Impact of COVID-19 Pandemic on Hand Surgery Volume in Japan
Hidemasa Yoneda, James Curley, Katsuyuki Iwatsuki, Masaomi Saeki, Nobunori Takahashi, Michiro Yamamoto

TL;DR
The study found that the COVID-19 pandemic initially reduced hand surgery volumes in Japan, but most procedures recovered, with a notable shift to outpatient surgeries.
Contribution
This study provides new insights into how the pandemic affected hand surgery practices and led to a shift in surgical settings in Japan.
Findings
Scheduled surgeries dropped by 44% during the first pandemic wave, especially for arthroplasties and polydactyly.
Trauma surgeries remained stable, while some procedures like tendon repair increased during the pandemic.
Outpatient surgeries increased significantly for wrist and forearm fractures and amputations.
Abstract
Objectives: The impact of the COVID-19 pandemic on hand surgery in Japan has not been fully elucidated. This study investigated changes in the volume of hand surgery practiced during the pandemic. Methods: We used the National Database Open Data Japan (NDB-ODJ), a comprehensive repository of healthcare data administered by the government, to investigate changes in the volume of hand surgery services delivered during the COVID-19 pandemic. The type and number of upper extremity surgical procedures was examined during each month of the pandemic to identify associations. Results: During the first wave in the spring of 2020, scheduled surgeries decreased by 44% compared to pre-pandemic levels, with arthroplasties, osteotomies, and polydactyly surgeries experiencing the largest reductions. Trauma surgeries remained relatively stable, and some procedures like tendon repair and replantation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
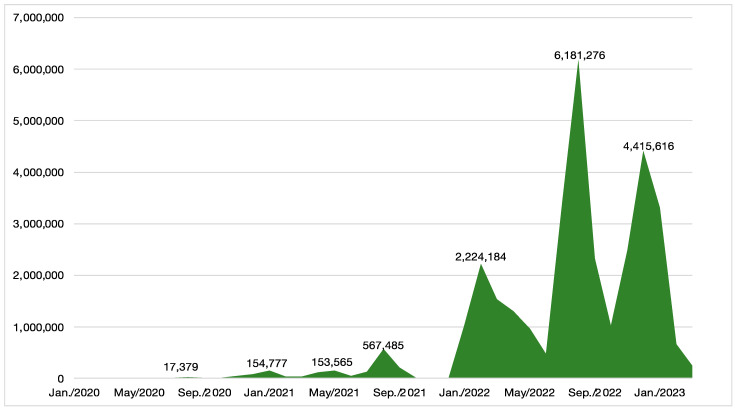 Figure 1
Figure 1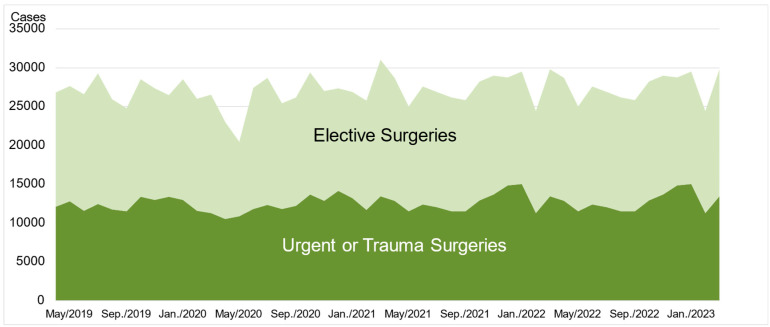 Figure 2
Figure 2- —Japan Society for the Promotion of Science
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and healthcare impacts · Genital Health and Disease · Dermatological and COVID-19 studies
1. Introduction
The COVID-19 pandemic, which emerged in 2020, had a significant impact on surgical treatments worldwide. Lockdowns were implemented in many countries to curb the spread of the virus, imposing substantial restrictions on people’s social lives. The reduction in group activities and outdoor pursuits led to a marked decrease in sports-related injuries and, consequently, a significant decline in the number of patients seeking treatment for traumatic injuries [1,2].
Healthcare resources were reallocated to prioritize the treatment of critically ill patients with respiratory failure. Medical supplies were preferentially used for the prevention and treatment of COVID-19, and masks and ethanol became temporarily scarce. Some general wards were converted into infectious disease wards, and intensive care physicians and pulmonologists were dedicated to treating the surge of COVID-19 patients. To compensate for the burden of long, challenging shifts, patient surges, and personnel shortages, in part due to their own infections, cross-departmental staffing was implemented [3].
Following the declaration by the World Health Organization (WHO) of a Public Health Emergency of International Concern on 30 January 2020, the American College of Surgeons recommended postponing elective surgeries except for emergency procedures on 13 March 2020. Based on these pronouncements, practitioners of orthopedic surgery in Japan, primarily led by the Japanese Orthopedic Association, also responded. Surgeons swiftly adapted to the pandemic situation by adjusting hospital resources and postponing elective surgeries [4].
In the United States, the number of hand surgeries significantly decreased, particularly during the emergence of challenging COVID-19 variants and surges in cases [5,6]. In the United Kingdom, there was an increase in the proportion of non-operative management and remote follow-up for hand trauma patients [7]. In India, there was also an increase in the proportion of conservative treatment for the management of hand trauma [8].
Studies show that Japan successfully contained COVID-19 early on without implementing lockdowns or mandatory restrictions on behavior [9,10]. Notwithstanding this, reports indicate a general decline in surgical volumes in Japan during the pandemic [11,12]. To our knowledge, the impact of the COVID-19 pandemic specifically on hand surgery treatment in Japan has not been reported.
Hand surgery specialists are responsible for treating patients suffering from acute trauma, a substantial responsibility given that the number of those requiring intervention may be comparable to, or even greater than, those seeking elective surgeries. Irrespective of other factors, the volume of trauma patients presenting to a healthcare system follows predictable, generally stable trends. Postponing or redirecting such regularly occurring urgent care to allocate medical resources to critically ill COVID-19 patients posed particular challenges.
We became interested in how the pandemic affected the overall practice of hand surgery, including trauma and elective procedures, and wanted to document how healthcare professionals navigated these challenges. Therefore, we aimed to investigate and elucidate the effects of the COVID-19 pandemic on hand surgery in Japan.
2. Materials and Methods
2.1. Data Source
We utilized data sets from the National Database of Health Insurance Claims and Specific Health Checkups of Japan (NDB) [13]. Japan has universal health coverage and claims are reimbursed through its statutory health insurance system. Anonymized, aggregated data from the NDB, published annually as NDB Open Data Japan (NDB-ODJ), include statistics on medical procedures and pharmaceuticals dispensed and can be downloaded from the website of the Ministry of Health, Labour, and Welfare of Japan (MHLW). Data up to March 2023 are currently available. The NDB-ODJ is a comprehensive database covering all hospitals with 20 beds or more; however, it does not include statistics on claims arising from occupational and motor vehicle injuries. Therefore, we do not have a complete understanding of the treatment trends for patients utilizing these insurance schemes.
2.2. Definition of the Pandemic Period
The novel coronavirus was first reported in Wuhan, China, in December 2019. As previously mentioned, the WHO declared a Public Health Emergency of International Concern in January 2020 and characterized it as a pandemic that March. The present study tracks with the pandemic periods determined by the MHLW (Table 1) in which successive waves of the pandemic were determined based on the number of patients who were receiving intensive care for COVID-19 [14]. While acknowledging that the pandemic was not over, the WHO withdrew its emergency declaration in May 2023, legally mandated infection control measures were lifted, and COVID-19 began to be managed more akin to seasonal influenza. Therefore, for this study, we elected to define this date as the end of the pandemic. The pandemic periods detailed in Table 1 were analyzed in two distinct phases. The initial phase encompasses periods 1 through 5, while the later phase covers periods 6 through 8.
2.3. Analytic Methods and Statistical Processing
We extracted the total number of upper extremity surgical procedures as a representation of hand surgery performed. The specific procedures are listed in Table 2. These were broadly classified into elective surgeries and urgent surgeries performed for trauma, vascular compromise, and other acute conditions. The number of surgical procedures was investigated on a monthly basis. The number of new COVID-19 cases and the number of critically ill patients were extracted from the MHLW website [15].
In the NDB-ODJ, counts of 10 or fewer are not reported. Therefore, we forcibly entered a value of 5 in such cases. Based on the values, we investigated the following:
- Changes in the total number of surgical procedures during the pandemic.
- Comparison of the number of surgical procedures before and after the first pandemic period.
- Comparison of the number of surgical procedures before the pandemic, in the first half (initial phase) of the pandemic, and in the second half (later phase) of the pandemic.
- Changes in the number of outpatient surgical procedures before the pandemic, in the first half (initial phase) of the pandemic, and in the second half (later phase) of the pandemic.
For statistical processing, the Mann–Whitney U test was used for comparisons between two groups. Spearman’s rank correlation coefficient was used to analyze the correlation between two variables. The Kruskal–Wallis test was used to assess the distribution among three or more groups, while Dunn’s test with Bonferroni adjustment was performed as a post-hoc test. In all tests other than those with a Bonferroni adjustment, a p-value of less than 0.05 was considered statistically significant. IBM SPSS Statistics 29.0 (Armonk, NY, USA) was used for the statistical analysis.
The items analyzed included: trends in the number of critically ill COVID-19 patients, new infections, and surgical procedures; changes in surgical procedures during the first period of the pandemic; the number of surgical procedures before and after the pandemic; and the proportion of outpatient and inpatient treatments before and after the pandemic.
3. Results
3.1. Trends in the Number of Critically Ill Patients, New Infections, and Surgical Procedures
Figure 1 shows the trends in the number of critically ill patients and new infections. Figure 2 shows the trends in the numbers of all surgical procedures investigated in this study. The number of surgical procedures for the examined items decreased by more than 10% in April and May 2020 during the first wave of the pandemic, and in May 2021 and May 2022. These decreases were related to the prevalence of variant COVID-19 strains (Figure 2), but there was no correlation between the number of infected individuals, critically ill patients, and procedures. The largest decrease occurred during the first wave in April and May 2020, with no significant fluctuations observed thereafter.
3.2. Change Between Surgical Procedures Before and After the First Pandemic Period
Regarding changes in the number of surgical procedures during the first pandemic period, a comparison between January 2020 (immediately before the pandemic) and May 2020 revealed that the average decrease in the number of elective surgeries was 44%, with nearly half of these procedures being reduced (Table 3). In contrast, the number of trauma surgeries remained relatively stable. Among elective surgeries, the number of arthroplasty, osteotomy, and polydactyly surgeries decreased to less than half. While some trauma and emergency surgeries decreased during this period, the number of tendon suture, amputation, nerve suture, and replantation procedures increased.
3.3. Changes in Surgical Volume Before and After the Pandemic
Compared to the pre-pandemic period, the volume of many surgical procedures decreased during the first half of the pandemic. Among elective surgeries, significant decreases were observed in osteotomies, while among trauma and emergency surgeries, there were significant decreases in finger pinning, as well as in open reduction and internal fixations (ORIF) (Table 4). Other surgical procedures showed only minor fluctuations. There were notable differences, however, in the number of Dupuytren contracture and amputation surgeries, which increased compared to the pre-pandemic period. Overall, the rates of many of the surgical procedures that were negatively impacted in the first half of the pandemic recovered to normal in the second half.
3.4. Changes in the Proportion of Outpatient Surgeries
There was a shift towards outpatient surgery for many elective and urgent surgical procedures, with a decrease in the proportion of inpatient surgeries (Table 5). Among elective surgeries, the proportion of outpatient procedures increased significantly for tenolysis, arthroplasty, carpal tunnel release, ulnar nerve transposition, and Dupuytren contracture surgery. Among trauma and emergency surgeries, a significant increase was observed in outpatient procedures for open reduction and internal fixation of wrist and forearm fractures as well as amputations. These trends continued into the second half of the pandemic.
4. Discussion
In this study, we investigated the impact of COVID-19 on the practice of hand surgery in Japan. We found that the number of trauma surgeries was largely unaffected by the pandemic, although there were some fluctuations. It is highly likely that the demand for surgery in the hand region was met during this period, even amidst reports suggesting that the incidence of trauma decreased. We observed a decrease in the number of non-traumatic cases during the first period of the pandemic, but these numbers recovered in the second period and remained stable thereafter.
Initially, we anticipated that the number of surgeries would have either remained the same or decreased after the onset of the pandemic compared to before, in line with reports from around the world. However, when examined by category, the number of surgeries during the pandemic significantly increased for two procedures: “fingertip amputation” and “Dupuytren contracture surgery”. It is possible that surgeons, impelled to prioritize and reallocate medical resources, resorted to performing fingertip amputation rather than replantation, as the former is simpler and requires a shorter operative time. However, since the number of replantation surgeries did not change significantly during the same period, we presume that the increase was influenced by the rise in finger gangrene cases associated with the increase in COVID-19 patients. We attributed the increase in the number of Dupuytren contracture surgeries to the commercial withdrawal of the Collagenase Clostridium histolyticum (CCH) injection just before the pandemic, forcing patients who were eligible for pharmacological treatment to opt for surgery [16].
The pandemic in Japan led to a shift in hand surgery practice, with a transition from inpatient to outpatient care when feasible. In Japan, fees for medical services are set by the government. Patients bear responsibility for contributing a certain percentage of the total cost, but there is monthly cumulative cap on out-of-pocket expenses. Therefore, the typical direct cost paid by a patient for inpatient treatment does not differ significantly from that of outpatient treatment. Moreover, hospitals have a financial incentive to provide inpatient surgery because the reimbursable billing amount is higher for inpatient compared to outpatient treatment. For these reasons, patients with concerns ranging from managing postoperative pain to inconvenience due to short-term follow-up have often been encouraged to choose inpatient surgery, even for conditions that would commonly be treated on an ambulatory basis in other countries. For example, in 2019, just before the pandemic, around 40% of patients undergoing carpal tunnel release were treated on an inpatient basis. However, during the COVID-19 pandemic, the reallocation of medical staff and hospital beds made it necessary to minimize inpatient admissions. Additionally, to avoid the risk of nosocomial infections, there was a shift towards day surgery and outpatient care.
While approximately 80% of hand trauma treatment in the United States is performed under general anesthesia [17], most hand trauma surgeries in Japan are performed under local or regional anesthesia, eliminating the need for recovery room facilities, making the transition to outpatient surgery easier. Although we were unable to investigate it in this study, the duration of hospital stays may also have been affected. In the United States, the length of hospitalization for patients undergoing lower extremity joint arthroplasty was shortened to 1.7 days during the pandemic [18]. The shift to outpatient care and reduction in length of stay for inpatient admissions were natural consequences of maintaining surgical services during the pandemic.
Among the upheavals engendered by COVID-19, in Japan, the pandemic appears to have marked an inflection point for providers, patients, and payers of healthcare services. We believe that the shift from inpatient to outpatient hand surgeries, a direct if unanticipated effect of the pandemic, will be sustained. In April 2024, the Ministry of Health, Labour, and Welfare significantly reduced the “Short term stay surgery basic fee” applied to hospitalizations of several days [19]. With the loss of profits from inpatient services, hospitals will likely encourage patients to opt for outpatient rather than inpatient care. Furthermore, from 2025, the out-of-pocket costs to consumers will be gradually increased and, depending on annual income, are expected to almost double for some patients [20]. We predict that the shift to outpatient surgery will further accelerate as both patients and healthcare providers face increased burdens and reduced benefits from inpatient care.
Will Japanese healthcare professionals be able to utilize the lessons learned when a similar pandemic occurs in the future? Basic infection control measures were thoroughly implemented among healthcare professionals. When severe COVID-19 cases increased, non-urgent treatments were suspended, and medical resources were inevitably triaged to focus on urgent and critically ill patients. As a result, Japan was able to control the COVID-19 pandemic relatively quickly compared to other countries. The shift to outpatient surgery, although an unintended consequence, is a trend that will likely continue, with careful consideration of the necessity of hospitalization and minimizing the length of stay to reduce nosocomial infections and contain costs.
This study has several limitations. As described previously, claims arising from occupational and motor vehicle injuries are not included in the NDB-ODJ, and the study lacks understanding of the treatment trends for patients utilizing these insurance schemes. Additionally, there is a possibility of aggregation errors due to coding inconsistencies inherent in such insurance reimbursement databases. While the NDB-ODJ has the advantage of being unrestricted and generally accessible, the data are released after an approximate two-year lag, making timely reporting challenging. Despite these limitations, this study was able to clarify the impact of the COVID-19 pandemic on hand surgery.
5. Conclusions
Overall, the COVID-19 pandemic had a minimal impact on the volume of hand surgery in Japan. By 2023, the number of most types of hand surgery procedures had recovered to pre-pandemic levels. However, there was a notable increase in amputation and Dupuytren contracture surgeries compared to the pre-pandemic period. The number of patients who experienced treatment delays due to the pandemic was low compared to other countries. Additionally, the concentration of medical resources during the pandemic led to a shift towards outpatient treatment for many procedures in hand surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Devarakonda A.K. Wehrle C.J. Chibane F.L. Drevets P.D. Fox E.D. Lawson A.G. The effects of the COVID-19 pandemic on trauma presentations in a level one trauma center Am. Surg.20218768668910.1177/000313482097371533231483 PMC 7688434 · doi ↗ · pubmed ↗
- 2Sabbagh R.S. Shah N.S. Kanhere A.P. Hoge C.G. Thomson C.G. Grawe B.M. Effect of the COVID-19 pandemic on sports-related injuries evaluated in US emergency departments Orthop. J. Sports Med.2022102325967122107537310.1177/2325967122107537335224117 PMC 8873554 · doi ↗ · pubmed ↗
- 3Hamada S. Moromizato T. Narita M. Taniguchi K. Shibuya K. Tokuda Y. Association between hospital internal medicine physician workforce and patient admissions during the COVID-19 pandemic in Japan BMC Health Serv. Res.2023236510.1186/s 12913-023-09043-036681836 PMC 9862232 · doi ↗ · pubmed ↗
- 4Stenseth N.C. Dharmarajan G. Li R. Shi Z.L. Yang R. Gao G.F. Lessons learnt from the COVID-19 pandemic Front. Public Health 2021969470510.3389/fpubh.2021.69470534409008 PMC 8365337 · doi ↗ · pubmed ↗
- 5Liu I.Z. Whitehead J. Schlafly M. Pakhchanian H. Raiker R. Snoddy M.C. Quantifying the impact of COVID-19 on hand and wrist surgery procedural volume: A national analysis of 381,046 cases J. Hand Surg. Glob. Online 2023515115810.1016/j.jhsg.2022.12.00436573172 PMC 9771746 · doi ↗ · pubmed ↗
- 6Uhlman K. Churchill I. Dydynsky R. Johnston S. Leveille C. Mc Rae M. Mc Rae M. The impact of the COVID-19 pandemic on case volume and wait times of elective hand procedures: A retrospective chart review study Plast Surg.20242292550324127654410.1177/2292550324127654439545215 PMC 11559549 · doi ↗ · pubmed ↗
- 7Shaw A.V. Holmes D. Jansen V. Fowler C. Wormald J.C.R. Wade R.G. Taha R. Reay E. Gardiner M.D. RSTNCOVID Hand Collaborative RSTN COVID Hand: Hand trauma in the United Kingdom and Europe during the COVID-19 pandemic J. Plast. Reconstr. Aesthet. Surg.20238425826510.1016/j.bjps.2023.04.07737354711 PMC 10148718 · doi ↗ · pubmed ↗
- 8Saha S. Dash S. Ansari M.T. Bichupuriya A.D. Gupta A.K. Singhal M. Optimising hand surgery during COVID-19 pandemic J. Hand Surg. Asian Pac. Vol.202126849110.1142/S 242483552150013233559584 · doi ↗ · pubmed ↗