Takotsubo Cardiomyopathy: A Consequence of Blunt Chest Trauma
Aditya Lal Vallath, Michael Galuska, Taylor Campbell

TL;DR
An 84-year-old woman developed takotsubo cardiomyopathy after a car accident, showing it can be caused by physical trauma, not just emotional stress.
Contribution
This case expands the understanding of takotsubo cardiomyopathy by linking it to blunt chest trauma in an elderly patient.
Findings
Takotsubo cardiomyopathy occurred following blunt chest trauma in an elderly woman.
Coronary angiography ruled out coronary artery disease as a cause.
The case highlights the importance of considering takotsubo cardiomyopathy in trauma patients with cardiac dysfunction.
Abstract
Takotsubo cardiomyopathy (TTC), also known as stress-induced cardiomyopathy or "broken heart syndrome," is a transient form of myocardial dysfunction often triggered by emotional or physical stress. While typically associated with emotional distress and possible physical stress, TTC has rarely been reported in the context of physical trauma, including blunt chest injuries. This case report describes a novel instance of TTC in an 84-year-old woman who developed the condition following a motor vehicle accident, resulting in blunt chest trauma. Coronary artery disease was ruled out through coronary angiography, which showed no significant coronary obstruction. The patient’s left ventricular ejection fraction at presentation was 25-30%, indicative of severe systolic dysfunction. The patient's clinical course, diagnostic findings, and management are discussed, contributing to the literature…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
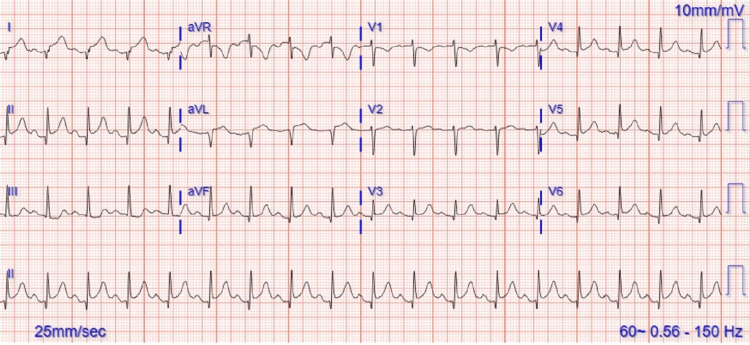 Figure 1
Figure 1| Initial findings on presentation | |
| Physical Exam | |
| Vitals | Temp: 37.1°C (98.7°F), HR: 106, Resp: 20, BP: 151/89, SpO2: 99% |
| Constitutional | Well appearing, no apparent distress |
| Eyes | Pupils equal, round, reactive to light, no conjunctival pallor |
| HENT | Mucous membranes moist, oropharynx unremarkable |
| Cardiovascular | Heart regular, no murmurs, good peripheral pulses |
| Pulmonary/Chest | Lungs clear, no wheezing, rales, or rhonchi, no respiratory distress |
| Abdominal | Soft, nontender, nondistended, normal bowel sounds, no guarding or rigidity, no pulsatile mass |
| Musculoskeletal | Left first MCP joint discomfort (no deformity), 4-inch subcutaneous hematoma on chest, no crepitus or JVD |
| Neurologic | AAOx3, no focal deficits, mild memory issues related to bruises |
| Skin | Superficial bruises on shins, no deformity or joint effusion, normal sensation and strength |
| Labs | |
| CBC | |
| WBC: 10.7 (3.10 - 8.50 10*3/uL) | |
| Hemoglobin: 14.5 (11.5 - 16.0 g/dL) | |
| Platelets: 241 (140 - 440 10*3/uL) | |
| Basic Metabolic Panel | Sodium: 135 (136 - 145 mmol/L) |
| CO2: 20 (22 - 29 mEq/L) | |
| Creatinine: 1.12 (0.60 - 1.10 mg/dL) | |
| eGFR: 49 (>60 mL/min) | |
| Glucose: 136 (83 - 110 mg/dL) | |
| Troponin I | Troponin I: 3.43 (0.00 - 0.05 ng/mL) |
| Coagulation Studies | APTT: 23 (23 - 35 seconds) |
| Protime: 9.9 (9.0 - 12.0 seconds) | |
| INR: 1.0 (normal) | |
| Type & Screen | ABO/Rh: A positive |
| Antibody Screen: Negative | |
| Radiology | |
| CT Chest | No acute injury to thorax, clear lungs, no pneumothorax or pleural effusion, no fracture, coronary artery calcification |
| CT Abdomen/Pelvis | No visceral or bony injury, multiple colonic diverticula, small fat-containing umbilical hernia, normal organs |
| X-ray | No evidence of fractures or dislocations noted |
| Category | Details |
| Vital Signs | |
| Temperature | 36.7°C (98.1°F) |
| Heart Rate | 101 bpm |
| Respiratory Rate | 18 bpm |
| Blood Pressure | 118/77 mmHg |
| SpO2 | 97% |
| Weight | 125 lbs (56.7 kg) |
| Pain Score | 4 (Moderate pain) |
| Body System | Findings |
| General | Well-appearing, no distress |
| Cardiovascular | Regular heart rhythm, no murmurs, good peripheral pulses |
| Pulmonary/Chest | Clear lungs bilaterally, bruising on left upper chest, tenderness on left anterior chest wall, no rib deformity or open wounds |
| Abdominal | Longitudinal bruising (seatbelt sign), no peritonitis, no hepatosplenomegaly |
| Musculoskeletal | No deformities, no pedal edema |
| Neurologic | Alert, oriented, no focal deficits |
| Skin | Warm, well-perfused, no acute rashes |
| Psychiatric | Normal affect |
| Laboratory Results | |
| Troponin I | 11,415 ng/L (high sensitivity) |
| Amylase | 123 U/L |
| CBC | WBC: 10.51 x 10^3 (3.10 - 8.50 x 10^3/uL) |
| Hemoglobin: 13.0 (11.5 - 16.0 g/dL) | |
| Platelets: 206 (140 - 440 x 10^3/uL) | |
| Basic Metabolic Panel | Sodium: 135 (136 - 145 mmol/L) |
| CO2: 22 (23 - 31 mEq/L), | |
| eGFR: 50 (>60 mL/min) | |
| Glucose: 131 mg/dL (Fasting 83 - 110 mg/dL) | |
| Potassium: 4.0 (3.5 - 5.1 mmol/L) | |
| Chloride: 104 (98 - 107 mmol/L) | |
| Creatinine: 1.10 (0.60 - 1.10 mg/dL) | |
| Magnesium: 2.2 (1.6 - 2.6 mg/dL) | |
| Phosphorus: 3.7 (2.3 - 4.7 mg/dL) | |
| Lactate: 1.4 (0.5 - 2.0 mmol/L) | |
| Coagulation Studies | aPTT: 23 s (23 - 35 Seconds) |
| Protime: 10.9 (9.0 - 12.0 seconds) | |
| INR: 1.0 (0.8 - 1.1) | |
| E-FAST Scan | |
| Thorax | Good lung sliding in all quadrants, no evidence of pneumothorax |
| Heart | Small pericardial effusion, no evidence of right ventricular collapse |
| Hepatorenal Pouch | No evidence of free fluid noted |
| Splenorenal Pouch | No evidence of free fluid noted |
| Pelvis | No evidence of free fluid around the bladder |
| Radiological Findings | |
| CT Abdomen & Pelvis | No visceral or bony injury, small umbilical hernia, multilevel lumbar disc protrusions |
| CT Chest | Clear lungs, no pneumothorax or pleural effusion, no aortic injury, coronary artery calcification |
| X-rays | No fractures or dislocations in tibia, fibula, ankle, wrist, or knees; osteoarthritis noted in the left wrist |
| Lab Component | Units | Day 1 | Day 2 | Range |
| WBC | 10³/µL | 7.74 | N/a | 4.50 - 11.00 10*3/uL |
| Hemoglobin | g/dL | 13.0 | N/a | 11.5 - 16.0 g/dL |
| Hematocrit | % | 39 | N/a | 37 - 47 % |
| Platelets | 10³/µL | 222 | N/a | 140 - 440 10*3/uL |
| Sodium | mmol/L | 137 | N/a | 136 - 145 mmol/L |
| Potassium | mmol/L | 4.1 | N/a | 3.5 - 5.1 mmol/L |
| Chloride | mmol/L | 104 | N/a | 98 - 107 mmol/L |
| CO2 | mEq/L | 23 | N/a | 22 - 29 mEq/L |
| BUN | mg/dL | 18 | N/a | 9 - 21 mg/dL |
| Creatinine | mg/dL | 1.00 | N/a | 0.60 - 1.10 mg/dL |
| Glucose (Fasting) | mg/dL | 121 | N/a | 70 - 105 mg/dL |
| Calcium | mg/dL | 9.10 | N/a | 8.50 - 10.30 mg/dL |
| Troponin I HS | ng/L | 9,755 | 10,716 | 0 - 34 ng/L |
| CK Total | U/L | N/a | 542 | 30 - 190 U/L |
| Troponin I | ng/mL | N/a | 3.43 | 0.00 - 0.05 ng/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTakotsubo Cardiomyopathy and Associated Phenomena · Pericarditis and Cardiac Tamponade · Cardiac Health and Mental Health
Introduction
Takotsubo cardiomyopathy (TTC), also known as stress-induced cardiomyopathy or "broken heart syndrome," is a transient form of myocardial dysfunction often triggered by emotional or physical stress. Although TTC is more commonly linked to emotional stress or physical stress, it can occur, albeit rarely, after physical trauma, including blunt chest injuries. The proposed mechanisms in these cases involve a surge in catecholamines or autonomic dysregulation, both of which can precipitate transient myocardial dysfunction following significant physical stress [1]. This case report presents a particularly novel instance of TTC in an 84-year-old woman who developed the condition after a motor vehicle accident (MVA) resulting in blunt chest trauma. What makes this case unique is not only the patient's age but also the severity of systolic dysfunction, with an initial left ventricular ejection fraction (LVEF) of 25-30%, indicating severe impairment. Coronary artery disease was ruled out through coronary angiography, which showed no significant coronary obstruction. The patient's clinical course, diagnostic findings, and management are discussed, highlighting the importance of considering TTC in elderly patients presenting with chest pain and cardiac dysfunction following blunt trauma. This case contributes to the literature by illustrating how physical trauma, particularly in the elderly, can trigger TTC, challenging the assumption that the condition is predominantly linked to emotional stress.
Case presentation
An 84-year-old woman with a past medical history of hyperlipidemia and hypothyroidism presented to the emergency department, after being involved in an MVA. She was the driver of a vehicle that collided with another car, resulting in airbag deployment and blunt chest trauma. Although initially evaluated by EMS at the scene, she declined transport to the hospital and went home. However, later in the day, she sought medical attention due to chest discomfort radiating to her back. She denied difficulty breathing, numbness, weakness, or any other neurological symptoms. On examination, the patient displayed bruising across her chest, but there were no signs of acute respiratory distress or other traumatic injuries beyond minor abrasions and a small hematoma on her left thumb. Her initial findings are noted in Table 1.
Her ECG (electrocardiogram) done at triage on initial presentation is noted in Figure 1.
ECG on the initial presentation showing diffuse sinus tachycardia ST elevation
Upon arrival at the level 1 trauma center, the patient denied dizziness, dyspnea on exertion, shortness of breath, or loss of consciousness but complained of localized chest pain at the site of bruising on the anterior chest wall. On examination, she had tenderness in the left anterior chest wall and mild tenderness in the lower abdomen. No fractures or open wounds were observed. The patient's concerns were addressed, and analgesia was provided for comfort. An EFAST (extended focused assessment with sonography for trauma) scan was conducted which revealed mild pericardial fluid; however, no other signs of trauma such as free fluid in the abdomen or pneumothorax were noted. Chest and abdominal CT scans with contrast were performed, revealing no visceral or bony injuries, but mild atelectasis in the lungs and a small cyst in the liver were noted. X-rays of the limbs showed no fractures or dislocations. While a STEMI (ST elevated myocardial infarction) was initially suspected due to widespread ST elevation on the ECG, the cardiologist also considered blunt trauma-induced pericarditis given the non-reciprocal ST changes. However, given that a STEMI could not be definitively ruled out, heparin infusion therapy was initiated as a precautionary measure. The patient’s high-sensitivity troponin levels were elevated at 3.43ng/ml, and she was admitted to the ICU for close monitoring. An echo was scheduled for the following morning to further assess the patient's cardiac function.
A summary of her clinical findings can be found in Table 2.
The patient was assessed by the surgical trauma team who after careful assessment found no acute traumatic injuries and recommended admitting the patient in the ICU for medical management. In the ICU, the patient was managed with close monitoring, heparin infusion, and measures to trend troponin levels. There were no acute concerns regarding respiratory, gastrointestinal, or renal systems. The plan included NPO status, monitoring vital signs, and adjusting glucose levels as needed.
On day 2, the patient was treated symptomatically for mild pain; however, there was no acute deterioration. Her heparin infusion was continued as protocol. Her initial troponin was elevated at 11,000, trending down to 9,755, with CK and myoglobin also elevated. Her lab values in the first 48 hours are reported in Table 3.
The decision was taken to undergo transthoracic echocardiography by the cardiologist in order to assess for the possible presence of cardiac dysfunction in this patient. Echocardiography revealed a left ventricle with normal size but mild thickening of the heart muscle (concentric hypertrophy). Severe systolic dysfunction was observed with a significantly reduced ejection fraction (25-30%). Diastolic filling was not assessed, and left atrial pressure remained within normal limits. Several segments of the left ventricle showed reduced or no movement (akinesis) as well as the presence of apical ballooning was noted on the echo. The right ventricle exhibited normal size and function. Both atria were of normal size. The inferior vena cava was dilated and demonstrated poor collapse, suggesting elevated right atrial pressure. Mild regurgitation was noted on the mitral, tricuspid, and aortic valves, with no significant narrowing (stenosis). The pulmonic valve appeared normal, but pulmonary artery pressure was moderately elevated at 46 mmHg, indicative of moderate pulmonary hypertension. A small pericardial effusion was present without evidence of cardiac tamponade.
An echo video noted in Video 1 represents the parasternal long-axis view. Note the apical dilation in the left ventricle.
The parasternal long-axis view with the apical dilation in the left ventricle
Based on the findings of the echocardiogram, a decision was made to catheterize the patient to rule out ischemic etiology. Informed consent was obtained from the patient after a thorough discussion of the procedure. Following sterile preparation and local anesthesia, a diagnostic coronary angiogram was performed via right radial artery access. Left and right coronary arteries were visualized and found to be normal with the exception of a non-occlusive myocardial bridge in the mid-left anterior descending artery (LAD). Left ventriculography revealed severe systolic dysfunction with an ejection fraction of approximately 25%. Regional wall motion abnormalities consistent with apical ballooning (Takotsubo cardiomyopathy) were observed. Left ventricular end-diastolic pressure was normal at 9 mmHg. Hemodynamic assessment across the aortic valve revealed no significant pressure gradient. Coronary artery catheterization is noted in Video 2.
Coronary catheterization
In conclusion, the patient had non-obstructive coronary artery disease and TTC. The patient was managed conservatively and was started on metoprolol 12.5 mg daily. On day 3, she was found to be comfortable. She was discharged with a LifeVest® wearable cardioverter defibrillator (WCD) and advised to continue her previous medications as well as metoprolol 12.5 mg daily. The WCD and metoprolol were prescribed to her as a precautionary measure against cardiac arrhythmias. She was also advised to follow up with her cardiologist and primary care provider for close monitoring. Her final diagnosis on discharge was TTC and pericardial effusion secondary to blunt chest injury from an MVA.
Discussion
TTC, also known as stress-induced cardiomyopathy or "broken heart syndrome," is a transient cardiac condition typically triggered by severe emotional or physical stress. It presents with symptoms similar to acute myocardial infarction, including chest pain and ST-segment elevation on ECG, but without the presence of obstructive coronary artery disease [1]. The diagnosis of TTC often relies on the modified Mayo Clinic criteria, which include the absence of significant coronary artery disease on angiography, transient abnormalities in left ventricular wall motion with mid-segment hypokinesis or akinesis and potential apical involvement, electrocardiographic evidence of ST-segment elevation and/or T-wave inversion, modest elevations in cardiac troponin levels, and the exclusion of other conditions such as myocarditis and pheochromocytoma [2]. The pathophysiology is thought to involve a sudden surge of catecholamines, leading to myocardial stunning, particularly affecting the left ventricle. This results in characteristic findings on imaging, such as a severely reduced ejection fraction with regional wall motion abnormalities, most commonly in the apical and mid-ventricular regions, while sparing the basal segments. This was first described by Sato et al. in 1990 after which the term was coined as Takatsubo cardiomyopathy after the classic octopus traps [3].
In this case, the patient's left ventriculogram revealed a 25% ejection fraction with anterolateral, apical, and diaphragmatic akinesis, supporting the TTC diagnosis. While a mid-LAD myocardial bridge could theoretically exacerbate stress-induced myocardial dysfunction in TTC by contributing to intermittent ischemia, in this case, it was non-occlusive. TTC, triggered by intense emotional or physical stress, causes temporary heart muscle weakening, particularly in the left ventricle. Although often self-limiting and requiring supportive care, recognizing TTC is crucial for appropriate management and avoiding unnecessary interventions. The etiology of TTC remains incompletely understood but is believed to involve catecholamine surges triggered by acute stress, leading to transient left ventricular dysfunction, particularly in the apical and mid-ventricular regions [4]. Additional contributing factors may include microvascular spasm, endothelial dysfunction, and inflammation. Risk factors include emotional stress, physical trauma, neurological events, or severe illness, with postmenopausal women being more commonly affected [4].
The exact cause of the contractile pattern in TTC is unclear, with several theories proposed. One suggests multivessel coronary artery spasm may lead to regional myocardial stunning, but this does not explain the severe apical dysfunction or mild cardiac enzyme elevation [3,5-7]. While coronary microvascular impairment has been observed, its role remains uncertain. Abnormal left ventricular wall motion, particularly affecting the apical myocardium, suggests potential disturbances in the coronary microcirculation. Studies, including those by Kume et al., Yoshida et al., and Khalid et al., have shown impaired coronary perfusion and metabolic abnormalities [8-10], with Elesber et al. noting a correlation between microvascular dysfunction and the severity of myonecrosis and ECG changes [11]. These findings indicate microvascular abnormalities may be involved, but whether they are a cause or result of apical ballooning remains unclear [12].
Elevated catecholamine levels, particularly epinephrine, appear to trigger myocardial dysfunction in TTC [13-15]. These high levels can lead to intracellular calcium overload, contraction band necrosis, and myocardial stunning. Elevated catecholamines (norepinephrine, epinephrine, and dopamine) are consistently observed in TTC patients, often two to three times normal [13-15]. This catecholamine surge induces changes in myocardial contractility via beta-2-adrenoceptor stimulation, leading to negative inotropic effects and left ventricular dysfunction. This "stimulus trafficking" is particularly relevant in the apical form of TTC, where beta-adrenergic receptors are most concentrated. Intravenous catecholamine or beta-adrenergic agonist administration can reproduce TTC's clinical features, further supporting the role of excessive catecholamine release [13-15]. Beta-blockers, such as metoprolol, reduce myocardial oxygen demand and myocardial stunning by blocking β1 and β2 receptors. Thus, the rationale behind using beta-blockers in TTC is to mitigate the acute effects of catecholamine excess on the heart, stabilizing the patient’s condition and helping prevent further myocardial damage or arrhythmias. While there is no definitive consensus on the optimal timing and duration for beta-blocker therapy in TTC, it is postulated that their use during the acute phase provides symptomatic relief and supports recovery by reducing stress on the heart muscle and minimizing the risk of further complications. As such, beta-blockers have become a key component in the management of TTC, with the catecholamine hypothesis being widely accepted as the primary pathophysiologic mechanism [13-15].
TTC's pathophysiology remains complex. Histologically, it is characterized by interstitial infiltrates (primarily mononuclear lymphocytes, leukocytes, and macrophages), myocardial fibrosis, and contraction bands, distinguishing it from ischemic myocardial infarction [16]. Inflammation is believed to play a significant role. Cardiac MRI reveals myocardial edema, necrosis, and fibrosis [16]. Late gadolinium enhancement (LGE), while once thought absent, is present in up to 10% of cases, typically in a focal or patchy pattern [17,18], distinct from myocarditis or ischemia. This LGE usually resolves with follow-up. Studies have shown macrophage recruitment, monocyte subtype changes, and increased pro-inflammatory cytokines [19]. Coexisting inflammatory or autoimmune conditions have been reported [20], though diagnostic guidelines (Mayo Clinic and the European Society of Cardiology) exclude myocarditis as a TTC criterion. Histological analysis has shown contraction band necrosis, inflammatory cell infiltration, and focal fibrosis, possibly from catecholamine cardiotoxicity [21].
Estrogen has cardioprotective effects, including vasodilation and prevention of atherosclerosis and endothelial dysfunction [22]. The predominance of postmenopausal women among TTC patients suggests estrogen deficiency may increase the risk. Studies show that the absence of estrogen replacement therapy may predispose women to the condition, and murine models indicate that ovariectomy removes cardiac protection, which is restored with estradiol [23]. Estrogen may also down-regulate beta-adrenergic receptors, linking its deficiency to Takotsubo risk. While rarer in men, TTC tends to have a worse prognosis in males, potentially due to the lack of estrogen’s protective effects [24].
The "aborted myocardial infarction" hypothesis suggests Takotsubo syndrome results from transient coronary occlusion due to acute thrombus formation followed by rapid lysis. Though angiography is often normal, intravascular imaging (IVUS, OCT) has revealed atherosclerotic vulnerabilities, such as eccentric plaques and thin-cap fibroatheromas in the mid-LAD, which may lead to transient occlusion [25,26]. Coronary artery vasospasm has also been implicated, with studies showing evidence of spasm and vasoconstriction, supported by acetylcholine provocation testing [3,27].
Neurogenic mechanisms, such as central nervous system activation during emotional distress, may also play a role in the myocardial changes seen in TTC. Overall, the condition is likely due to a combination of high local catecholamine concentrations, myocardial necrosis, and impaired adrenergic responsiveness, primarily induced by severe emotional stress. A combination of factors as discussed above may be responsible for the development of TTC in this patient. Trauma as a cause has been rarely implicated in the development of TTC. Ahmed et al. reported a case with reverse TTC and commotio cordis secondary to trauma from an MVA. The case was reported to be a variant of TTC which showed basal hypokinesis/akinesis with apical sparing or hyperkinesis [28]. Another case report by Ritchie et al. reported a 59-year-old woman who developed TTC and pulmonary edema following a motor vehicle collision, presenting with respiratory distress and ST elevation on ECG, but without coronary artery occlusion. Coronary angiography confirmed apical ballooning, and the patient improved rapidly. TTC poses a diagnostic challenge, especially in trauma patients where other serious conditions, such as acute coronary syndrome (ACS) or aortic injury, must be ruled out. A systematic review by Gruhl et al. found that patients with traumatic brain injury may develop TTC due to catecholamine excess. It was reported that these patients underwent quick resolution of cardiac pathology as long as the TBI was managed appropriately [29]. Similarly, Cimaroli et al. demonstrated a case of TTC similar to this case in a patient following blunt chest trauma [30] which highlights the need for further evaluation to assess trauma as a potential cause for it.
The differential diagnosis for TTC is broad, encompassing several conditions that can mimic ACS. A key challenge is differentiating TTC from myocardial infarction (MI), as both can present with chest pain, ECG changes, and elevated cardiac enzymes. However, TTC is typically characterized by the absence of obstructive coronary artery disease on angiography and the presence of left ventricular apical ballooning. Myocardial contusion, particularly in cases of trauma, is another important consideration. It can also cause chest pain and ECG abnormalities. However, unlike TTC, myocardial contusion often shows evidence of direct myocardial injury, such as wall motion abnormalities that extend beyond the apex and may be associated with other traumatic injuries. Other conditions that should be considered include myocarditis, pericarditis, and pulmonary embolism, each with distinct clinical and diagnostic features. To differentiate TTC from these other conditions, a comprehensive evaluation involving cardiac imaging and biomarker testing is essential. TTC typically has an excellent prognosis with nearly full recovery within 6-8 weeks. Recurrence rates are low, estimated at around 1-2%. Mortality rates are generally low, reported to be between 3-4%. However, complications can occur in a significant proportion of patients (at least 25%). These complications may include mitral regurgitation (mild to moderate), left heart failure, cardiogenic shock, dynamic left ventricular outflow tract obstruction, the development of left ventricular mural thrombi, ventricular arrhythmias, ventricular wall rupture, and, in rare cases, death [4].
Conclusions
In conclusion, this case underscores the importance of considering TTC in patients presenting with acute coronary syndrome-like symptoms following significant trauma, such as an MVA. "Apparent myocardial injury" in this context refers to the absence of both coronary artery occlusion (as would be seen in a myocardial infarction) and evidence of myocardial necrosis on initial imaging. The stress of the traumatic event can precipitate catecholamine-induced myocardial dysfunction, leading to the characteristic apical ballooning of TTC, even without direct cardiac injury. Differentiating TTC from other life-threatening conditions, particularly myocardial infarction, is crucial to avoid unnecessary interventions such as thrombolysis or coronary angioplasty. Misdiagnosis as ACS could also lead to inappropriate administration of antithrombotic therapy, with its associated risks. This case demonstrates the generally favorable prognosis of TTC with appropriate recognition and supportive care. However, while most patients experience rapid recovery, it is important to acknowledge the potential for complications such as heart failure, arrhythmias, or cardiogenic shock. A comprehensive diagnostic approach, integrating advanced imaging like cardiac MRI and biomarker assessment (including troponins and BNP), is essential. Finally, appropriate follow-up care is necessary to monitor for recurrence or the development of long-term myocardial dysfunction such as heart failure or cardiomyopathy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Takotsubo cardiomyopathy Stat Pearls [Internet] Ahmad SA Brito D Khalid N Ibrahim MA Treasure Island (FL)Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 430798/28613549 · pubmed ↗
- 2Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction Am Heart J Prasad A Lerman A Rihal CS 40841715520081829447310.1016/j.ahj.2007.11.008 · doi ↗ · pubmed ↗
- 3Takotsubo-type cardiomyopathy due to multivessel spasm Clinical Aspect of Myocardial Injury: From Ischemia to Heart Failure Sato H Tateishi H Uchida T 5664 Tokyo, Japan Kagakuhyouronsha 1990 https://cir.nii.ac.jp/crid/1570854175774875008
- 4Pathophysiology of Takotsubo syndrome Stat Pearls [Internet] Khalid N Ahmad SA Shlofmitz E Chhabra L Treasure Island (FL)Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 538160/30844187 · pubmed ↗
- 5Differentiation between patients with takotsubo cardiomyopathy and those with anterior acute myocardial infarction Circ J Inoue M Shimizu M Ino H 89946920051563521010.1253/circj.69.89 · doi ↗ · pubmed ↗
- 6Electrocardiography cannot reliably differentiate transient left ventricular apical ballooning syndrome from anterior ST-segment elevation myocardial infarction J Electrocardiol Bybee KA Motiei A Syed IS 383640200710.1016/j.jelectrocard.2006.04.00717067626 · doi ↗ · pubmed ↗
- 7Release pattern of cardiac biomarkers in left ventricular apical ballooning Int J Cardiol Nef HM Mollmann H Weber M Deetjen A Brandt R Hamm CW Elsasser A 1281291152007 https://www.internationaljournalofcardiology.com/article/S 0167-5273(06)00299-3/abstract 1676913810.1016/j.ijcard.2006.01.034 · doi ↗ · pubmed ↗
- 8Assessment of coronary microcirculation in patients with takotsubo-like left ventricular dysfunction Circ J Kume T Akasaka T Kawamoto T 9349396920051604116210.1253/circj.69.934 · doi ↗ · pubmed ↗