Reduction of Antibiotic Prescription in Complicated Appendicitis through Behavioral Change Measures
Alberto A. Artiles Garcia, Humberto Guanche Garcell, Miguel J. Pinto Echevarría, Carlos A. Sanchez Portela, Carlos M. Sanchez Rivas, Marlon Arias Medina, Niuvis Seoane Perez, Osiris I. Escobar More, Tania M. Fernandez Hernandez

TL;DR
This study shows that changing how antibiotics are prescribed for complicated appendicitis can reduce usage and costs without harming patients.
Contribution
The study demonstrates a successful behavioral intervention to reduce antibiotic use in complicated appendicitis treatment.
Findings
A 29.5% reduction in antibiotic treatment duration was observed during the second intervention period.
Antibiotic consumption and costs decreased by 38.7% and 24.6%, respectively, with no adverse patient outcomes.
The intervention improved healthcare efficiency and helped prevent microbial resistance.
Abstract
Background Variability in the prescription of antibiotics constitutes an area for improvement related to patient safety issues, including the risk of infection and health care efficiency based on evidence. Objectives The study aims to evaluate the effect of an intervention to reduce the duration of antibiotic treatment in complicated appendicitis. Methods A quality improvement program was implemented in the surgical department of The Cuban Hospital (Doha, Qatar). During a 3-month baseline period, data about antibiotic duration, consumption (daily defined doses), and cost (in Qatary Riyals) were identified, as well as during two plan-do-study-act (PDSA) intervention periods. Interventions include action focused on staff education, monitoring antibiotic use, feedback, and reminders during discharge planning. Results At baseline, 13 patients with complicated appendicitis were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
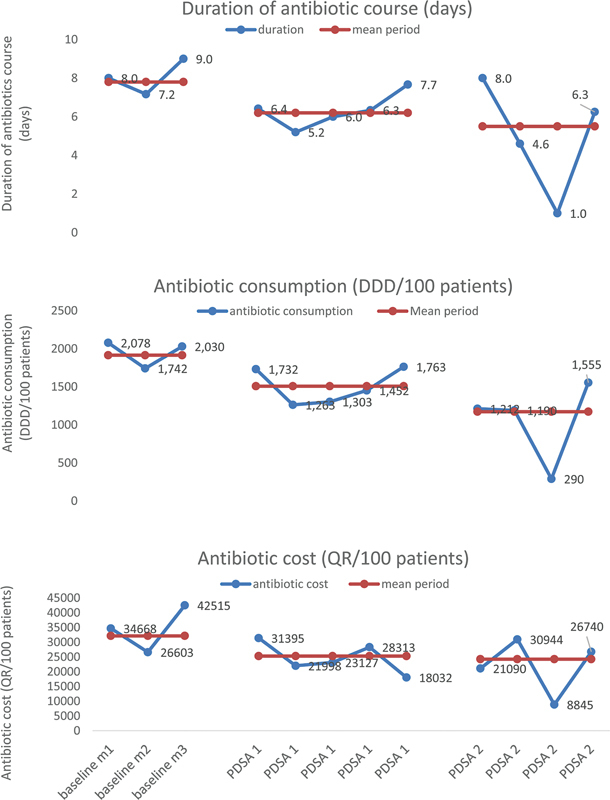 Fig. 1
Fig. 1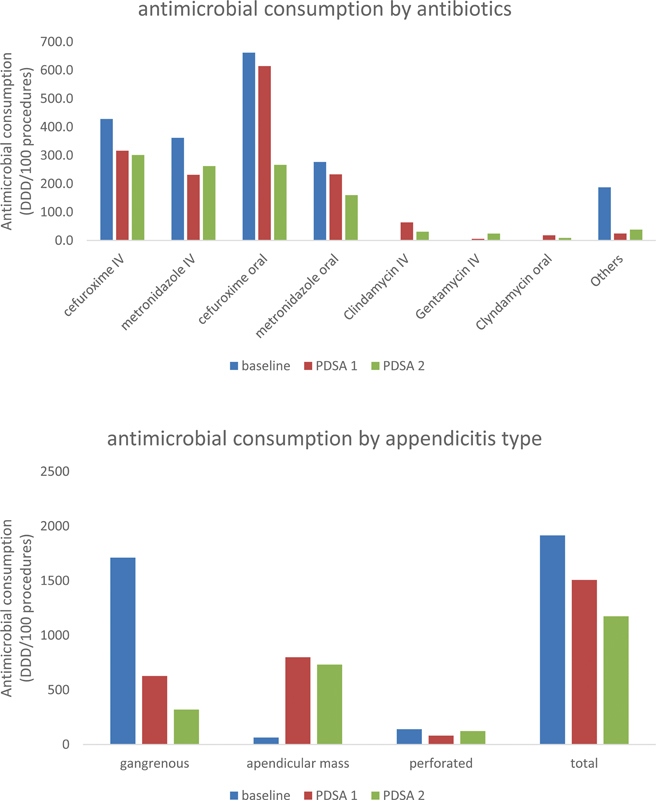 Fig. 2
Fig. 2| PDSA cycle 1 | PDSA cycle 2 | ||
|---|---|---|---|
| Time | April–August 2023 | September–December 2023 | |
| Plan | 1. To review and evaluate with the surgical team, the current recommendations of antibiotic prophylaxis based on international guidelines and corporate policies | 1. To conduct a detailed analysis of prolonged antibiotic prescriptions done patient by patient based on the supporting evidence | |
| Do | 1. Review the appropriateness of prescription during morning team meetings and at discharge | 1. Daily review of antibiotic prescription at discharge by the surgical team | |
| Study | |||
| Act | - Reduction in duration of antibiotic prescription | - Improved prescription practices | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAppendicitis Diagnosis and Management · Intraperitoneal and Appendiceal Malignancies · Meta-analysis and systematic reviews
Introduction
Variability in health care practices is frequently observed and is sometimes associated with failures in compliance with evidence-based recommendations. When this is linked to unnecessary or excessive antibiotics use for the management of selected clinical conditions, it has additional implications that include adverse effects (e.g., Clostridium difficile infections), the development of antimicrobial resistance, and increased cost among others. 1 2
In complicated appendicitis, antibiotics are required after the surgical procedure, and various studies described proper outcomes with short duration of antibiotics treatment in complicated appendicitis. 3 4 The recent guidelines of the World Society of Emergency Surgery recommend limiting antibiotics use to 3 to 5 days if adequate source control is achieved. 5
During 2022, we conducted a quality improvement (QI) intervention to improve antibiotic prophylaxis in various surgical procedures and observed a significant variability of antibiotic treatment in complicated appendicitis. 6 Patients with an intraoperative diagnosis of gangrenous, perforated, or appendicular mass received, in addition to the surgical prophylaxis, up to 11 days of antibiotics mainly cefuroxime plus metronidazole as per hospital policy.
Accordingly, from the previous findings, we decide to develop a QI intervention to reduce the duration of the antibiotic course in complicated appendicitis by 25% from baseline by December 2023.
Materials and Methods
A QI program was implemented in the surgical department of The Cuban Hospital, a community hospital member of Hamad Medical Corporation (Doha, Qatar). The project was approved by the Quality and Patient Safety Department and recorded in Life QI ( https:/lifeqisystem.com ).
The QI project team includes members of the surgical team, pharmacy, and infection control department. The Corporate Policy CL 7197 on antimicrobial prescribing recommends the use of cefuroxime plus metronidazole for surgical prophylaxis.
Complicated appendicitis includes the appendicular mass, gangrenous, and perforated according to surgeon's assessment during the surgical procedures (most performed through laparoscopic methods). Baseline data collection was conducted over a 3-month period including days on antibiotics (during admission plus after discharge), antibiotic consumption using Defined Daily Dose (DDD)/Anatomical Therapeutic Chemical (ATC) system (ATC/DDD), and antibiotic cost (as per hospital prices in Qatari Riyals [QR]). No action for improvement was implemented during baseline including staff feedback.
Intervention
The baseline period includes 13 patients with complicated appendectomies during January to March 2023. After the baseline data collection from the patients' electronic medical records, the surgical team and key leaders were informed about the summary of baseline data to support further actions focused on staff education, monitoring antimicrobial use, and feedback to staff.
Two plan-do-study-act (PDSA) cycles were conducted ( Table 1 ). The first PDSA cycle (April–August 2023, 41 patients) includes a dedicated session review with the surgical team of the current recommendation for antibiotic prophylaxis and treatment of complicated appendicitis. The monitoring of antibiotic prescription duration was performed weekly and the staff was informed through a progress report distributed by email, and open analysis during morning meetings was done. During the second PDSA cycle (September–December 2023, 15 patients), additional data analysis of patients with prolonged antibiotic use was performed including its rationality based on evidence. The close monitoring of antibiotic duration and timely feedback to staff were implemented including the analysis during the discharge planning. The discharge planning is performed usually the day before discharge and includes communication with the patient, the review of the postdischarge management, and patient and family educational needs.
The Revised Standards for Quality Improvement Reporting Excellence (version 2.0) were followed in this QI project.
Analysis of data was performed using descriptive statistics. The antimicrobial consumption and cost were presented as DDD and QR per 100 patients, respectively.
Results
At baseline, 13 patients were documented with complicated appendicitis (13/70 appendectomies, 18.6%), while 41 (41/175 appendectomies, 23.4%) and 15 patients (15/108 appendectomies, 13.9%) during PDSA cycles 1 and 2, respectively. Appendicular mass was reported in 36 patients, gangrenous appendicitis in 30 patients, and perforated appendicitis in 3 patients.
The mean duration of antibiotic treatment was 7.8 days at baseline, and 6.2 and 5.5 days during PDSA cycles 1 and 2, with a 29.5% reduction during the intervention, achieving the QI project goal. The mean antimicrobial consumption was 1,915 DDD/100 patients at baseline and 1,508 and 1,173 DDD/100 patients during PDSA cycles 1 and 2 with a 38.7% reduction. The antimicrobial cost was 32,153 QR/100 patients at baseline, and 25,285 and 24,249 QR/100 patients during PDSA cycles 1 and 2 with a 24.6% reduction ( Fig. 1 ).
Duration of antibiotic course, antibiotic consumption, and cost in complicated appendicitis (days) during baseline and intervention period. DDD, Daily Defined Dose; QR, Qatari riyals.
The reduction of duration (23%) and antimicrobial consumption (40.4%) was mainly in patients with gangrenous or perforated appendicitis, while the cost reduction was higher in appendicular mass (30.1%) ( Fig. 2 ). The combination of cefuroxime–metronidazole was more than 90% of antibiotic consumption during baseline and PDSA cycle 1, and in PDSA cycle 2, this was reduced to 84% due to its limited availability and the use of alternative prophylaxis (gentamycin plus clindamycin). Therefore, the combination of cefuroxime–metronidazole contributes with 93, 87, and 85% of the cost during the baseline and PDSA cycles 1 and 2, respectively ( Fig. 2 ). The mean duration of inpatient treatment was 2.8 days and after discharge was 4.3 days by switching from intravenous to oral route.
Antimicrobial consumption by antibiotic type and appendicitis type according to periods (DDD/100 procedures). DDD, Daily Defined Dose; IV, intravenous; PDSA, plan-do-study-act.
All patients were followed up 30 days after the procedure date and no complication was detected including surgical site infections.
Discussion
The study has shown the reduction of antibiotic treatment after complicated appendicitis by an intervention focused on increasing the staff's awareness about the need for the rational use of antibiotics based on the best evidence available. 5 7
Regardless of the observed reduction in antibiotic use, we consider potential additional reduction could be achieved, in gangrenous or perforated appendicitis, mainly in patients with limited evidence of disseminated or severe abdominal infection observed during the surgical procedure.
Laverde et al, in a cohort study, reported that an extended duration of antibiotic treatment was not associated with a reduced risk of developing surgical infection after appendectomy. 8 Other studies report similar findings in adults and pediatric patients. 9 10
While the ATC/DDD system is valuable for monitoring antibiotic consumption and its impact on health care efficiency, the guidelines recommend the maximum duration of treatment in complicated appendicitis. 5 11 The Access, Watch, Reserve (AWaRe) guideline indicates that in complicated appendicitis, antibiotic therapy can be continued for 5 days if the symptoms have resolved and the source of the infection has been eliminated with surgery. 11
Actions to promote behavioral change in prescription practices have demonstrated the improvement in antibiotic practices in appendicitis and other clinical conditions. 12 13 In addition to the education, monitoring, and feedback to staff, reminders during the discharge planning could be important. The discharge planning is a key moment to review the prescription practices and identify the required postdischarge antibiotics.
The most significant challenge is the sustainability of the practices in health care settings with frequent staff renewal. Then, long-term sustainability requires continuous staff education, up-to-date antimicrobial policy based on the best evidence about the duration of antibiotic treatment in complicated appendicitis, and monitoring and feedback to staff.
Study limitation : In a single-center experience with a low volume of surgical procedures, implementing QI initiatives could be easier, and staff communication could be more expedited.
Conclusion
The QI intervention resulted in a reduction in the duration of antibiotic treatment in patients with complicated appendicitis, with satisfactory patient outcomes. Additionally, the reduction in consumption and costs of antimicrobial use impacted the efficiency of health care and the prevention of microbial resistance and other adverse effects.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Antimicrobial Resistance Collaborators Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis Lancet 2022399(10325):62965535065702 10.1016/S 0140-6736(21)02724-0PMC 8841637 · doi ↗ · pubmed ↗
- 2Pulingam T Parumasivam T Gazzali A M Antimicrobial resistance: prevalence, economic burden, mechanisms of resistance and strategies to overcome Eur J Pharm Sci 202217010610334936936 10.1016/j.ejps.2021.106103 · doi ↗ · pubmed ↗
- 3Ramson D M Gao H Penny-Dimri J C Duration of post-operative antibiotic treatment in acute complicated appendicitis: systematic review and meta-analysis ANZ J Surg 202191(7-8):1397140433576567 10.1111/ans.16615 · doi ↗ · pubmed ↗
- 4David A Dodgion C Zein Eddine S B Davila D Webb T P Trevino C M Perforated appendicitis: short duration antibiotics are noninferior to traditional long duration antibiotics Surgery 20201670247547731587914 10.1016/j.surg.2019.08.007 · doi ↗ · pubmed ↗
- 5Di Saverio S Podda M De Simone B Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines World J Emerg Surg 202015012732295644 10.1186/s 13017-020-00306-3PMC 7386163 · doi ↗ · pubmed ↗
- 6Guanche Garcell H Aragón Palmero F J Marquez Reyna D AA quality improvement intervention on surgical prophylaxis impact in antibiotic consumption and cost in selected surgical procedures J Healthc Qual Res 2024390425826538616433 10.1016/j.jhqr.2024.03.003 · doi ↗ · pubmed ↗
- 7Lamm R Kumar S S Collings A T Diagnosis and treatment of appendicitis: systematic review and meta-analysis Surg Endosc 202337128933899037914953 10.1007/s 00464-023-10456-5 · doi ↗ · pubmed ↗
- 8Laverde B LB Maak M Langheinrich M Antibiotic treatment after appendectomy for acute complicated appendicitis to prevent intrabdominal abscess and wound infections Langenbecks Arch Surg 20244090118038850459 10.1007/s 00423-024-03367-z PMC 11162365 · doi ↗ · pubmed ↗