Woman With a Swollen Finger
Gayle Galletta

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
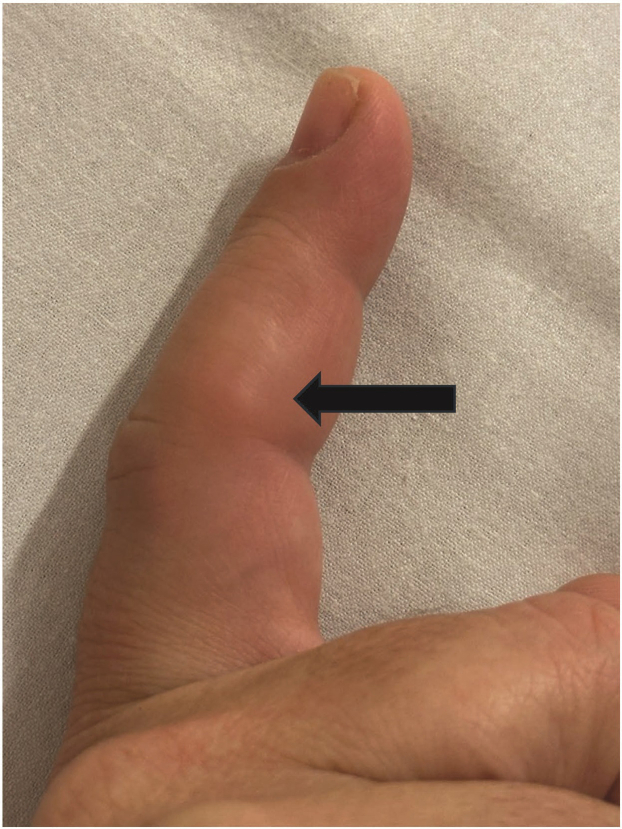 Figure 1
Figure 1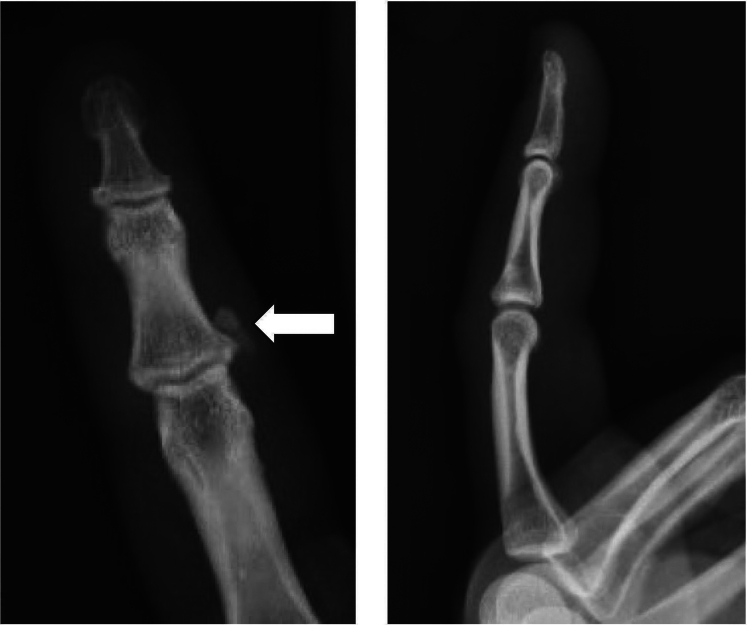 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Surgery and Rehabilitation · Sarcoma Diagnosis and Treatment · Musculoskeletal synovial abnormalities and treatments
Case Presentation
1
A 46-year-old right-handed woman presented to a community emergency department with a 2-day history of progressively worsening pain, redness, and swelling to her right index finger proximal interphalangeal joint (Fig 1). She denied trauma but states that the pain worsens with activity, especially working as a barista at a coffee shop. The physical examination was normal except for redness, swelling, and exquisite tenderness of the ulnar aspect of the right index finger proximal interphalangeal joint. There was no tenderness over the flexor tendon. Finger x-rays were obtained (Fig 2).Figure 1. Right index finger with tender nodule (black arrow) at the proximal interphalangeal joint.Figure 2. Anterior-posterior and lateral images of the right index finger demonstrate a soft tissue calcification at the ulnar aspect of the index finger proximal interphalangeal joint (white arrow), suggestive of calcium hydroxyapatite deposition disease.
Diagnosis: Hydroxyapatite Crystal Deposition Disease
2
Hydroxyapatite crystal deposition disease (HADD) is a rare cause of hand and wrist pain and causes swelling that may mimic infectious arthritis or tenosynovitis.1 The diagnosis may be made by the classic history of sudden onset of atraumatic pain and classic x-ray findings.2 The x-ray calcifications seen with HADD are not present with tenosynovitis.3 Treatment includes nonsteroidal anti-inflammatories and a splint for comfort.1^,^3 Symptoms typically improve within 4 to 7 days and resolve within 4 weeks.1 HADD has a high rate (up to 70%) of misdiagnosis, and many patients undergo unnecessary workups and surgical treatment.3
Funding and Support
By JACEP Open policy, all authors are required to disclose any and all commercial, financial, and other relationships in any way related to the subject of this article as per ICMJE conflict of interest guidelines (see www.icmje.org). The authors have stated that no such relationships exist.
Conflict of Interest
The author works as a paid medical consultant for Defibrio, a defibrillator start-up company. The author’s consulting work had no influence on this manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bernier D.Marteau E.Roulet S.Hydroxyapatite deposits of the hand and wrist: a diagnosis not to be ignored Pan Afr Med J 38202140810.11604/pamj.2021.38.408.2925334381552 PMC 8325461 · doi ↗ · pubmed ↗
- 2Dimmick S.Hayter C.Linklater J.Acute calcific periarthritis-a commonly misdiagnosed pathology Skeletal Radiol 51820221553156110.1007/s 00256-022-04006-835149896 PMC 9197888 · doi ↗ · pubmed ↗
- 3Doumas C.Vazirani R.M.Clifford P.D.Owens P.Acute calcific periarthritis of the hand and wrist: a series and review of the literature Emerg Radiol 144200719920310.1007/s 10140-007-0626-917541659 · doi ↗ · pubmed ↗