Clearing the Path: Redefining Hepatolithiasis Removal Through Endoscopic Hepaticogastrostomy
Woo Suk Kim, Tasur Seen, Krishna Gurram

TL;DR
A new endoscopic method is proposed for removing bile stones in the liver, offering a less invasive alternative to surgery.
Contribution
The paper presents a successful case of using EUS-guided hepaticogastrostomy for hepatolithiasis treatment.
Findings
Endoscopic ultrasound-guided hepaticogastrostomy successfully cleared stones in a patient with recurrent hepatolithiasis.
The procedure provided complete symptomatic relief and no recurrence during follow-up.
This approach serves both diagnostic and therapeutic purposes with less invasiveness than traditional methods.
Abstract
Hepatolithiasis is a condition characterized by the presence of bile stones in the intrahepatic bile ducts. It represents a significant therapeutic challenge owing to its association with recurrent cholangitis, biliary obstruction, and potentially life-threatening complications such as hepatic abscesses and cholangiocarcinoma. Traditional treatments include hepatectomy and percutaneous transhepatic cholangioscopic lithotomy (PTCL), both of which are effective but highly invasive, whereas endoscopic approaches often leave residual stones. We report a case of recurrent hepatolithiasis with abscesses in an 80-year-old woman who had failed to respond to conventional endoscopic approaches. Endoscopic ultrasound (EUS)-guided hepaticogastrostomy was successfully performed through the transgastric approach to allow access to intrahepatic stones for clearance with complete symptomatic relief and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
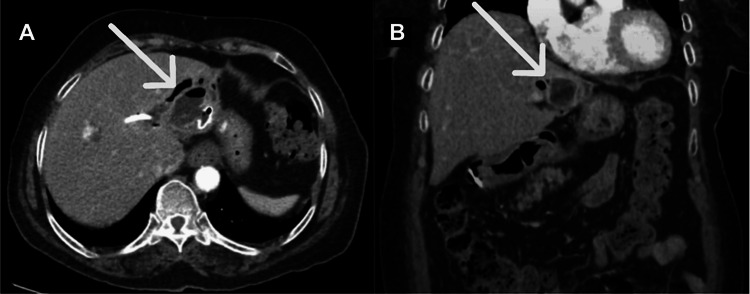 Figure 1
Figure 1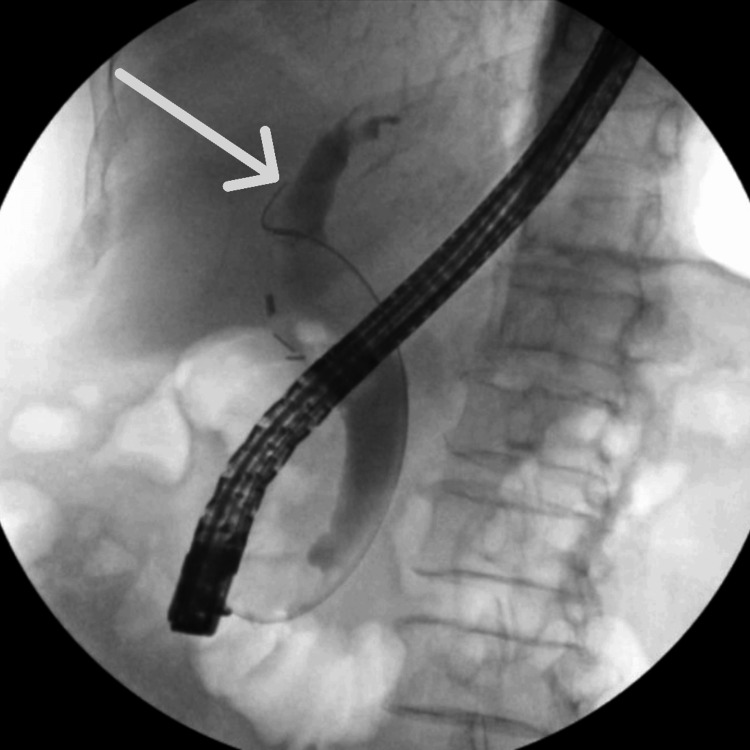 Figure 2
Figure 2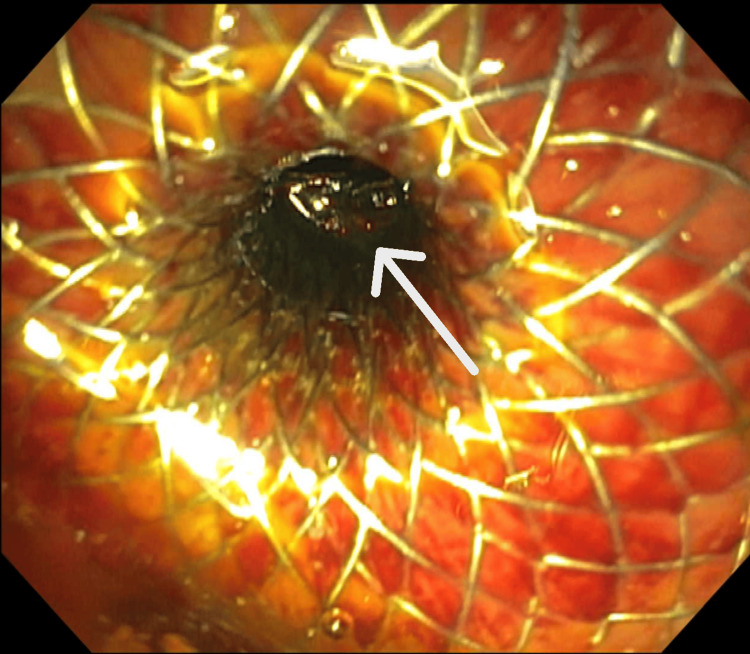 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pancreatic and Hepatic Oncology Research · Esophageal and GI Pathology
Introduction
Hepatolithiasis represents the presence of bile stones in the intrahepatic bile ducts proximal to the confluence of the hepatic ducts. It is considered a significant cause of recurrent cholangitis and biliary obstruction [1]. This condition is predominantly found in East Asia, with incidence rates between 2% and 25% in Asian countries compared to approximately 1% in the West [2]. The disease has been associated with low socioeconomic class due to a diet mainly consisting of high carbohydrates, low protein, and low fat. However, incidence rates in East Asia have been decreasing with the improvement in nutrition and the Westernization of diet and public health policies. On the other hand, the disease is rare in the West, and it most often presents as secondary hepatolithiasis associated with underlying conditions causing strictures of the bile ducts or stasis of bile, such as primary sclerosing cholangitis, benign post-surgical strictures, malignancy, or choledochal cysts [3]. Nevertheless, incidence rates in the West have been increasing with migration and advancements in diagnostic capabilities [4].
Clinically, hepatolithiasis usually presents with the triad of right upper quadrant abdominal pain, fever, and jaundice, with further complications such as intrahepatic abscesses, biliary strictures, and increased risk for cholangiocarcinoma [5]. Diagnosis is established through a combination of laboratory and imaging findings. Laboratory tests often yield leukocytosis with neutrophil predominance and elevated liver function tests, including alkaline phosphatase and bilirubin, suggesting an obstructive pattern. Imaging studies such as ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI) can show intrahepatic or extrahepatic ductal dilation with stones, focal strictures, and segmental hepatic atrophy [6].
Treatments traditionally have relied on surgical approaches, such as hepatectomy and percutaneous transhepatic cholangioscopic lithotomy (PTCL). Endoscopic intervention has been limited to the direct visualization of stones and bile drainage through stent or balloon dilation [7,8]. These methods have often resulted in residual stones that act as a nidus for recurrent infections, with an incidence rate of 29.6% even after surgery [9].
Due to the high recurrence rate despite invasive surgeries and the rising incidence rate in the West, there is an urgent need for more effective and minimally invasive alternatives for the treatment of hepatolithiasis. To overcome these limitations in the current management, we propose a novel endoscopic approach for direct removal of hepatolithiasis by hepaticogastrostomy. This provides a less invasive alternative with improved patient outcomes and reduced recurrence, further expanding the role of endoscopy in this complex condition.
Case presentation
An 80-year-old woman was brought to the emergency department with recurrent right upper quadrant abdominal pain and fever. She had a surgical history of cholecystectomy, complicated by left intrahepatic biliary stricture and resultant hepatolithiasis, which were previously treated with endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy and transpapillary common bile duct stent placement. However, computed tomography (CT) of the abdomen now showed multiple hepatic abscesses due to hepatolithiasis (Figure 1). The patient was treated with percutaneous drainage and antibiotics and then discharged home with a plan to repeat ERCP.
Axial (A) and coronal (B) computed tomography scans of the abdomen showing liver abscesses due to hepatolithiasis (arrows)
Two months later, the patient presented again with persistent fevers. A repeat ERCP confirmed a retained hepatolithiasis as the likely nidus for recurrent infections, and the intrahepatic duct stent was replaced. Despite the intervention, the patient continued to have symptoms; therefore, the decision was made to proceed with the direct endoscopic removal of the hepatolithiasis via hepaticogastrostomy.
The left intrahepatic bile duct was punctured using a 19-gauge needle under endosonographic guidance via a transgastric approach. The bile duct was injected with contrast, and a cholangiogram was obtained to confirm that contrast extended to the left intrahepatic bile duct (Figure 2). A 10 x 10 mm covered lumen-apposing metal stent was chosen due to the low risk of stent migration, reduced risk of leakage into the peritoneum, and large lumen diameter to ensure complete drainage of multiple hepatolithiasis [10]. It was deployed in a transgastric fashion into the left intrahepatic bile duct and dilated with a 10 mm balloon. Several stones were directly visualized and extracted by a basket (Figure 3). Due to the high stone burden, the remaining stones were left to be passively cleared through the stent. A wire was passed under direct visualization into the left intrahepatic duct, and a double pigtail stent was placed as an anchoring stent at the intrahepatic biliary ducts and the stomach. The patient returned for stent removal in two months following the successful hepaticogastrostomy with no further hepatolithiasis and resolution of her symptoms.
Cholangiogram showing contrast extending to the left intrahepatic bile duct (arrow)
A 10 x 10 mm stent deployed in a transgastric fashion into the left intrahepatic bile duct with visualized hepatolithiasis (arrow)
Discussion
Hepatolithiasis remains a significant therapeutic challenge due to the ineffective removal of stones and its association with serious complications involving recurrent infections, hepatic abscesses, biliary strictures, and cholangiocarcinoma [1]. Although surgical approaches using hepatectomy and PTCL can offer relief in localized disease, these options are invasive and carry high risks, particularly in elderly patients with multiple comorbidities [7]. Endoscopic interventions have been largely limited to stent placement and balloon dilation, which rarely address the underlying cause and result in residual stones that act as a nidus for infection [8]. ERCP with electro-hydraulic lithotripsy (EHL) or laser lithotripsy has been demonstrated as effective, with a meta-analysis reporting an overall stone clearance rate of 88% and a recurrence rate of 13% [11]. Despite its potential, this approach has been primarily studied in patients with low stone burden and, therefore, was deferred in our patient due to the concern for extended procedural time given her multiple hepatolithiasis and comorbidities.
This case illustrates the limitation of traditional endoscopic management of hepatolithiasis and introduces a novel approach using hepaticogastrostomy for direct stone removal. Endoscopic ultrasound (EUS)-guided hepaticogastrostomy allows for precise access to the intrahepatic bile ducts with a technical success rate of 98% and a complication rate of 15-20%, including pneumoperitoneum, bilioperitoneum, infection, and stent dysfunction [12]. To minimize the risk of bile leakage, a covered stent was used in our patient. Although hepaticogastrostomy is indicated in the management of bile drainage for malignant biliary obstruction or complex benign strictures, this approach is a novel alternative for hepatolithiasis, allowing diagnostic and therapeutic intervention in a single session. Moreover, the procedural success in this elderly patient underlines the potential of this intervention as a viable alternative to invasive surgeries, especially for patients who are not optimal candidates for surgery.
Conclusions
Hepaticogastrostomy offers a less aggressive alternative in the treatment of hepatolithiasis compared to traditional surgeries and a safer approach for high stone burden compared to more recent endoscopic advancements such as ERCP with EHL. This novel technique represents a promising advance by enabling precise localization and direct clearance of retained stones. Further studies should aim to develop standardized protocols, validate its safety and effectiveness within a greater series of cases, and define the role of hepaticogastrostomy within the overall context of hepatolithiasis management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Classification and management of hepatolithiasis: a high-volume, single-center's experience Intractable Rare Dis Res Feng X Zheng S Xia F Ma K Wang S Bie P Dong J 151156120122534308910.5582/irdr.2012.v 1.4.151PMC 4204570 · doi ↗ · pubmed ↗
- 2Hepatolithiasis: clinical series, review and current management strategy Turk J Surg Dilek ON Atasever A Acar N 3823923620203377839810.47717/turkjsurg.2020.4551 PMC 7963303 · doi ↗ · pubmed ↗
- 3Recurrent pyogenic cholangitis with hepatolithiasis-the role of surgical therapy in North America J Gastrointest Surg Al-Sukhni W Gallinger S Pratzer A 4965031220081799912110.1007/s 11605-007-0398-2 · doi ↗ · pubmed ↗
- 4Primary hepatolithiasis, recurrent pyogenic cholangitis, and oriental cholangiohepatitis: a tale of 3 countries Adv Anat Pathol Tsui WM Lam PW Lee WK Chan YK 3183281820112165436310.1097/PAP.0b 013e 318220 fb 75 · doi ↗ · pubmed ↗
- 5Surgical management of hepatolithiasis HPB (Oxford) Sakpal SV Babel N Chamberlain RS 1942021120091959064710.1111/j.1477-2574.2009.00046.x PMC 2697895 · doi ↗ · pubmed ↗
- 6Hepatolithiasis and biliary parasites Baill Clin Gastroenterol Leung JW Yu AS 68170611199710.1016/s 0950-3528(97)90016-69512805 · doi ↗ · pubmed ↗
- 7Indication and procedure for treatment of hepatolithiasis Arch Surg Uchiyama K Onishi H Tani M Kinoshita H Ueno M Yamaue H 14915313720021182295010.1001/archsurg.137.2.149 · doi ↗ · pubmed ↗
- 8Balloon endoscopy-assisted endoscopic retrograde cholangiopancreatography for hepatolithiasis in patients with hepaticojejunostomy Surg Endosc Hakuta R Sato T Nakai Y 242324323820243845374810.1007/s 00464-024-10738-6PMC 11078785 · doi ↗ · pubmed ↗