Case Report: Total intragastric mesh migration six years after diaphragmatic rupture and hiatal hernia surgery
Asma Sghaier, Mohamed Amine Elghali, Abdelrahmen Daadoucha, Amal Letaief, Itimed GHARBI, Fehmi Hamila, Sabri Youssef, Nir Messer, Asma SGHAIER, Ivan Romic, Asma SGHAIER

TL;DR
A rare case of mesh migration into the stomach six years after surgery for diaphragmatic rupture and hiatal hernia is reported.
Contribution
This case highlights the long-term complication of mesh erosion and migration, which is rarely documented in the literature.
Findings
Mesh erosion into the stomach occurred six years after the initial surgery.
The cause of the mesh migration remains unexplained, with possible links to inflammation or mesh composition.
Such long-term complications are uncommon and not well understood.
Abstract
Background: Mesh implementation to repair the hiatal space is already justified. Nevertheless, the use of this procedure is debated in regard of complications that may occur. Mesh erosion and migration are considered the most serious complications of mesh repairs. Case presentation: It has not yet been well described in the literature. We describe a case of mesh erosion of stomach, many years later after a prosthetic repair of a diaphragmatic rupture associated to hiatal hernia, is presented here because of its rarity. Conclusion: Few explanations have been put forward to explain this incident. Could it be due to inflammatory processes, or to the composition of the Meshes? As yet, there is no definitive explanation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
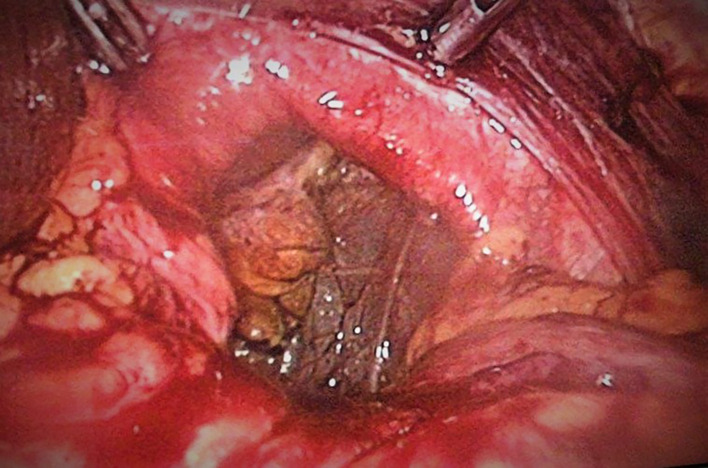 Figure 1
Figure 1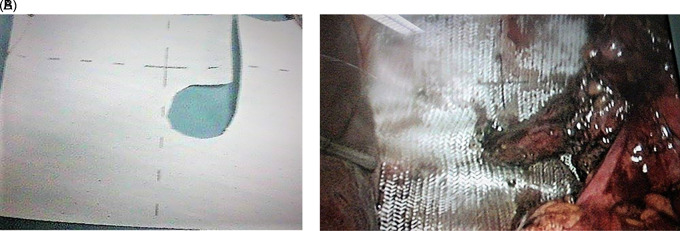 Figure 2
Figure 2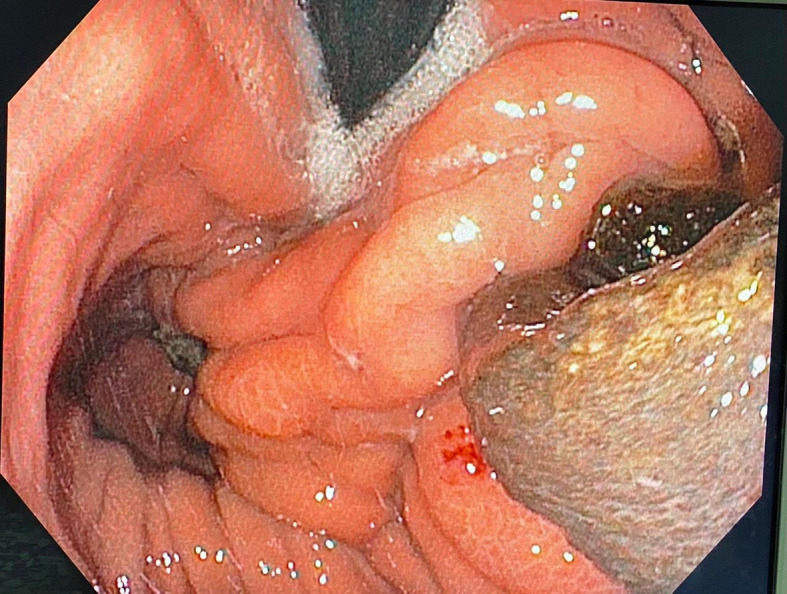 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastroesophageal reflux and treatments · Dysphagia Assessment and Management · Esophageal and GI Pathology
Introduction
Delayed presentation of traumatic diaphragmatic rupture is a challenging diagnostic and treatment with necessity of mesh reinforcement. ^ 1 ^ Mesh repair can also be proposed for hiatal hernia. ^ 2 ^ There are a few published observational studies supporting the use of mesh, convincing lower rates of recurrence with lack of long-term follow-up. Likewise, there are sparse published studies proving the complications associated with mesh in the long-term, ^ 3 ^ which provided the importance for this case. Limited related complications of mesh in such localization have been described. We describe one case of late dysphagia due to intragastric mesh migration six year after surgical reparation for diaphragmatic rupture associated with hiatal hernia.
Case report
A 52-year-old white man, with history of epigastric pain and gastroesophageal reflux disease, was operated for mixt hiatal hernia (Type III). During the operation we found that it was a left diaphragmatic rupture with a large collar with gastric migration into the thorax. The diaphragmatic hernia is located 5 cm from a wide hiatus with a sliding hiatal hernia ( Figure 1).
Diaphragmatic defect.
Intraperitoneal gastric reduction and Nissen fundoplication was performed. A two-face mesh 15×15 cm was put in place covering the orifice of the diaphragmatic rupture and the hiatal orifice by tying the esophagus ( Figure 2). Fixation was performed by crown tacks. Post-operative course was simple. The patient required level I analgesics. Transit was restored after 24 hours. The patient described no complaints, particularly no dysphagia, and the physical examination was normal.
A: Plaque double face. B: Intraoperative view of mesh placement.
By interviewing the patient post-operatively, we discovered that the patient, who belongs to the forces of order. He was a security officer and he was a victim of an accident during a pursuit and was violently struck with the wheel of his car. He consulted as a matter of emergency and had an abdominal ultrasound and was put out with analgesic treatment.
The patient remained asymptomatic for more than six years postoperatively. When, he had progressive complaints of dysphagia and weight loss. An upper gastro-intestinal endoscopy showed a dilated esophagus, crossed cardia easily without protrusion with evidence of anti-reflux montage and migration of mesh into the stomach. Pneumatic dilation of antireflux montage with a 30-mm balloon was performed ( Figure 3).
Endoscopic view of the mesh into stomach.
An attempt at endoscopic removal of the mesh had failed. A magnetic resonance imaging examination had not described any signs in favor of a diaphragmatic defect.
The decision was then made to operate the patient laparoscopically and to remove the mesh.
The patient was operated on, the per operative exploration discovered the presence of several adhesions at the supra meso-colic level. A longitudinal gastrotomy was carried out which made it possible to reveal the mesh that was inside and to extract it with the few staples that were attached ( Figure 4).
Mesh after surgical extraction.
The postoperative course was simple. The patient was discharged at day six.
Discussion
Mesh repair is becoming increasingly necessary to manage large diaphragmatic rupture. ^ 4 ^ But use of mesh at the hiatus is yet controversial because of possible complications that may occur. ^ 5 ^ ^–^ ^ 7 ^ Recommendation with a fairly high level of evidence concerning indications of prosthetic mesh does not clearly developed. Many procedures were proposed. Tension-free procedure consist of mesh setting without tight suture to procure excessive tension whereas the on-lay technique with consolidation of the defect closure by mesh. The materiel could be placed in an anterior, posterior, or circular position with a hole for the passage of the esophagus. ^ 7 ^
The mesh used for hiatal reinforcement are made usually of non-resorbable material. It should have a very low risk of post-operative adhesions, and can be easy to be manipulate proceeding by laparoscopic approach.
Polypropylene mesh seems to offer most of these requirements; however, it is susceptible to be responsible of intraperitoneal adhesions and also sometimes fistulas. ^ 8 ^ Prosthetic reinforcement, though associated with a low rate of hernia recurrence, has particular drawbacks like this case of migration into stomach that we described in this article. Indeed, there are two considerable complications due to meshes: Parietal erosion and esophageal stenosis. The incidences of these two main complications ranged in literature between 0%–0.49% ^ 8 ^ and 3.9% ^ 9 ^ respectively depending on the series. However, surgical management is crucial to treat both conditions. A predisposition to esophageal stenosis succeeding the setting up of meshes produced by biological materials and toward parietal erosion after the use of polytetrafluoroethylene and polypropylene meshes has been developed by retrospective studies. ^ 10 ^ Furthermore, stitches around a mesh placed above the fundoplication may be responsible of dysphagia, and contact of the mesh with the esophagus may leads to erosion, as illustrated in our case. Moreover, a surgical approach might provide a crucial role in decreasing the incidence of complications due to mesh. ^ 10 ^ The techniques proposed for this purpose are tension-free repair with mesh placement without crus suturing to avoid excessive tension and the on-lay technique with reinforcement of the crucial closure by mesh. The on-lay technique is usually performed in all cases of hiatal hernia, independently of hernia size. ^ 11 ^
Further recent studies concluded that mesh might be associated with fewer short-term recurrences, and the biological mesh was involved with improved short-term quality of life. Nevertheless, these advantages were offset by more dysphagia, ^ 12 ^ which is why most experienced practitioners recommend mesh use exclusively for carefully selected cases. ^ 13 ^ For our patient we could not explain this intragastric migration of the Mesh. Would it be related to the fixation by the tackers and the nature of the Mesh? We do not have valid proof and explanations.
Conclusions
Our case, even though it is rare, demonstrates this, as we are led to re-operate a patient and to be faced with technical difficulties and often even a conversion to open surgery to retrieve the mesh that migrated inside the digestive tract. The mesh type may provide a role in the complication rate, with synthetic mesh being more implicated. The simultaneous co-existence of an intraperitoneal infection may also be responsible, although that must be proven by well-conducted studies and further controlled randomized trials.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Al-Nouri O Hartman B Freedman R : Diaphragmatic rupture: Is management with biological mesh feasible? Int. J. Surg. Case Rep. 2012;3(8):349–353. 10.1016/j.ijscr.2012.04.011 22584115 PMC 3376699 · doi ↗ · pubmed ↗
- 2Spiro C Quarmby N Gananadha S : Mesh-related complications in paraoesophageal repair: a systematic review. Surg. Endosc. 2020 Oct;34(10):4257–4280. 10.1007/s 00464-020-07723-0 32556700 · doi ↗ · pubmed ↗
- 3BernabéMQ Adelina EC : Use of absorbable meshes in laparoscopic paraesophageal hernia repair World. J. Gastrointest. Surg. 2019 October 27;11(10):388–394. 10.4240/wjgs.v 11.i 10.388 PMC 682193431681460 · doi ↗ · pubmed ↗
- 4Sirbu H Busch T Spillner J : Late bilateral diaphragmatic rupture: challenging diagnostic and surgical repair. Hernia. 2005 Mar;9(1):90–92. 10.1007/s 10029-004-0243-4 15351874 · doi ↗ · pubmed ↗
- 5Veronique M Marc Z Myriam D : Complications of Mesh Repair in Hiatal Surgery: About 3 Cases and Review of the Literature. Surg. Laparosc. Endosc. Percutan. Tech. 2012;22:222–225.10.1097/SLE.0b 013e 318253 e 44022874707 · doi ↗ · pubmed ↗
- 6Idrissi A Mouni O Bouziane M : Intraesophageal Migration of a Paraesophageal Hernia Mesh: A Case Report. Cureus. 2022 Apr 21;14(4):e 24339. 10.7759/cureus.24339 35607570 PMC 9123389 · doi ↗ · pubmed ↗
- 7Tam V Winger DG Nason KS : A systematic review and meta-analysis of mesh versus suture cruroplasty in laparoscopic large hiatal hernia repair. Am. J. Surg. 2016 January;211(1):226–238. 10.1016/j.amjsurg.2015.07.007 26520872 PMC 5153660 · doi ↗ · pubmed ↗
- 8Priego P Ruiz-Tovar J Pérez de Oteyza J : Long-term results of giant hiatal hernia mesh repair and antireflux laparoscopic surgery for gastroesophageal reflux disease. J. Laparoendosc. Adv. Surg. Tech. A. 2012;22(2):139–141. 10.1089/lap.2011.0340 22146080 · doi ↗ · pubmed ↗