A large right side cardiac benign metastasizing leiomyoma of uterine origin as a rare cause of acute breathlessness
Mahmoud Morsy, Mohammed Ellisy

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
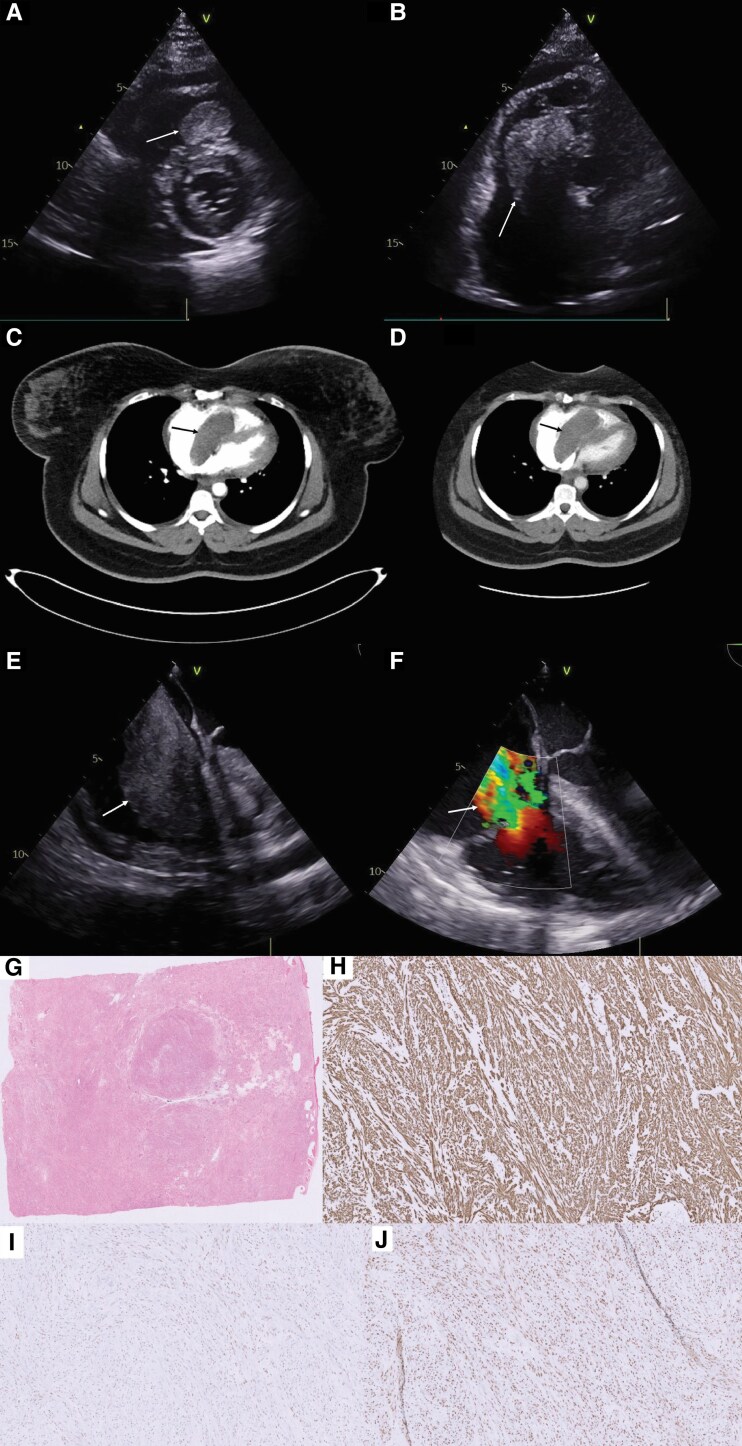 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Cardiac Structural Anomalies and Repair · Cardiovascular Effects of Exercise
A 34-year-old female with a history of hysterectomy for uterine fibroid with intravascular leiomyomatosis in 2019 presented with acute breathlessness (NYHA class IV) and ankle swelling. Clinical examination revealed raised jugular venous pressure and oedema of both lower limbs. Laboratory tests showed a negative D-dimer with elevated BNP of 1416. Chest radiography did not demonstrate any signs of lung congestion. Transthoracic echocardiogram revealed a large right-sided cardiac mass extending from the right atrium to the right ventricle across the tricuspid valve and circumferential pericardial effusion (Figure 1A and B). Due to the acute presentation, computed tomography of thorax, abdomen, and pelvis (CT-TAP) was performed, which revealed a 77 mm × 37 mm × 26 mm mass (Figure 1C and D), with no evidence of other organ involvement, residual or recurrent pelvic tumour. Following surgical review, the decision was made to operate, given the obstructive nature of the mass and the rapid progression of symptoms. The patient underwent excision of the mass with replacement of tricuspid valve with a bioprosthetic valve, due to severe tricuspid regurgitation after the mass excision (Figure 1F). The patient had an uneventful postoperative course and was discharged home after one week. During three- and six-month follow-up, the patient was asymptomatic. There was no evidence of residual mass in a two-month follow-up cardiac magnetic resonance imaging.
Histopathological examination confirmed the diagnosis of leiomyoma, with the presence of oestrogen and progesterone receptors (Figure 1G–J). Multidisciplinary team discussion advised that the most probable diagnosis is a benign metastasizing leiomyoma (BML), given the rare incidence of primary cardiac leiomyomas and the history of intravascular leiomyomatosis. They advised to start hormonal therapy, to reduce the future recurrence of leiomyoma.
Resection of secondary cardiac tumours has been reported in the literature in situations where it poses haemodynamic compromise.^1^ Hormonal therapy is effective in reducing the recurrence of hormone-receptor positive BML but requires long-term adherence.^2^ In a published meta-analysis looking into 2277 patients who underwent tricuspid valve replacement with mechanical and bioprosthetic valves, there was no significant difference between the two groups in mortality, need for re-operation, and 5-year valve failure (see Supplementary material online, Videos S1–S3).^3^
Supplementary Material
ytaf102_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tyebally S, Chen D, Bhattacharyya S, Mughrabi A, Hussain Z, Manisty C, et al Cardiac tumors: JACC cardiooncology state-of-the-art review. JACC Cardio Oncol 2020;2:293–311.34396236 10.1016/j.jaccao.2020.05.009PMC 8352246 · doi ↗ · pubmed ↗
- 2Fu Y, Li H, Tian B, Hu B. Pulmonary benign metastasizing leiomyoma: a case report and review of the literature. World J Surg Oncol 2012;10:268.23234399 10.1186/1477-7819-10-268PMC 3545911 · doi ↗ · pubmed ↗
- 3Negm S, Arafat AA, Elatafy EE, Fawzy HF. Mechanical versus bioprosthetic valve replacement in the tricuspid valve position: a systematic review and meta-analysis. Heart Lung Circ 2021;30:362–371.33229238 10.1016/j.hlc.2020.03.011 · doi ↗ · pubmed ↗