Use of sodium–glucose cotransporter‐2 inhibitors among Aboriginal people with type 2 diabetes in remote Northern Territory: 2012 to 2020
Matthew J. L. Hare, Winnie Chen, Thomas Berhane, Sumaria M. Corpus, Louise J. Maple‐Brown

TL;DR
This study examines the use and outcomes of a diabetes medication called SGLT2i in Aboriginal people with type 2 diabetes living in remote Northern Territory communities from 2012 to 2020.
Contribution
The study provides insights into the real-world use and safety of SGLT2i in a high-risk, understudied Aboriginal population with type 2 diabetes.
Findings
SGLT2i use increased over time among remote Aboriginal people with T2D.
Safety data revealed no major concerns specific to this population.
The study highlights the potential benefits of SGLT2i in managing diabetes-related complications.
Abstract
Aboriginal people in remote Northern Territory communities experience the highest burden of type 2 diabetes (T2D) globally. Sodium–glucose cotransporter‐2 inhibitors (SGLT2i) improve cardiac and renal outcomes in selected populations. However, safety in this context is unknown. We investigated SGLT2i use and outcomes in remote Aboriginal people with T2D between 2012 and 2020.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
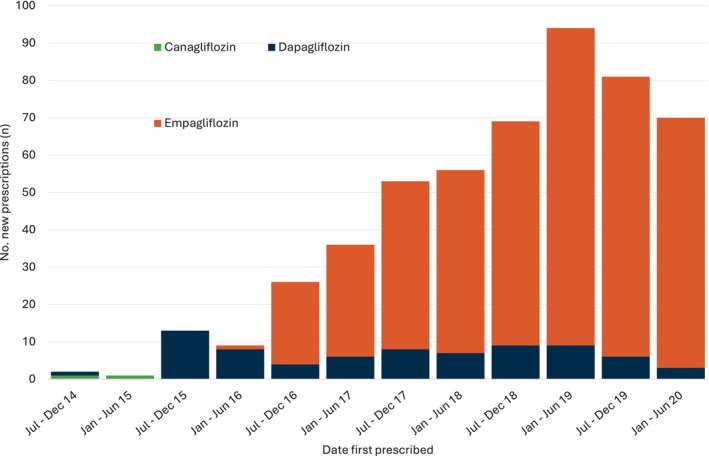 Figure 1
Figure 1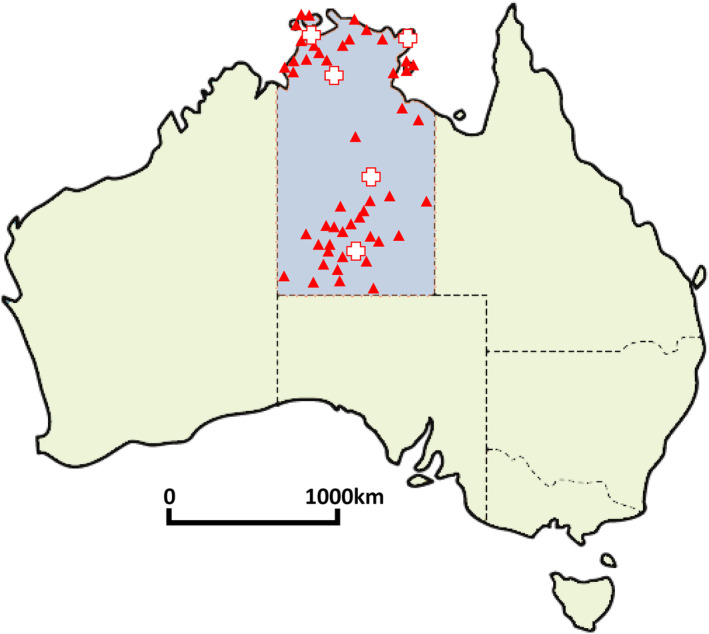 Figure 2
Figure 2- —National Health and Medical Research Council, Investigator Grant 10.13039/501100000925
- —Diabetes Australia Research Program
- —Sylvia and Charles Viertel Charitable Foundation ‐ Clinical Investigator Award
- —Australian Diabetes Society Skip Martin Fellowship
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Hyperglycemia and glycemic control in critically ill and hospitalized patients · Pancreatic function and diabetes
Aboriginal people living in remote areas of the Northern Territory (NT) experience some of the highest burden of type 2 diabetes (T2D) in the world, with a reported adult prevalence of diabetes of up to 40% in some areas of the NT.1 Diabetes in the NT is associated with high rates of complications, including chronic kidney disease (CKD) and cardiovascular disease.2, 3
Sodium–glucose cotransporter‐2 inhibitors (SGLT2i) improve cardiac and renal outcomes for select patient populations.4, 5 However, the safety profile of SGLT2i among Aboriginal people in the remote NT is unknown. Potential adverse effects include volume depletion, diabetic ketoacidosis (DKA), genitourinary infections and amputations. Heightened risk of such events is foreseeable in the NT due to climate, food insecurity, complex diabetes phenotypes6 and high background rates of infection7 and amputation.8 Thus, our study aimed to investigate the use and outcomes of SGLT2i for T2D in remote Aboriginal people living in NT between 2012 and 2020.
We investigated a retrospective cohort of all Aboriginal patients with T2D prescribed an SGLT2i at all 48 NT Health remote primary healthcare clinics in the NT, between October 2012 (first SGLT2i approved by Therapeutic Goods Administration) and June 2020. A map of included clinic sites is displayed in Figure 1. These clinics are all sole providers in remote Aboriginal communities. The included cohort was formed using extraction of prescription data from the Primary Care Information System (PCIS), which is the electronic medical record system used in all NT Health remote community clinics. No specific inclusion criteria were used to select patients with T2D; however, during the study period up to 2020, SGLT2i were only Pharmaceutical Benefits Scheme (PBS)‐indicated for T2D.9 Clinical data were collected via manual review of individual patient records in PCIS and also the electronic medical records system for all public hospitals in the NT. Baseline data collected included demographics, anthropometry, comorbidities, smoking status and medications. Clinical effectiveness indicators were compared between baseline, and at 6‐month intervals up to 2 years from SGLT2i commencement – these clinical indicators included haemoglobin A1c (HbA1c), weight, blood pressure, estimated glomerular filtration rate (eGFR) and urine albumin–creatinine ratio (uACR). Given the longitudinal nature of routinely collected data and possibility of multiple measurements, the closest reading (e.g. HbA1c) within 6 months of the relevant 6‐, 12‐, 18‐ and 24‐month interval was selected. Adverse events and discontinuation could occur at any time point while on SGLT2i therapy. Therefore, adverse events and discontinuation data were collected up until the end of the data collection period at January 2021. The NT Human Research Ethics Committee (NT HREC 2020‐3721), and Aboriginal and Torres Strait Islander Advisory Group of the Diabetes across the Lifecourse: Northern Australia Partnership approved the study.
A total of 519 Aboriginal people from 48 remote NT communities was included. The mean age of the cohort was 47 years (standard deviation 12 years), and 55% were female. There was a high proportion of people with comorbidities including 401 (77%) with CKD and 95 (18%) with cardiovascular disease (Table 1). The majority of people taking an SGLT2i were prescribed empagliflozin, and the number of new prescriptions during the study period increased over time (Fig. 2).
At a median follow‐up of 2.0 years, use of SGLT2i was associated with modest improvements in HbA1c and weight (Table 2). There was minimal decline in renal function (eGFR, uACR) between baseline and follow‐up. At the end of the follow‐up period, 28% of patients discontinued therapy. Seventeen (3.3%) deaths, nine non‐traumatic amputations (1.8%), six severe hypoglycaemia events (1.2%), one DKA event (0.2%) and no cases of Fournier gangrene (0%) were observed.
Discussion
We report the first study to our knowledge of SGLT2i use and outcomes among Aboriginal people in remote Australian communities. Australians with diabetes living in more remote and/or disadvantaged socioeconomic areas may have reduced access to SGLT2i and other newer diabetes medications,10 but this association has not been confirmed in Aboriginal and Torres Strait Islander populations.11 Our study is timely as expanded clinical indications for SGLT2i, including heart failure and CKD, are driving further increases in utilisation.9 The strength of our study is that it includes individual patient data from a large number of remote primary healthcare clinics. The NT‐wide cohort in this study has similar characteristics in terms of age and sex distribution but higher mean HbA1c (9.9% in this study, vs 7.9%) compared to our previous study of all patients with diabetes within the same remote Australian communities.1
In summary, we found that SGLT2i were being prescribed to people likely to benefit based on international trial evidence. The cohort being prescribed SGLT2i had a high prevalence of CKD, CVD and cardiovascular risk factors. SGLT2i prescription was accompanied by modest improvements in weight and HbA1c over time (reduction of 2 kg and 0.4% respectively), consistent with 2‐year findings of major international studies such as the EMPA‐REG and DECLARE trials12, 13 and a previous study within an urban Aboriginal and Torres Strait Islander cohort.14 Adverse events such as amputations and DKA (1.8% and 0.2% respectively) from this study are also comparable with other major trials.15
A limitation of this study was that only prescription data from the included electronic medical record system was available for analysis. Secondary use of electronic medical record data is subject to variations in data accuracy and completeness. Furthermore, routinely collected electronic medical record data do not provide information on medication dispensing or adherence, which has previously been described as a potential issue in remote primary NT Health remote primary health clinics.16 If medication adherence is optimised, it is plausible that the observed clinical effect of SGLT2i may be greater than what has been reported in this study.
While the findings of this study are largely reassuring, the possibility of higher rates of rare, but serious, adverse events in this unique context is not excluded given the limited sample size and lack of a comparison group. Future studies investigating the effectiveness and safety profile of SGLT2i in remote NT Aboriginal populations including a larger patient cohort, with matched controls, would be crucial as use of SGLT2i increases within these contexts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hare MJL , Zhao Y , Guthridge S , Burgess P , Barr ELM , Ellis E et al. Prevalence and incidence of diabetes among Aboriginal people in remote communities of the Northern Territory, Australia: a retrospective, longitudinal data‐linkage study. BMJ Open 2022; 12: e 059716.10.1136/bmjopen-2021-059716 PMC 912576035569825 · doi ↗ · pubmed ↗
- 2Hare MJL , Maple‐Brown LJ , Shaw JE , Boyle JA , Lawton PD , Barr ELM et al. Risk of kidney disease following a pregnancy complicated by diabetes: a longitudinal, population‐based data‐linkage study among Aboriginal women in the Northern Territory, Australia. Diabetologia 2023; 66: 837–846.36651940 10.1007/s 00125-023-05868-w PMC 10036460 · doi ↗ · pubmed ↗
- 3Barr ELM , Cunningham J , Tatipata S , Dunbar T , Kangaharan N , Guthridge S et al. Associations of mortality and cardiovascular disease risks with diabetes and albuminuria in urban indigenous Australians: the DRUID follow‐up study. Diabet Med 2017; 34: 946–957.28375555 10.1111/dme.13360 · doi ↗ · pubmed ↗
- 4Zala A , Maple‐Brown L , Shaw J , Hare M . Current evidence and practical guidance for the use of sodium–glucose co‐transporter‐2 inhibitors in type 2 diabetes. Aust J Gen Pract 2021; 50: 225–230.33786548 10.31128/AJGP-05-20-5432 · doi ↗ · pubmed ↗
- 5Zelniker TA , Wiviott SD , Raz I , Im K , Goodrich EL , Bonaca MP et al. SGLT 2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta‐analysis of cardiovascular outcome trials. Lancet 2019; 393: 31–39.30424892 10.1016/S 0140-6736(18)32590-X · doi ↗ · pubmed ↗
- 6Wicks MM , Barr ELM , Maple‐Brown L . Pancreatitis and post‐pancreatitis diabetes in Central Australia. Intern Med J 2023; 53: 568–576.34779564 10.1111/imj.15620 · doi ↗ · pubmed ↗
- 7Boyd R , Patel M , Currie BJ , Holt DC , Harris T , Krause V . High burden of invasive group A streptococcal disease in the Northern Territory of Australia. Epidemiol Infect 2016; 144: 1018–1027.26364646 10.1017/S 0950268815002010 · doi ↗ · pubmed ↗
- 8Stuart L , Kimmel L , Jolly A . Incidence of lower limb amputation in Central Australia. Aust Health Rev 2021; 45: 361–367.33647229 10.1071/AH 20182 · doi ↗ · pubmed ↗