carthy W.J.Nemcek A.A.Jr.Yao J.S.Current management of visceral artery aneurysms Surgery 1201996627633886237010.1016/s 0039-6060(96)80009-2 · doi ↗ · pubmed ↗
- 4Pulli R.Dorigo W.Troisi N.Pratesi G.Innocenti A.A.Praseti C.Surgical treatment of visceral artery aneurysms: a 25-year experience J Vasc Surg 4820083343421864448010.1016/j.jvs.2008.03.043 · doi ↗ · pubmed ↗
- 5Corey M.R.Ergul E.A.Cambria R.P.The natural history of splanchnic artery aneurysms and outcomes after operative intervention J Vasc Surg 6320169499572679254510.1016/j.jvs.2015.10.066 · doi ↗ · pubmed ↗
- 6Censullo A.Vijayan T.Using nuclear medicine imaging Wisely in diagnosing infectious diseases Open Forum Infect Dis 42017 ofx 01110.1093/ofid/ofx 011PMC 541402628480283 · doi ↗ · pubmed ↗
- 7Ferrero E.Ferri M.Viazzo A.Visceral artery aneurysms, an experience on 32 cases in a single center: treatment from surgery to multilayer stent Ann Vasc Surg 2520119239352183158910.1016/j.avsg.2011.04.006 · doi ↗ · pubmed ↗
- 8Chaer R.A.Abularrage C.J.Coleman D.M.The Society for Vascular Surgery clinical practice guidelines on the management of visceral aneurysms J Vasc Surg 7220203 S 39S 3220100710.1016/j.jvs.2020.01.039 · doi ↗ · pubmed ↗