Liquid silicone gel injection leading to primary squamous cell carcinoma of the breast
Hidenobu Takahashi, Yen‐Shuo Huang, Chee‐Yin Chai, Jung‐Yu Kan

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
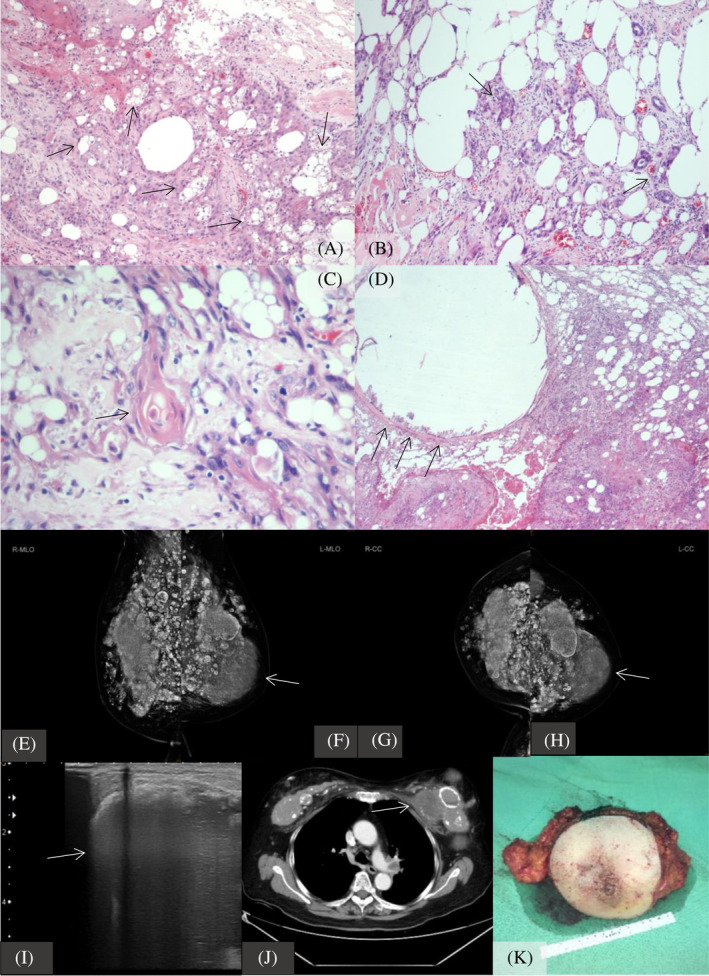 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Cancer Treatment Studies · Breast Lesions and Carcinomas · Breast Implant and Reconstruction
Primary squamous cell carcinoma (SqCC) of the breast, which represents <0.1% of all breast cancers, is rare and diagnostically challenging, possibly having high mortality due to its large size, distant metastasis, and rapid progression. Bagged silicone possibly induces primary breast SqCC. Liquid silicone gel was replaced with bagged silicone breast implants; however, this was warned about by the FDA on March 8, 2023.
This case details primary SqCC of the breast in an 81‐year‐old postmenopausal Asian woman with a history of bilateral liquid silicone gel injections in her 20s. She exhibited local heat, swelling, and mild erythema in the left breast. Chest computed tomography (CT) showed a 10.3 cm left breast tumor with lymph node and bilateral lung metastases, significant calcifications around the silicone injection sites, and pathological findings of squamous cell carcinoma with keratinization. (Figure 1) Tumor markers revealed elevated serum SqCC antigen at 28.0 ng/mL, with normal CEA and CA15‐3 levels. Treatment included a left modified radical mastectomy and sentinel lymph node biopsy, with negative estrogen receptor, progesterone receptor, human epidermal growth factor receptor 2, and GATA Binding Protein 3, and a Ki‐67 index of 15%.
Primary SqCC of the breast, representing less than 0.1% of all breast cancers, is rare and diagnostically challenging. The 2003 WHO classification mandates three criteria for diagnosing breast SqCC: (1) Exclusive presence of SqCC without other neoplastic changes, (2) Absence of SqCC at any other primary site, and (3) No overlying skin or nipple involvement.
Literature indicates that early‐stage breast SqCC typically has a favorable prognosis, yet lacks specific diagnostic and management guidelines.1 These tumors are often hormone and HER2 receptor negative, as seen in our case.2 Our case, with the largest reported primary breast SqCC (10.3 cm), underscores the lack of standardized treatment protocols. Despite the absence of formal guidelines, our patient underwent surgical treatment without subsequent chemotherapy, radiation, or hormone therapy. However, Aparicio et al. reported no survival advantage for SqCC patients receiving neoadjuvant or adjuvant chemotherapy, in comparison to those who did not receive chemotherapy, highlighting the need for tailored treatment strategies.3
However, silicone gel injections, once popular in Taiwan, have been associated with complications like mastitis, sarcoma, and systemic issues such as autoimmune/inflammatory syndrome induced by adjuvants (ASIA) also called human adjuvant disease (HAD) indicate liquid silicone dissemination may lead chronic inflammatory status due to silicone spread.4 Our case reveals long‐term risks including significant calcification and chronic inflammation surrounding the injected silicone gel parcels on CT scans, which induces squamous cell metaplasia in future (Figure 1). This case supports the notion that breast SqCC can occur following silicone injections. Microscopically, the breast tissue was infiltrated by invasive carcinoma with squamous differentiation, exhibiting varying degrees of nuclear atypia and prominent keratinization. These neoplastic cells were interspersed with numerous vacuolated cavities and empty spaces of different sizes. In the surrounding mammary tissue, an exuberant foreign body reaction was observed, characterized by the presence of multinucleated giant cells and lymphocytic infiltration. Based on the patient's clinical history and the morphological findings, it is suggested that the occurrence of squamous cell carcinoma in the breast is associated with the silicone injection (Figure 1).5
This report highlights a case of SqCC linked to silicone gel injections and the largest SqCC currently reported; however, the latent population numbers who received silicone gel injection was unclear, when the injection was popular in Taiwan, the part of population may had received silicone gel injection by non‐authorized medical professional, thus not officially recorded. Owing to the benign appearance on mammograms and ultrasounds, individuals who received silicone gel injections may require additional screening methods such as SqCC tumor marker assessment and magnetic resonance imaging/CT studies and guided biopsy to suspicious lesion.
In conclusion, this case of primary breast SqCC following silicone gel injection emphasizes the urgent need for research on the link between silicone gel, implants, and SqCC development in the breast. This highlights the carcinogenic risk associated with liquid silicone gel injections, as evidenced by the high occurrence of SqCC. This case report responds to a recent FDA warning and emphasizes the need for heightened awareness and screening of individuals with past silicone gel injections.
CONFLICT OF INTEREST STATEMENT
All authors declare no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhang X , Zhang B , Zang F , Zhao L , Yuan Z , Wang P . Clinical features and treatment of squamous cell carcinoma of the breast. Onco Targets Ther. 2016;9:3181–3185.27313463 10.2147/OTT.S 95128 PMC 4892827 · doi ↗ · pubmed ↗
- 2Hennessy BT , Krishnamurthy S , Giordano S , Buchholz TA , Kau SW , Duan Z , et al. Squamous cell carcinoma of the breast. J Clin Oncol. 2005;23(31):7827–7835.16258085 10.1200/JCO.2004.00.9589 · doi ↗ · pubmed ↗
- 3Aparicio I , Martinez A , Hernandez G , Hardisson D , De Santiago J . Squamous cell carcinoma of the breast. Eur J Obstet Gynecol Reprod Biol. 2008;137(2):222–226.17481802 10.1016/j.ejogrb.2007.03.021 · doi ↗ · pubmed ↗
- 4Cohen Tervaert JW , Mohazab N , Redmond D , van Eeden C , Osman M . Breast implant illness: scientific evidence of its existence. Expert Rev Clin Immunol. 2022;18(1):15–29.34882509 10.1080/1744666 X.2022.2010546 · doi ↗ · pubmed ↗
- 5Toyonaka R , Ozeki J , Koyama Y , Takahashi S , Tang X , Kobayashi H , et al. A case of breast squamous cell carcinoma following breast augmentation with liquid silicone injection after 16 years. Surg Case Rep. 2022;8(1):22.35089470 10.1186/s 40792-022-01378-w PMC 8799800 · doi ↗ · pubmed ↗