An unusual case of mesenteric fibromatosis
Yu‐Cheng Chiang, Po‐Hsuan Wu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
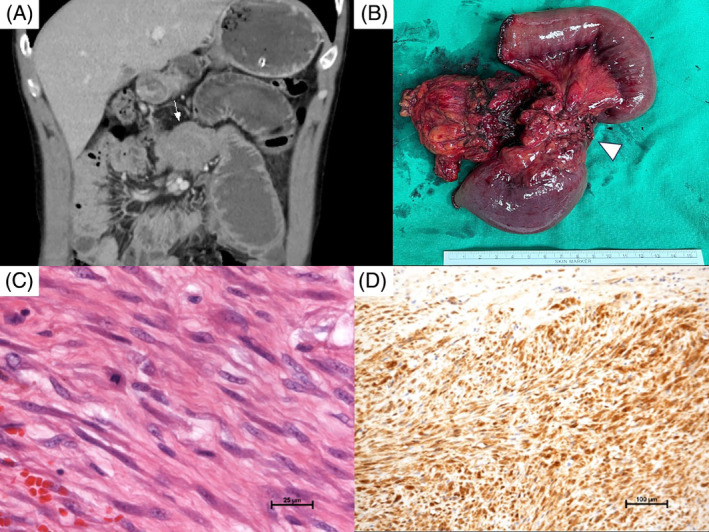 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSoft tissue tumor case studies · Vascular Malformations and Hemangiomas · Oral and Maxillofacial Pathology
A 35‐year‐old male presented at our emergency department with a 2‐week history of abdominal fullness, pain, and vomiting. He had no underlying health conditions, previous surgeries, or familial cancer history. Physical examination and lab tests in the emergency room were unremarkable, revealing no palpable abdominal mass. However, an abdominal computed tomography (CT) scan showed a 7.5 × 5.2 cm mesenteric soft tissue mass, suggestive of a gastrointestinal stromal tumor (GIST) involving the small bowel, likely causing mechanical ileus (Figure 1A, arrow). During laparotomy, a 7.5 × 4.5 × 3.5 cm mass was found in the mesentery of the jejunum, attached to the jejunum and T‐colon. Resection of the mesenteric tumor (Figure 1B, arrowhead), along with a segment of the jejunum and a segment of the transverse colon, was successfully performed, followed by end‐to‐end anastomosis of the jejunum and T‐colon separately. Microscopic examination revealed spindle and stellate cells exhibiting vesicular nuclei with small nucleoli (Figure 1C). Immunohistochemistry showed that the tumor cells were positive for β‐catenin and exhibited focal expression of SMA, desmin, and H‐caldesmon, while being negative for S‐100, DOG‐1, and CD117. These characteristics are typical of intra‐abdominal mesenteric fibromatosis (MF) (Figure 1D).
Desmoid‐type fibromatosis (DTF) is a rare tumor, constituting only 0.03% of all neoplasms,1, 2 predominantly affecting individuals in their 30s and 40s, with a female‐to‐male ratio of 2:1.1 Desmoid fibromatosis can develop in various body parts, typically involving the limbs, abdominal wall, and less frequently, the abdominal cavity, especially the mesentery. Patients with DTF may initially be asymptomatic, but as the tumor enlarges, it can press on nearby organs, leading to complications like intestinal obstruction, ischemia, and bleeding.3, 4 The etiology of fibromatosis is unclear, but potential contributing factors include trauma, estrogen levels, genetic predisposition (e.g., familial adenomatous polyposis [FAP]), and autoimmune disorders like Crohn's disease.1 About 30% of sporadic DTF cases follow trauma, indicating that abnormal cell proliferation in wound healing. The incidence of DTF in FAP patients is around 1000 times higher than in the general population,4 with 5%–15% of DTF cases occurring in FAP individuals.2 Additionally, β‐catenin mutations are identified in 71%–91% of spontaneous DTF cases.2 Accurate diagnosis of MF is critical, as misdiagnosis can result in inappropriate treatment. Grossly, MF appears as solid, grayish, uniform masses, differing from the softer, variable GISTs.3, 5 On CT, MF is typically well‐defined and homogeneous, contrasting with the heterogeneous, often necrotic GISTs. On magnetic resonance imaging (MRI), MF mostly appears hypointense on T2‐weighted images.3, 5 Diagnosis relies on microscopic analysis and immunostaining, with β‐catenin expression being a key identifier.3, 5 Treatment for MF is debated due to its unpredictable nature. Observation is preferred for slow‐growing or regressing tumors,5 while surgery is the primary treatment for progressive, operable MF.2 Achieving microscopically negative for residual tumor (R0 surgical margins) is crucial for reducing recurrence rates.2 Aggressive surgery can lead to complications like short bowel syndrome. Radiotherapy is controversial due to radiation enteritis risks. For microscopically positive residual tumor (R1 resection), postoperative recurrence, or unresectable tumors, systemic treatments like chemotherapy, anti‐estrogenic therapy, and molecular‐targeted therapy are options. Despite available treatments, recurrence rates are high (24%–77%), necessitating regular monitoring through CT or MRI scans.3 In conclusion, mesenteric DTF is uncommon, marked by slow yet locally invasive growth. While symptoms like ileus are infrequent, they can occur, as demonstrated in our case. Surgical removal is the preferred initial treatment, yet the high rate of recurrence continues to be challenging.
CONFLICT OF INTEREST STATEMENT
All authors declare no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ji H , Zhu W , Zhao B , Shi J , Wei Q , Sun B , et al. A giant mesenteric fibromatosis involving the muscular layer of the colon wall: a case report. Medicine (Baltimore). 2019;98(1):e 14015.30608449 10.1097/MD.0000000000014015 PMC 6344171 · doi ↗ · pubmed ↗
- 2Sioda NA , Wakim AA , Wong T , Patel S , Coan K , Row D . A large sporadic intra‐abdominal desmoid‐type fibromatosis in a young male: a case report. Front Surg. 2020;7:60.33117845 10.3389/fsurg.2020.00060 PMC 7493805 · doi ↗ · pubmed ↗
- 3Mitrovic Jovanovic M , Djuric‐Stefanovic A , Velickovic D , Keramatollah E , Micev M , Jankovic A , et al. Aggressive fibromatosis of the right colon mimicking a gastrointestinal stromal tumour: a case report. J Int Med Res. 2021;49(3):300060521994927.33752489 10.1177/0300060521994927 PMC 7995451 · doi ↗ · pubmed ↗
- 4Zhang L , Zheng Y , Yu X , Yu K , Zhu S . Primary intra‐abdominal desmoid fibromatosis associated with familial adenomatous polyposis: a case report. Exp Ther Med. 2023;26(1):308.37273755 10.3892/etm.2023.12007 PMC 10236137 · doi ↗ · pubmed ↗
- 5Wronski M , Ziarkiewicz‐Wroblewska B , Slodkowski M , Cebulski W , Gornicka B , Krasnodebski IW . Mesenteric fibromatosis with intestinal involvement mimicking a gastrointestinal stromal tumour. Radiol Oncol. 2011;45(1):59–63.22933936 10.2478/v 10019-010-0051-7PMC 3423715 · doi ↗ · pubmed ↗