Expert Consensus on Dry Needling Practices for Headache: An International Delphi Study Protocol
Thomas Perreault, Jan Dommerholt, César Fernandez-de-las-Peñas, Lars Arendt-Nielsen, Barbara Cagnie, Stefano Di Antonio, Matteo Castaldo

TL;DR
This paper outlines a study to create guidelines for using dry needling to treat headaches by gathering expert opinions through a structured process.
Contribution
The study introduces a novel international Delphi method to establish consensus-based clinical recommendations for dry needling in headache treatment.
Findings
A literature review was conducted to inform the initial survey items for the Delphi study.
Consensus will be defined as 75% agreement among experts across three rounds of questionnaires.
The goal is to produce clinical guidelines that can improve both research and patient care in headache treatment.
Abstract
Background: Dry needling is increasingly utilized by clinicians in the treatment of patients with headaches. Although current evidence supports the use of dry needling for reducing headache pain, needling approaches are inconsistent among published studies, and no guidelines on dry needling for headaches have been established. Methods: A study will be conducted using the Delphi method, consisting of three rounds of questionnaires sent to an expert panel of clinicians and researchers. Results: To guide the development of the initial survey, we completed a literature review of articles related to dry needling for headaches. A steering committee will assess the initial survey items synthesized from the literature search and provide recommendations for the first and subsequent rounds of the study. Percentage agreement will be the primary measure throughout all rounds of this study. We…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
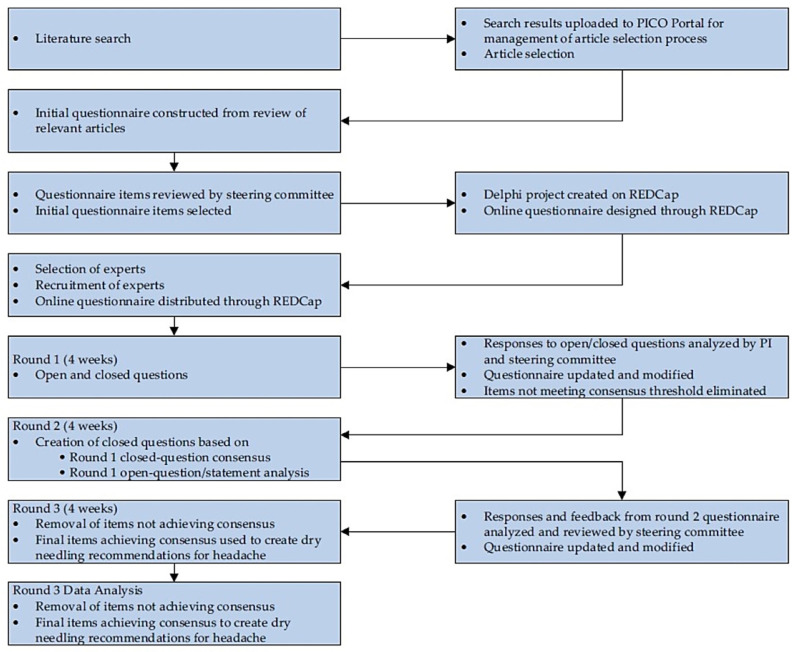 Figure 1
Figure 1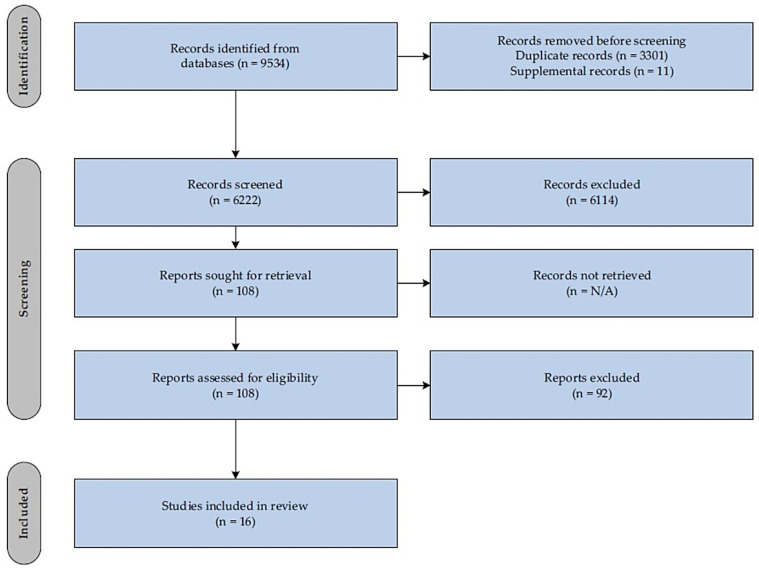 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMyofascial pain diagnosis and treatment · Migraine and Headache Studies · Sympathectomy and Hyperhidrosis Treatments
1. Introduction
On any given day, it is estimated that 15.8% of the world population will experience a headache [1]. According to the International Headache Society, a multitude of headache phenotypes exists, classified as a primary or secondary headache disorder [2]. Primary headaches include migraine and tension-type headache (TTH), among others, with an estimated pooled prevalence in the global population of 14% (95% CI 12.9–15.2) and 26% (95% CI 22.7–29.5), respectively [1]. Even if its pathogenesis is incompletely understood, migraine is characterized by a cyclic sensitization of cortical and subcortical brain areas that reached its peak during the headache phase, when an increased activation of the trigeminovascular system has been observed [3]. Migraine is reported to be the most burdensome of all headaches and is ranked within the top ten leading causes of disability worldwide [4]. In fact, it is the leading cause of years lived with disability in people between the ages of 15 and 49 years old [5]. Migraine presents as headache attacks lasting 4–72 h of moderate or severe intensity and typically have a pulsating quality and unilateral location. They can be aggravated by routine physical activity and are accompanied by nausea, photophobia, or phonophobia [2]. On the other hand, TTH pain does not worsen with routine physical activity and does not feature nausea. Photophobia or phonophobia may be present in some chronic cases. In addition, TTH is typically bilateral and has a pressing or tightening quality with mild to moderate intensity, lasting minutes to days [2]. Cervicogenic headache (CGH) is a secondary headache disorder that occurs by pain referral of cervical origin to the head from upper cervical joints or muscles, among other structures [2,6,7]. Convergence of nociceptive afferents from the upper cervical region, with neurons also receiving input by afferents of the trigeminal nerve, may explain the phenomenon of referred pain to the head [6]. The prevalence of CGH is far less researched compared to migraine and TTH; however, previous studies estimate the prevalence of CGH to be as low as 0.17% in the general population [8] to as high as 4.1% [9]. An earlier study also reported that patients with CGH experience similar negative effects on health-related quality of life as do patients with migraine and TTH, most significantly in the domain of physical functioning [10]. Whilst headache types differ in diagnostic criteria, it is common for their clinical findings and symptomology to overlap in some sub groups of patients [11]. To further complicate the clinical headache diagnosis, one headache may co-exist with another, such as TTH and migraine [12].
Lifestyle factors such as poor sleep, low levels of physical activity, poor dietary habits, alcohol use and smoking, among others, may negatively impact headache characteristics [13,14]. Yet, educating individuals suffering from migraine, TTH or CGH to modify these lifestyle factors, when possible, and to keep an accurate headache diary may improve headache care [15]. In addition, headache types like migraine are associated with psychosocial comorbidities such as depression and anxiety, which add to the headache burden [16]. Consideration of these factors in the overall management of headache are being increasing investigated [12,13].
Cervical musculoskeletal impairments are prevalent in patients with migraine, CGH, and TTH [17,18,19]. These include increased pain sensitivity and dysfunction in the upper cervical spinal joints, restricted cervical range of motion, forward head posture, decreased function of the deep neck flexor muscles, reduced thoracic spine mobility, and trigger points in muscles of the head and neck [20,21,22,23,24]. A trigger point (TrP) is defined as a hypersensitive spot located within a taut band of skeletal muscle that is painful upon stimulation, and typically features referred pain and associated phenomena [25]. Tender points are also associated with primary and secondary headache types, commonly along the peri cranial and cervical region [26,27]. Like TrPs, tender points exhibit hyperalgesia and other signs reflective of central sensitization [28,29], but do not share the same pathophysiological features that are characteristic of TrPs, such as localized muscle contractures [30] and elevated concentrations of algesic and inflammatory substances [31]. Phenotypically, a TrP may exhibit nociceptive, nociplastic, neuropathic or mixed-type pain features in nature. That is, TrPs may be a primary source of pain or altered nociception, or secondary and comorbid with another disorder [25]. According to recent evidence, nociceptive input from TrPs in the craniofacial, craniomandibular and cervical region can also project to the trigeminocervical complex (TCC) and may precipitate headache pain via convergence of cervical and trigeminal afferents in the upper cervical spinal cord [32]. Trigger points are treatable musculoskeletal impairments, and therefore often targeted with various interventions in the clinical setting for the management of headache disorders [33].
Clinicians often use needling therapies for the treatment of TrPs in patients with headache. These include TrP injections using local anesthetics [33], botulinum toxin [34] or dry needling, where no pharmacological substance is used [35] and acupuncture [36]. Dry needling (DN) involves the insertion of solid monofilament needles through the skin and into various tissues of the body, most commonly into TrPs, to reduce pain and improve function [37]. Acupuncture is based on classical theories and principles of Traditional Chinese Medicine and involves the use of needles into acupuncture points to alter or regulate the flow of energy along meridian pathways [38]. Although DN and acupuncture differ in historical background and theories, both practices are commonly used for treating pain and share similar neurophysiological mechanisms [38]. Furthermore, many acupuncture points prescribed for treating headaches are in or around muscles of the head and neck that harbor TrPs [36,39].
De Pauw et al. reported consensual agreement across experts that impairments in muscle length/stiffness are good clinical indicators for the use of TrP therapy in patients with TTH in their Delphi study [40]. A previous study on patients with migraine reported that identification of TrPs in the head and neck muscles, specifically those TrPs eliciting migraine-like pain, has utility when planning to administer needling interventions [41]. Yet, DN may also target nerve innervation fields [42], periosteal structures and cervical entheses [43] for the management of headache pain. Dry needling is used by physicians, physical therapists, and chiropractors, among others [44,45], in many countries of the world for the treatment of neuromusculoskeletal disorders, including headache. Research on DN has grown over the past twenty years. In fact, a recent bibliometric analysis identified 458 articles published on the topic of DN for myofascial pain syndrome (MPS) alone, produced from 46 countries across the world [46]. Studies exploring the fundamental mechanisms of DN corroborate evidence for neurophysiological and biochemical effects that are elicited at peripheral [47,48], spinal [49,50], and supraspinal levels [37,51] that together serve to reduce nociception and modulate pain.
A recent umbrella review on DN concluded it is effective for reducing pain in the short term for musculoskeletal conditions associated with TrPs across all body regions, after analyzing nearly two hundred randomized controlled trials across thirty five systematic reviews [52]. In addition, DN was superior to the sham, placebo, and no intervention for reducing pain intensity. While no superiority was shown comparing DN to other interventions used in clinical practice, this review and others support using DN as an adjunct therapy [52,53]. For headaches, a previous review reported that DN reduced headache pain in all eight studies analyzed, including migraine [54]. Yet, Vázquez-Justes et al. reported high heterogeneity in the methodologies across DN studies, which rendered the authors unable to perform a meta-analysis. Furthermore, the authors supported the idea of developing specific protocols to increase consistency of methods across DN studies for headache [54]. Another recent meta-analysis reported that DN was not statistically better than other interventions for reducing headache pain intensity in the short term in patients with TTH (SMD −1.27, 95% CI = −3.56 to 1.03), CGH (SMD−0.41, 95% CI = −4.69 to 3.87), or mixed headaches (migraine and TTH) (SMD 0.03, 95% CI = −0.42 to 0.48). However, DN was shown to be effective for reducing disability and headache frequency compared to other interventions in patients with TTH and CGH [55]. According to Pourahmadi et al. most studies investigating dry needling for headache suffered from failure to report on allocation concealment and statistical heterogeneity. In addition, most studies poorly described DN procedures and failed to reference a specific DN approach. Moreover, no analysis regarding a specific DN technique on outcomes for any headache type could be performed due to the high variability in approaches used across studies [55]. It is conceivable that improved consistency of DN procedures across headache studies will allow researchers to observe if specific DN parameters impact study outcomes. For example, the physiological mechanisms of DN for pain modulation are influenced by needling dosage [48,50]. More specifically, the duration of needling is among the various dosage parameters and can influence the effect of DN on the autonomic nervous system [56]. Thus, if improved consistency in dosage parameters is achieved across studies using DN for headaches, researchers may begin investigating the impact of various DN dosages on outcomes for specific headache types.
In a recent DN review, the authors could not determine the impact of DN dosage on pain outcomes due to the wide variation in dosing variables and inconsistency in the needling techniques used between studies [57]. For example, only 2 of the 18 studies reported the number of needles used and only 4 of the 14 studies, which reported the elicitation of local twitch responses, specified how many occurred. As a result, the authors suggested reporting dosage parameters with specific recommendations on how to report DN technique, number of needles used per session, region treated, number of muscles and specific muscles treated per session, if a local twitch response (LTR) occurred (and if so how many), visit frequency and total visits [57]. Likewise, a survey study of physical therapists in the United States investigated DN practice patterns for the management of musculoskeletal pain and found significant variability in the use of needling techniques among respondents [58]. A more recent systematic review found considerable variation in and underreporting of DN procedures across more than twenty DN studies [59]. Consequently, the authors voiced concern over the potential impact this heterogeneity may have on the internal validity of many DN randomized controlled studies. Therefore, the Delphi process was recommended to assimilate a set of guidelines for DN [59]. Since studies investigating the use of DN for headaches are also widely inconsistent in needling approaches, and clinical guidelines on DN for headaches have not been established, a Delphi study would be an appropriate method to establish expert-based guidelines on DN for headaches [60].
In the healthcare setting, a Delphi study can generate consensus on a given research question through expert interviews using a questionnaire or other survey instrument. Typically, a structured questionnaire is issued over two to three rounds, undergoing several revisions after analyzing participant responses and feedback from the previous rounds. The aims of this Delphi study will be to develop a broad consensus on DN practices for the management of CGH, TTH, and migraine to inform practicing clinicians and further research studies on expert consensus-based practices for DN in these headaches. Additionally, it is our aim to contribute a study protocol that is consistent with established Delphi study guidelines to the clinical and research community involved in the use of dry needling for headache management.
2. Methods
2.1. Study Design
According to the Mass General Brigham (MGB) Institutional Review Board, the current project meets the criteria for exemption and was approved by the MGB Research Information Security Office (protocol #2024P001341). In addition, this protocol is registered on Open Science Framework (OSF) (https://doi.org/10.17605/OSF.IO/VBSY9). This study will implement a three-round Delphi design in accordance with the Guidance on Conducting and Reporting Delphi Studies (CREDES) (see Table S1) and other recommendations [61,62,63] along with direction from published Delphi studies in rehabilitation [18,40,64,65]. This study will consist of three rounds of online questionnaires sent to an expert panel of clinicians and researchers, both nationally and internationally. A systematic literature review of articles related to DN for headache was initially performed across several databases to inform the selection of survey items. A combination of closed and open-ended questions was developed to guide the first round of the survey. A steering committee has been established, and prior to the production phase of the Delphi, the committee will assess the study methodology, assess the initial survey items synthesized from the literature search, and provide any further recommendations for items to inform the first round, and subsequent rounds, of the Delphi study. This expert committee consists of six academic and clinical experts from the following countries: Spain, Denmark, Italy, Belgium, and the United States. Each committee member has over ten years of clinical and academic experience, has declared no conflicts of interest and has published on the topics of headache and/or dry needling extensively. After collection of participants’ responses and feedback from the first round and other rounds, the questionnaire will be refined and reissued to progress toward probable consensus.
Research Electronic Data Capture (REDCap) will be used to create, issue, and assist with analyzing electronic questionnaires from each round. Study data will also be collected and managed using REDCap electronic data capture tools hosted by Mass General Brigham Research Computing, Enterprise Research Infrastructure & Services (ERIS) group. Research Electronic Data Capture is a secure, HIPAA-compliant, web-based application designed to support data capture for research studies [66,67].
Research data will be shared with the steering committee and a statistician for interpretation and analysis. In this study, data will be collected via electronic questionnaires delivered to the participants’ personal or institutional email address. Members of the steering committee, other than the PI, will have no direct contact with expert participants regarding this Delphi study process. Steering committee members will support the PI in the development of the initial questionnaire, help with data analysis and with formalizing future iterations of the questionnaire. All personal identifiers will be removed from the data sets and replaced with placeholder values. The controller of the data is the institution of the PI of the study. Finally, participants will be informed that the PI may reach out to them for further communications following the completion of the study when clarification of responses or feedback is needed for proper analysis of the study data, or for further data analyses related to this study only. Figure 1 presents the Delphi study schema.
2.2. Subject Selection
To capture a diverse sample, experts from a diverse range of institutions globally will be asked to participate. Eligible participants will include but not be limited to physicians, physical therapists, osteopaths, and chiropractors with at least 5 years of clinical experience in the management of headaches (CGH, TTH, and migraine) and at least 3 years of experience using DN for the treatment of patients with headache disorders. In addition, experts with 10% or more of their total treatment population that is headache related will be preferred [40]. Eligible individuals may also be academic researchers not currently in practice, but they must meet the defined clinical experience and DN experience requirements with headache management. Moreover, they must have achieved primary authorship or co-authorship of at least one relevant peer-reviewed publication on the topic of headache. The steering committee will be responsible for recruiting international experts, specifically experts identified through the literature search as authors, clinicians and/or academic professionals known to the members of the steering committee to have expertise in headache management, along with experts who are international DN instructors who meet the eligibility criteria.
There are no official guidelines available for researchers to use when selecting experts for a Delphi study, or determining appropriate sample size [68]. Based on a systematic review of the Delphi literature, Junger et al. confirmed that, at a minimum, the criteria used for the selection and recruitment of experts should be explained in the methodology, along with survey response rates and information related to the participants expertise [61]. For this study, we will lean on clinical and academic experience/knowledge related to headache and dry needling, along with authorship of peer-reviewed publications, which are commonly used criteria to define expertise in Delphi studies [68]. We aim to recruit and retain 30 experts from multiple countries, which is similar to the number of participants included in previous Delphi studies on the topic of headache [18,40] and DN [65]. Moreover, selecting an expert panel size larger than 30 may not improve the Delphi results and potentially contributes to lower survey response rates [69]. Importantly, a homogenous group of 30 experts with specialized knowledge and experience, in our case DN for headaches (CGH, TTH and migraine), is sufficient to obtain stable results from a Delphi survey [70]. Thirty participants that best represent the expert population most appropriate for this study will be chosen, following agreement to participate.
2.3. Subject Enrollment
A purposive sample of individuals will be invited via email to participate in this Delphi study. An email invitation will be sent to the potential panelists and will include a Delphi study fact sheet to provide information about the study. Following agreement to participate, a participant demographic questionnaire will be issued to assess eligibility for the study. Prior to the round one questionnaire, participants will answer questions related to basic demographics (age, sex, country of residence, current institution, or clinic) along with professional credentials, experience related to clinical practice, relevant academic experience, and DN experience for headache management. Upon confirmation of interest and eligibility, a REDCap survey will be sent electronically to the participant for rounds one through three. The principal investigator will be responsible for executing and managing all aspects of the survey process through REDCap. For participants who are non-English speaking, a translated version of the invitation email, and surveys for the study will be provided. Following consent to participate, each panelist will be asked to commit to participation in each round of the Delphi. Experts will be informed that participation is completely voluntary and there are no consequences for withdrawing from the study at any time or refusing to participate. Participants will be provided with a Delphi study information fact sheet explaining the type of data being collected and the reason for carrying out such a study. Potential participants will be provided with a clear explanation of the anticipated process, and an explanation that participation would last a period of 3–4 months.
2.4. Study Procedures
The initial survey items chosen for round one was supported by a systematic review of the literature on DN for migraine, TTH, and CGH. PubMed, CINAHL, and Web of Science databases were searched for articles published up to 17 October 2023. The criteria for inclusion were (1) articles written in the English language, (2) articles must either be a systematic review, meta-analysis, or randomized controlled trial investigating the effects of DN on migraine, TTH, or CGH; (3) articles that include outcome measures relating to either headache frequency, headache pain intensity, or disability. No limits were placed on the date of publications. Two reviewers who are Doctors of Physical Therapy, TP and JD were involved in the creation of the search syntax for each database, with the help of a Health Science Librarian who was also consulted in the literature search process. To optimize the chances of identifying relevant studies, we used a dual-reviewer title and abstract screening process [71,72]. The same two reviewers, TP, and JD, uploaded all search results data to the PICO Portal for automatic removal of duplicates and to carry out the process of screening titles and abstracts. Screening of titles and abstract together has been shown to have high precision in yielding relevant articles for systematic reviews [73]. In total, 9534 articles were identified, as shown in Table 1.
Following removal of duplicates, 6233 articles remained. After the screening of titles and abstracts, 6125 were excluded, leaving 108 for full-text review. Articles were excluded for the following reasons based on our inclusion criteria: wrong study design, not a dry needling study and article not in English. Finally, 16 articles fully met the inclusion criteria [7,42,43,54,55,74,75,76,77,78,79,80,81,82,83,84]. Figure 2 below presents the study selection process.
2.4.1. Round One
Following the literature review, each of the sixteen studies was summarized by two reviewers, TP and JD, and the relevant methods and DN details of each study were organized thematically. Recording the details of the needling procedures across studies resulted in an archetypical set of dosage parameters on DN for headache that were used to develop the initial questionnaire. In addition, the overall treatment regimens, and the rationale behind the use of DN for headache were recorded. A previous DN Delphi study on plantar heel pain used the Standards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA) guidelines to develop their survey items [65], yet not all items recommended by the STRICTA guidelines are relatable to DN. Therefore, we followed recommendations from recent reviews on DN [57,59] in addition to STRICTA guidelines [85] when summarizing the studies, and to guide the development of the initial questionnaire, as shown in Table 2.
Two physical therapists, TP, and JD, developed the initial questionnaire. Topics identified from the study summaries in Table 2 were examined and translated into the initial survey items (see Table S2). Particular attention was given to the rationale and details of the needling procedures across studies to observe consistencies on how DN is administered in the treatment of headache. The initial survey items best reflected the common approaches on DN for headache. Each of the items included in the initial questionnaire related to DN rationale and DN dosage will be asked for each headache type (migraine, TTH and CGH). In addition, the initial survey will ask experts open-ended questions about any further DN considerations according to each headache type. Before distributing the initial survey to participants, the questionnaire will be pilot tested by three clinical and research experts from the steering committee.
Experts will rate their level of agreement for the included items using a 5-point Likert-scale, except for the initial open questions that will be included as part of the first round. Answers to open questions will be analyzed by the Principal Investigator (PI) and steering committee and converted to closed questions for the next survey round. After each item and open-ended question, there will be space for expert comments. Participant responses from the open-ended questions will be coded alongside each other and analyzed to identify concepts, categories and themes [88]. The PI will organize the data into a Microsoft Excel table and present it to the steering committee. An iterative process will ensue to determine what additional closed question items can be created for round two of the questionnaire based on the thematic analysis. Following the final round of the study, data from REDCap will be exported for statistical analysis.
We define that consensus has been reached when 75% percent of participants “strongly agree” or “agree” with an item. A percentage agreement value of 75% is commonly chosen for determining consensus among Delphi studies, according to a recent review [89]. Participants will not need to vote further on items achieving consensus in round one, and therefore items achieving consensus will not be included in the round two questionnaire. Items achieving 75% agreement or more for “disagree” or “strongly disagree” will be removed. Items that received an overall rating of “unsure” or that were rated as “strongly agree” or agree” by less than or equal to 50% of participants during the first and second round will require further investigation by the steering committee and items/questions will be amended for the next round. That is, if items that are believed to be important fall just below the threshold for consensus, the PI and steering committee will consider including these items as posteriori considerations provided that sufficient justification is provided. A table will be created to provide explanations for amended items moving into the next round. Following each round, the steering committee will review all questionnaire data, participant responses and comments, and the PI will make edits accordingly to prepare for the next survey round.
2.4.2. Round Two
Themes originating from the open-ended responses and analysis of data from the structured questions of round one will guide the formation of the round two questionnaire. In round two, participants can modify their answers from round one based on results and feedback from that round. Participants will be able to see the amount of consensus on statements from the previous round, and where they answered compared to the group. Participants will not need to vote further on items achieving consensus in this round, and therefore items achieving consensus will not be included in the round three questionnaire. Items achieving 75% agreement or more for “disagree” or “strongly disagree” will be removed. Items that received an overall rating of “unsure” or that were rated as “strongly agree” or “agree” by less than or equal to 50% of participants during the first and second round will require further investigation by steering committee and items/questions will be amended for the next round. A table will be created to provide explanations for amended items moving into round three.
2.4.3. Round Three
In round three, participants can modify their answers from round two based on results and feedback from that round. Participants will be able to see the amount of consensus on statements from the previous round, and where they answered compared to the group. If consensus is still not reached on a particular item, items will be reviewed and revised according to the criteria by the PI and steering committee and a fourth round will be performed. If all items have reached consensus according to our methods after round three, the questionnaire process will be complete. However, a fourth round may be performed to investigate expert agreement on an official list of recommendations for DN in headache management comprising all consensual items.
2.5. Statistical Analysis
Standard descriptive statistics will be used to describe the demographic characteristics of participants based on the first group of questions of the round one questionnaire. Anonymous answers from the open-ended questions following round one will be analyzed thematically as described in the study procedures section of this protocol. Percentage agreement calculations will be the primary measure throughout all rounds of this Delphi study [90]. However, depending on the data, measures of dispersion and central tendency may be used in place of or in addition to percentage agreement, using Interquartile Range (IQR) and/or Median, respectively, as these measures are also widely used in Delphi studies to define consensus [68]. Data will be analyzed using SPSS 30.0.0 or other statistical software at the end of each round. Wilcoxon rank-sum tests will be used for the final round to evaluate stability and consistency of responses between the final two rounds, with the aim of moving toward consensus [68]. The response rates of participants will also be measured following each round, which is increasingly investigated in Delphi studies [60,62].
3. Results
We plan to present our results through high-impact publication for the benefit of healthcare professionals, researchers, and patients. Outcomes will be displayed quantitatively (i.e., percentage agreement calculations, and possibly IQR and Median) and qualitatively. At the time of submission of this Delphi study protocol, the first round of this study is planned to begin on or before 1 March 2025.
4. Discussion
Dry needling has steadily evolved in clinical practice since its appearance in the literature as far back as the 1940s. Research interest in DN has grown substantially over the last 30 years, with studies investigating the use of DN for headache emerging in the early to mid-1980s [78,91]. At present, a recent meta-analysis study now supports DN as an effective intervention for reducing headache frequency and intensity across a range of headache types, with follow-ups of at least up to 3 months [92].
This study protocol describes the research design for a three, potentially four, round Delphi study to reach expert consensus for recommendations on the use of DN in headache management. The Delphi technique is a firmly established methodology for pursuing consensus on topics related to healthcare, and formulating recommendations based on expert opinion [60,69]. Having consensus-driven recommendations on DN for headaches would assist researchers in designing the methods and protocols for future clinical trials incorporating DN for headaches, and for this reason, a Delphi study will be performed. In addition, clinicians would benefit from having expert recommendations to reference prior to and during the delivery of DN treatments for patients with headaches, as no guidelines currently exist. After reviewing the literature on DN for headache, our observations are much like recent reviews on DN. That is, inconsistencies in DN procedures (i.e., dosage parameters and DN techniques) and practice patterns are prevalent across studies [57,59], especially those studies investigating DN for headache [55].
We also identified wide variations in treatment rationales across studies, with some studies referring to the peripheral mechanisms of DN and others leaning on more spinal or central mechanisms of action. In addition, the clinical indications for DN in headache management also fluctuate across studies. Most of the studies we reviewed administered DN to TrPs for treatment of headache, regardless of headache type. For example, Gildir et al. selected only active TrPs (TrPs that caused the clinical pain compliant when stimulated, i.e., at least part of the headache was reproduced with TrP stimulation) to be needled in patents with TTH [81,93]. Rezaeian et al. performed DN to active TrPs in the sternocleidomastoid muscle (SCM) in patients with migraine [76]. In contrast, Kamali et al. administered DN to TrPs in the suboccipital, temporalis, upper trapezius, or SCM muscles in patients with TTH, without specifying if TrPs elicited headache symptoms upon examination, or if they were latent [82]. A recent study, published after our review of the literature, analyzed the effects of DN on reducing the number of active TrPs in the cranial or facial muscles in patients with TTH, and reported a significant reduction in the total number of active TrPs, along with reductions in headache intensity [94]. None of the studies we reviewed specifically addressed latent TrPs (TrPs that are clinically dormant, are only painful when stimulated, and have similar characteristics as active TrPs) with DN in patients with headaches. Like active TrPs, latent TrPs in the muscles of the head and neck may be a source of local motor dysfunction and peripheral nociception that contribute to muscle pain as well as trigeminocervical and central sensitization [95,96]. It is conceivable that DN may be indicated not only for treatment of active TrPs, but also of latent TrPs in patients with headaches, especially since a recent study found that the pain-relieving mechanisms of DN are intrinsically related to reducing nociceptive input from TrPs, helping to attenuate peripheral sensitization [97]. However, regarding headache management, a multimodal approach that includes DN is recommended considering that nociplastic and neuropathic phenotypes of TrPs may be present, which are related to comorbid factors [25]. Nevertheless, according to a recent systematic review, it remains uncertain whether the TrP should be targeted for DN to be effective in the treatment of headaches [54]. Gaining expert consensus regarding dosage parameters, needling techniques, treatment rationales and clinical indications for the use of DN in headache would be valuable to research and treatment practices. In addition, the insights gained from this Delphi study may also be applicable to the management of various sub-types of headaches.
This Delphi study protocol does have some limitations. First, the questionnaire in its present form does not include items related to psychosocial factors like depression or anxiety, or lifestyle factors, which are relevant in the management of migraine, TTH and CGH. It is possible, however, that certain open-ended questions may lead to the inclusion of such items in other iterations of the questionnaire. Second, survey and questionnaire instruments used in Delphi studies may be subject to certain biases and misinterpretations, which may impact the credibility of the research being performed [98,99]. Third, because most of the research on DN for headache is focused on migraine, TTH and CGH, according to our review of the literature, not all headache types will be investigated in this study. Lastly, while we will include a diverse sample of experts from across the globe, there will be no specific limit to the number of potential experts from one region or country.
5. Conclusions
This study seeks to gather expert opinions regarding DN practices for headaches and synthesize them into group consensus via implementing a three-round Delphi study. Having expert guidelines and recommendations for DN practices for the management of cervicogenic, TTH, and migraine headaches would serve to inform researchers in designing the methods and specific protocols for future studies incorporating DN for these headache types. In addition, clinicians would benefit from having expert guidelines and recommendations to reference prior to and during the delivery of DN treatments for patients with headaches.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stovner L.J. Hagen K. Linde M. Steiner T.J. The global prevalence of headache: An update, with analysis of the influences of methodological factors on prevalence estimates J. Headache Pain 2022233410.1186/s 10194-022-01402-235410119 PMC 9004186 · doi ↗ · pubmed ↗
- 2Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition Cephalalgia 201838121110.1177/033310241773820229368949 · doi ↗ · pubmed ↗
- 3Ashina M. Migraine N. Engl. J. Med.20203831866187610.1056/NEJ Mra 191532733211930 · doi ↗ · pubmed ↗
- 4Stovner L.J. Nichols E. Steiner T.J. Abd-Allah F. Abdelalim A. Al-Raddadi R.M. Ansha M.G. Barac A. Bensenor I.M. Doan L.P. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016 Lancet Neurol.20181795497610.1016/S 1474-4422(18)30322-330353868 PMC 6191530 · doi ↗ · pubmed ↗
- 5Steiner T.J. Stovner L.J. Vos T. Jensen R. Katsarava Z. Migraine is first cause of disability in under 50s: Will health politicians now take notice?J. Headache Pain 2018191710.1186/s 10194-018-0846-229468450 PMC 5821623 · doi ↗ · pubmed ↗
- 6Bogduk N. Govind J. Cervicogenic headache: An assessment of the evidence on clinical diagnosis, invasive tests, and treatment Lancet Neurol.2009895996810.1016/S 1474-4422(09)70209-119747657 · doi ↗ · pubmed ↗
- 7Sedighi A. Nakhostin Ansari N. Naghdi S. Comparison of acute effects of superficial and deep dry needling into trigger points of suboccipital and upper trapezius muscles in patients with cervicogenic headache J. Bodyw. Mov. Ther.20172181081410.1016/j.jbmt.2017.01.00229037632 · doi ↗ · pubmed ↗
- 8Knackstedt H. Bansevicius D. Aaseth K. Grande R.B. Lundqvist C. Russell M.B. Cervicogenic headache in the general population: The Akershus study of chronic headache Cephalalgia 2010301468147610.1177/033310241036844220974607 · doi ↗ · pubmed ↗