Endoscopic ultrasonography‐guided removal of a stent that had migrated into the pancreas post‐pancreaticojejunostomy: A case report
Satoshi Kajitani, Kazuyuki Matsumoto, Kentaro Oki, Akihiro Matsumi, Kazuya Miyamoto, Yuki Fujii, Daisuke Uchida, Koichiro Tsutsumi, Shigeru Horiguchi, Motoyuki Otsuka

TL;DR
A 64-year-old woman had a migrated stent successfully removed from her pancreas using endoscopic ultrasonography after previous attempts failed.
Contribution
Demonstrates a novel endoscopic ultrasonography-guided technique for stent removal in a complex post-surgical case.
Findings
Endoscopic ultrasonography-guided drainage allowed access to the pancreatic duct for stent removal.
The patient's symptoms improved after successful stent removal without complications.
The technique provided a safe alternative when traditional endoscopic methods failed.
Abstract
A 64‐year‐old woman had undergone subtotal stomach‐preserving pancreaticoduodenectomy for locally advanced pancreatic head cancer. She had an uneventful postoperative course with no recurrence. However, approximately 18 months after surgery, she presented with recurrent abdominal pain. Although contrast‐enhanced computed tomography abdominal radiographs showed internal stent migration to the residual pancreas, dilatation of the tail side of the pancreatic duct was observed. The impaired internal stent was considered to be the cause of the abdominal pain. An attempt to remove the stent via balloon‐assisted endoscopy was unsuccessful as the pancreaticojejunostomy site could not be reached. Consequently, endoscopic ultrasonography‐guided pancreatic duct drainage was performed, and a plastic stent was placed through the jejunal site to the stomach. Two months later, the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
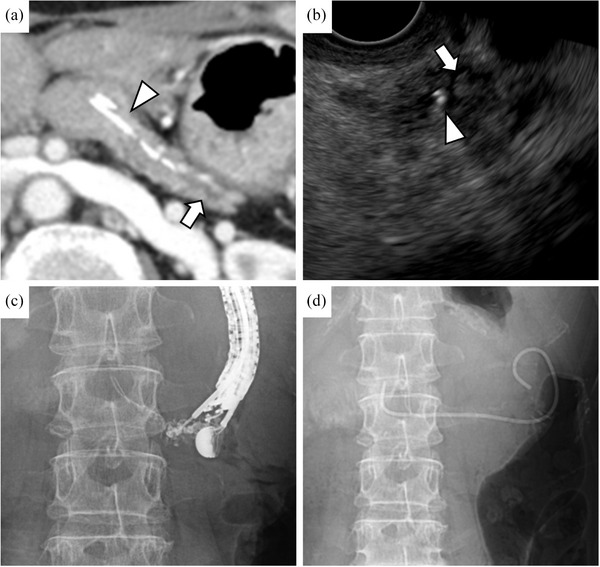 FIGURE 1
FIGURE 1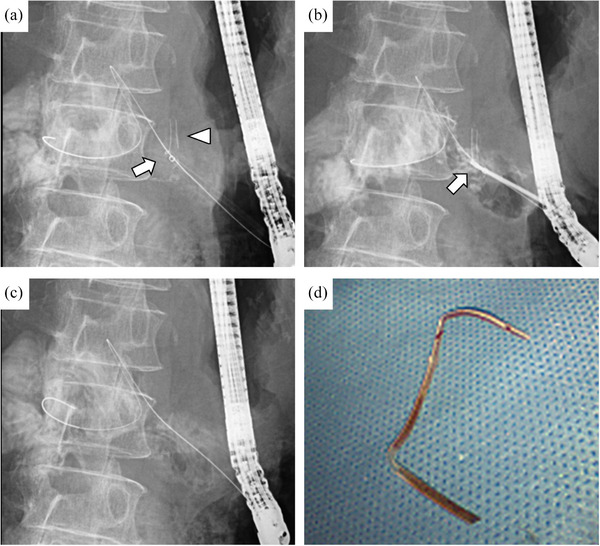 FIGURE 2
FIGURE 2| Author | Age (y) | Sex | Etiology | Migrated sent Size/length/type | Symptoms | Device delivery system | Grasping device | Complications |
|---|---|---|---|---|---|---|---|---|
| Kato A. | 84 | F | IPMN | 7Fr/NA/plastic stent | Unknown | EndoSheather | Basket catheter | None |
| Higashimori A. | 55 | M | CP | 5Fr/NA/Plastic stent (fracture) | None | EndoSheather | Biopsy forceps | None |
| Matsumi A. | 80 | M | Prevention for PEP | 5Fr/3 cm/plastic stent | None | EndoSheather | Biopsy forceps | None |
| Ushio M. | 78 | F | Prevention for PEP | NA/NA/plastic stent | Pancreatitis | UMIDAS sheath cannula | Biopsy forceps | None |
| Takahashi K. | 71 | M | Prevention for PEP | 5Fr/3 cm/plastic stent | None | 8.5Fr stent pusher tube | Basket catheter | None |
| Author | Age | Sex | Etiology | Surgery | Symptoms | Migrated stent | Device | Grasping instrument | Complications |
|---|---|---|---|---|---|---|---|---|---|
| Takahashi S. | 68 | M | Cholangiocarcinoma | PD | None |
Straight type Trans‐jejunal plastic stent | SpyDS | Snare | None |
| Our case | 64 | F | Pancreatic carcinoma | PD | Abdominal pain |
Straight type Internal plastic stent | EndoSheather | Biopsy forceps | None |
- —None
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Esophageal and GI Pathology · Gallbladder and Bile Duct Disorders
INTRODUCTION
Internal stents are often placed at the pancreatojejunostomy site following pancreaticoduodenectomy (PD) to prevent postoperative complications such as pancreatic fistulas.1 While these stents are usually expelled spontaneously,2 retained stents can lead to complications in rare cases, including pancreatitis. Balloon‐assisted endoscopy is typically used to remove retained stents. However, postoperative adhesions and anatomical alterations disrupt access to the pancreatojejunostomy site.
Endoscopic ultrasonography‐guided pancreatic duct drainage (EUS‐PD) has been reported as an effective approach for pancreatic duct assessment in patients with surgically reconstructed intestinal anatomy.3 EUS‐PD is particularly useful in cases where conventional balloon‐assisted endoscopy fails. Notably, several treatments using a trans endosonographically/EUS‐guided created route (ESCR) have been reported.
Recently, a newly developed endoscopic introducer with a dual‐layer structure, consisting of an inner sheath and an outer sheath, enabled device insertion up to 5.7Fr diameter after the removal of the inner sheath. This device is useful for biopsies of bile duct lesions and for overcoming challenging cases.4, 5, 6, 7, 8 Here, we report a case of successful removal of an internal stent that had migrated to the pancreatic duct following PD by employing an ESCR that involved using a newly developed endoscopic introducer.
CASE REPORT
A 64‐year‐old woman was diagnosed with an unresectable locally advanced pancreatic head cancer. She underwent chemotherapy with modified folinic acid, fluorouracil, irinotecan, and oxaliplatin (mFOLFIRINOX) for 18 months, which achieved local tumor control without the emergence of distant metastases. Subsequently, radiotherapy was administered, followed by a subtotal stomach‐preserving PD. Approximately 18 months later, the patient presented with recurrent, persistent abdominal pain that lasted for approximately 1 month, prompting her to seek medical attention. Laboratory test results showed no evidence of an inflammatory response or elevated pancreatic enzyme levels (white blood cell 1.69 × 10^3^/µL, C‐reactive protein 0.04 mg/dL, amylase 94 mg/dL, and lipase 13 U/L). However, the glycosylated hemoglobin A1c levels of the patient worsened compared to 2 months prior measurement (8.2% vs. 7.4%, respectively).
Abdominal contrast‐enhanced computed tomography revealed a retained internal stent in the pancreatic duct with dilation of its tail side (Figure 1a). EUS identified the stent and debris echoes, suggesting an obstruction of pancreatic juice outflow (Figure 1b). The abdominal pain was attributed to obstruction of pancreatic juice outflow caused by the internal stent. First, double‐balloon enteroscopy (DBE) was conducted using a short‐type DBE (EI‐580BT: working length 1550 mm; Fujifilm) which failed to access the pancreatojejunostomy site due to postoperative intestinal adhesions. A long‐type DBE (EN‐580T: working length 2000 mm; Fujifilm) was then attempted but remained unsuccessful even for 110 min. Consequently, stent removal via an EUS‐PD route was planned.
Radiographs showing a stent that had migrated into the pancreatic duct. (a) Using contrast‐enhanced computed tomography, an internal stent (arrowhead) was observed within the main pancreatic duct, along with dilation of the tail side of the main pancreatic duct (arrow). (b) Employing endoscopic ultrasonography, an internal stent (arrowhead) and debris echoes (arrow) were identified within the pancreatic duct. (c) The pancreatic duct was punctured transgastrically using a 19G needle for fine‐needle aspiration. (d) A 6Fr double pigtail plastic stent was placed with one pigtail positioned in the jejunum and the other in the stomach.
The pancreatic duct was punctured transgastrically using a 19G needle (EZ Shot 3 Plus; Olympus), followed by the insertion of a 0.025‐inch guidewire (VisiGlide 2; Olympus) that was advanced across the pancreatojejunostomy site (Figure 1c). After dilating the puncture site using a drill‐type endoscopic dilator (Tornus ES; Asahi Intecc), a 6Fr double‐pigtail plastic stent (Zimmon Biliary Stent; Cook Medical) was placed, considering the 2 mm pancreatic duct and the risk of deviation. One pigtail was positioned in the jejunum and the other in the stomach (Figure 1d).
Approximately 2 months later, the double‐pigtail plastic stent was removed using forceps after securing the route with a guidewire. The ESCR was dilated to 4 mm using a balloon dilator (REN; KANEKA Medix), and an endoscopic introducer (EndoSheather; Piolax) was placed within the pancreatic duct (Figure 2a). Bbiopsy forceps (1.8 mm outer cup diameter, Radial Jaw 4; Boston Scientific) were then inserted to directly grasp and remove the internal stent (Figure 2b–d). On the same day, to prevent post‐procedural pancreatitis, a 7Fr single‐pigtail plastic stent (Through & Pass TYPE IT; KANEKA Medix) was placed and the patient was discharged without any complications. The pancreatic duct stent was removed approximately one month later, leading to symptom improvement.
Radiographs showing the removal of a stent that had migrated into the pancreatic duct. (a) An endoscopic introducer (arrow) was placed near the internal stent (arrowhead) within the pancreatic duct. (b) Biopsy forceps (arrow) were inserted into the endoscopic introducer to directly grasp the internal stent. Both the introducer and the stent were retracted together. (c) The internal stent was successfully removed without any remnants. (d) Photograph of the removed internal stent.
DISCUSSION
In PD, internal stents are often placed in the pancreatic duct to prevent postoperative pancreatic fistulas and to maintain ductal patency in early anastomotic edema cases.1 According to Kadowaki et al., internal stents are spontaneously expelled in most cases, with a reported median time to expulsion of 454 days.2 Shin et al. reported that among 88 patients with internal stent placement after pancreaticobiliary surgery, abnormal stent migration occurred in nine patients (10.2%) within the first year. The migration sites included the hepaticojejunal anastomosis in four cases, the intrahepatic duct in three cases, and the remnant pancreatic duct in two cases.9 Since the migration site can cause pancreatitis, intestinal obstruction, liver abscess, or cholangitis, stent removal is recommended for symptomatic and asymptomatic cases where the stent has been retained for 18 months or more.
Stent retrieval methods include surgical, percutaneous, and endoscopic approaches. Among them, endoscopic retrieval is often attempted first due to its minimally invasive nature. However, there are no dedicated devices for the retrieval of migrated stents, and most endoscopists use several existing devices to remove them. Recently, the endoscopic introducer was developed to deliver endoscopic devices more safely and accurately. This device consists of a 7.2Fr outer sheath and a tapered inner sheath, which reduces the step between the guidewire and the sheath, allowing smooth insertion. The device is advanced over a guidewire to the target site; once positioned, the guidewire and inner sheath are removed, leaving the outer sheath in place. Devices up to 5.7Fr in diameter can then be inserted or removed through the outer sheath. A PubMed search (duration: 2015–2024) with the keywords “migrated stent,” “pancreas,” “pancreatic stent,” “sheath,” “device delivery system,” and “pusher tube” identified five cases of successful retrieval of migrated pancreatic stents using a device delivery system (Table 1). The median patient age was 78 years, including three men and two women. The stents were all made of plastic, and the device delivery system was inserted through the papilla in all cases. The endoscopic introducer was used in three cases, endoscopic retrograde cholangiopancreatography guided sheath (UMIDAS sheath cannula; Olympus) in one case, and a method utilizing an 8.5Fr bile duct stent pusher tube was employed in one case. Biopsy forceps were used in three cases and basket catheters in two cases. All cases were successfully managed without complications.
PubMed search (duration: 2015–2024) using the keywords “endoscopic ultrasound‐guided pancreaticogastrostomy” and “migrated stent” identified only one case of stent removal through ESCR. In that case, following PD, DBE was performed for pancreatic duct drainage but resulted in intestinal perforation, necessitating EUS‐PD. Subsequently, two plastic stents were regularly exchanged. However, one straight‐type plastic stent migrated into the pancreatic duct. Using a peroral pancreatoscope (POPS), the migrated stent was successfully retrieved via ESCR.10 In this case, due to the narrow pancreatic duct diameter, POPS insertion was challenging. Instead, the endoscopic introducer was used, and biopsy forceps were successfully used to remove the stent. This approach proved cost‐effective, and efficient and reduced procedural time (Table 2).
This case report details the first report of the successful retrieval of an internal stent that migrated to a remnant pancreas after PD using an endoscopic introducer via ESCR. Traditionally, approaching the pancreatic duct in reconstructed intestines using DBE involves several steps, including advancing the scope to the pancreatojejunostomy, identifying the pancreatic duct anastomosis, and inserting the catheter. Each of these steps can be anatomically challenging and often preoperatively unpredictable. Utilizing ESCR is unaffected by these factors, allowing for a rapid approach to the pancreatic duct and a reduction in procedure time. Furthermore, in the present case, the method combined existing techniques and devices, making it universally applicable in enabling stent removal in a low‐cost, safe, and minimally invasive manner compared to open surgery. For cases where DBE‐ERCP is challenging or where procedure time needs to be minimized, this technique may be used as a viable treatment option. With further standardization and safety validation, ESCR has the potential to become a treatment option comparable to DBE.
CONFLICT OF INTEREST STATEMENT
None.
ETHICS STATEMENT
N/A
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Goh SK , Kok HK , Houli N . Intrahepatic migration of pancreatic stent after pancreaticoduodenectomy: Percutaneous cholangioscopic retrieval is feasible. BMJ Case Rep 2021; 14: e 244380.10.1136/bcr-2021-244380 PMC 848716734593550 · doi ↗ · pubmed ↗
- 2Kadowaki S , Miura F , Amano H et al. Whereabouts of an internal short stent placed across the pancreaticojejunostomy following pancreatoduodenectomy. J Hepatobiliary Pancreat Sci 2012; 19: 566–577.22869100 10.1007/s 00534-012-0533-7 · doi ↗ · pubmed ↗
- 3Will U , Fueldner F , Buechner T et al. Endoscopic ultrasonography‐guided drainage of the pancreatic duct (EUS‐PD)‐indications and results with a literature review. J Clin Med 2024; 13: 7709.39768632 10.3390/jcm 13247709 PMC 11677581 · doi ↗ · pubmed ↗
- 4Kato A , Natsume M , Yoshida M et al. Endoscopic tapered sheath‐assisted removal of a proximally migrated pancreatic stent. Endoscopy 2022; 54: E 767–768.35359015 10.1055/a-1792-2955 PMC 9735239 · doi ↗ · pubmed ↗
- 5Higashimori A , Maruyama H , Maeda N et al. Successful retrieval of a fractured migrated pancreatic stent using an endoscopic tapered sheath for severe pancreatic duct stenosis. Endoscopy 2023; 55: E 747–748.37236262 10.1055/a-2086-1946 PMC 10219759 · doi ↗ · pubmed ↗
- 6Matsumi A , Matsumoto K , Uchida D et al. Successful removal of a proximally migrated pancreatic stent using a novel device delivery system. Endoscopy 2023; 55: E 641–642.37068740 10.1055/a-2063-3408 PMC 10110365 · doi ↗ · pubmed ↗
- 7Ushio M , Tomishima K , Ishii S et al. Successful withdrawal of migrated pancreatic stent with a prototype guiding sheath. Endoscopy 2023; 55: E 5–6.36084939 10.1055/a-1907-4640 PMC 9812664 · doi ↗ · pubmed ↗
- 8Takahashi K , Ohyama H , Mikata R et al. Successful endoscopic retrieval of a migrated pancreatic stent using a basket catheter for peroral cholangioscopy through a biliary plastic stent pusher tube: A case report. J Rural Med 2022; 17: 189–192.35847756 10.2185/jrm.2022-003PMC 9263960 · doi ↗ · pubmed ↗