Urgent Transcatheter Mitral Edge‐to‐Edge Repair Is Associated With Worse in‐Hospital Outcomes: A Nationwide Analysis
Carlos Diaz‐Arocutipa, Cesar Joel Benites‐Moya, Javier Torres‐Valencia, Adhya Mehta, Lourdes Vicent

TL;DR
Urgent mitral valve repair is linked to worse hospital outcomes, including higher death rates and more complications, compared to non-urgent procedures.
Contribution
This study provides a nationwide analysis showing that urgent TEER is associated with significantly worse in-hospital outcomes.
Findings
Urgent TEER was linked to higher in-hospital mortality and complications like cardiogenic shock and major bleeding.
Patients undergoing urgent TEER had longer hospital stays and higher costs compared to non-urgent cases.
No significant difference was found in renal replacement therapy or pericardial complications between the groups.
Abstract
To assess in‐hospital outcomes in patients undergoing urgent versus non‐urgent transcatheter mitral edge‐to‐edge repair (TEER). We used the NIS database 2016−2019 to include admissions who underwent TEER. Inverse probability of treatment weighting (IPTW) was used to compare urgent versus non‐urgent groups. A total of 29 730 weighted admissions were included, of whom 21.6% were urgent admissions. Urgent admissions had a higher risk of in‐hospital mortality (risk ratio [RR] 3.67, 95% confidence interval [CI] 2.39−5.62), cardiogenic shock (RR 4.95, 95% CI 3.73−6.57), intra‐aortic balloon pump (RR 3.97, 95% CI 2.53−6.23), percutaneous ventricular assist device (RR 17.24, 95% CI 6.37−46.66), mechanical ventilation (RR 3.79, 95% CI 2.80−5.11), acute stroke (RR 2.56, 95% CI 1.32−4.97), in‐hospital cardiac arrest (RR 2.25, 95% CI 1.08−4.69), major bleeding (RR 5.18, 95% CI 2.97−9.06),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
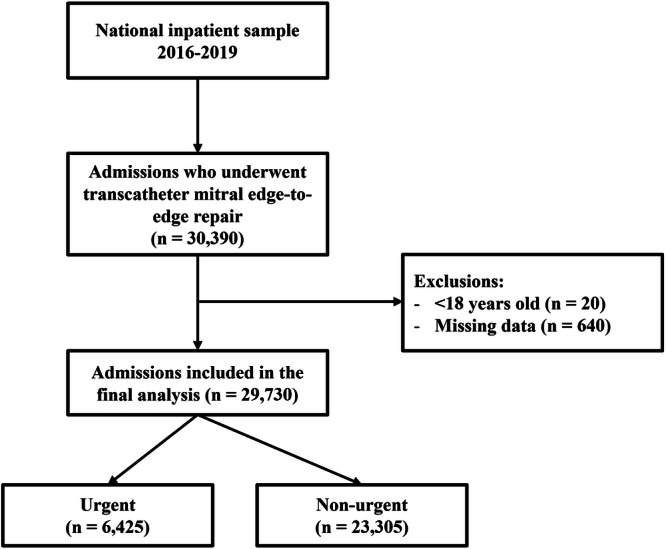 Figure 1
Figure 1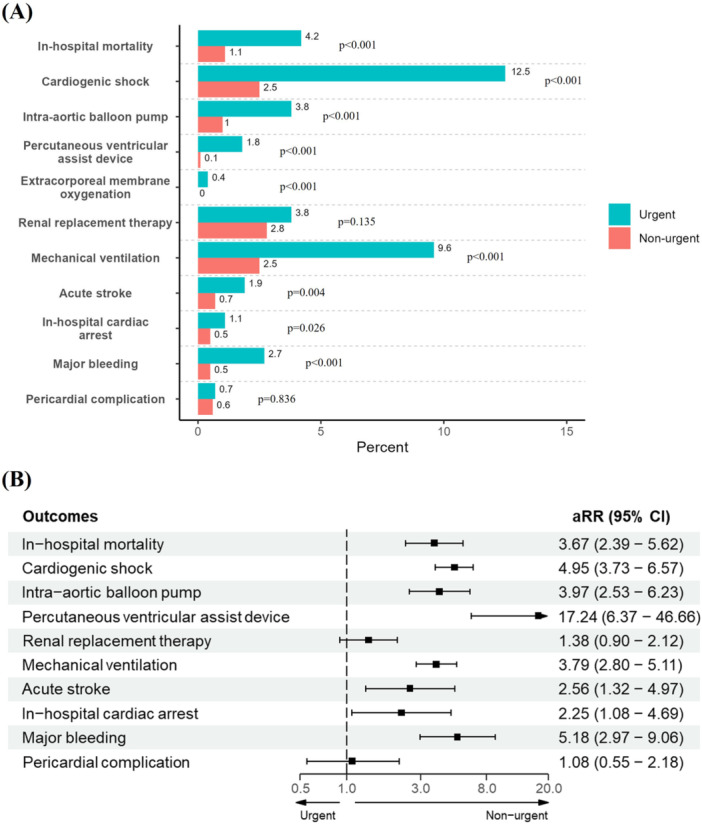 Figure 2
Figure 2| Characteristic | Overall | Type of admission | ||
|---|---|---|---|---|
| Non‐urgent | Urgent |
| ||
| Weighted admissions | 29 730 | 23 305 | 6425 | |
| Age (years) | 79 (71−85) | 79 (71−85) | 78 (69−85) | 0.196 |
| Female sex | 13 605.0 (45.8%) | 10 580.0 (45.4%) | 3025.0 (47.1%) | 0.284 |
| Race | < 0.001 | |||
| White | 23 115.0 (77.7%) | 18 430.0 (79.1%) | 4685.0 (72.9%) | |
| Black | 2375.0 (8.0%) | 1740.0 (7.5%) | 635.0 (9.9%) | |
| Hispanic | 1695.0 (5.7%) | 1185.0 (5.1%) | 510.0 (7.9%) | |
| Other | 2545.0 (8.6%) | 1950.0 (8.4%) | 595.0 (9.3%) | |
| Household income | 0.008 | |||
| Quartile 1 | 6420.0 (21.6%) | 4830.0 (20.7%) | 1590.0 (24.7%) | |
| Quartile 2 | 6860.0 (23.1%) | 5350.0 (23.0%) | 1510.0 (23.5%) | |
| Quartile 3 | 8305.0 (27.9%) | 6595.0 (28.3%) | 1710.0 (26.6%) | |
| Quartile 4 | 8145.0 (27.4%) | 6530.0 (28.0%) | 1615.0 (25.1%) | |
| Hypertension | 24 320.0 (81.8%) | 18 850.0 (80.9%) | 5470.0 (85.1%) | < 0.001 |
| Atrial fibrillation | 17 650.0 (59.4%) | 13 680.0 (58.7%) | 3970.0 (61.8%) | 0.046 |
| Dyslipidemia | 17 420.0 (58.6%) | 13,870.0 (59.5%) | 3550.0 (55.3%) | 0.006 |
| Renal failure | 11 200.0 (37.7%) | 7965.0 (34.2%) | 3235.0 (50.4%) | < 0.001 |
| Diabetes | 7655.0 (25.7%) | 5590.0 (24.0%) | 2065.0 (32.1%) | < 0.001 |
| Chronic pulmonary disease | 7640.0 (25.7%) | 5640.0 (24.2%) | 2000.0 (31.1%) | < 0.001 |
| Peripheral vascular disorders | 6720.0 (22.6%) | 5205.0 (22.3%) | 1515.0 (23.6%) | 0.345 |
| Previous PCI | 5600.0 (18.8%) | 4520.0 (19.4%) | 1080.0 (16.8%) | 0.036 |
| Previous CABG | 5585.0 (18.8%) | 4555.0 (19.5%) | 1030.0 (16.0%) | 0.004 |
| Previous myocardial infarction | 4370.0 (14.7%) | 3400.0 (14.6%) | 970.0 (15.1%) | 0.649 |
| Previous stroke | 3500.0 (11.8%) | 2715.0 (11.6%) | 785.0 (12.2%) | 0.576 |
| Previous ICD | 3370.0 (11.3%) | 2680.0 (11.5%) | 690.0 (10.7%) | 0.447 |
| Previous pacemaker | 3165.0 (10.6%) | 2515.0 (10.8%) | 650.0 (10.1%) | 0.487 |
| Elixhauser Comorbidity Index | 6.00 (4.00−7.00) | 5.00 (4.00−7.00) | 7.00 (5.00−8.00) | < 0.001 |
| Admission on weekend | 1,135.0 (3.8%) | 170.0 (0.7%) | 965.0 (15.0%) | < 0.001 |
| Expected primary payer | < 0.001 | |||
| Medicare | 24 585.0 (82.7%) | 19 285.0 (82.8%) | 5300.0 (82.5%) | |
| Medicaid | 750.0 (2.5%) | 450.0 (1.9%) | 300.0 (4.7%) | |
| Private | 3775.0 (12.7%) | 3155.0 (13.5%) | 620.0 (9.6%) | |
| Other | 620.0 (2.1%) | 415.0 (1.8%) | 205.0 (3.2%) | |
| Bed size of hospital | < 0.001 | |||
| Small | 1990.0 (6.7%) | 1440.0 (6.2%) | 550.0 (8.6%) | |
| Medium | 5630.0 (18.9%) | 4615.0 (19.8%) | 1015.0 (15.8%) | |
| Large | 22 110.0 (74.4%) | 17 250.0 (74.0%) | 4860.0 (75.6%) | |
| Location of hospital | 0.341 | |||
| Rural | 160.0 (0.5%) | 140.0 (0.6%) | 20.0 (0.3%) | |
| Urban non‐teaching | 2200.0 (7.4%) | 1755.0 (7.5%) | 445.0 (6.9%) | |
| Urban teaching | 27 370.0 (92.1%) | 21 410.0 (91.9%) | 5960.0 (92.8%) | |
| Region of hospital | < 0.001 | |||
| Northeast | 5430.0 (18.3%) | 4050.0 (17.4%) | 1380.0 (21.5%) | |
| Midwest | 5920.0 (19.9%) | 5080.0 (21.8%) | 840.0 (13.1%) | |
| South | 10 630.0 (35.8%) | 8270.0 (35.5%) | 2,360.0 (36.7%) | |
| West | 7750.0 (26.1%) | 5905.0 (25.3%) | 1,845.0 (28.7%) | |
| Ownership of hospital | < 0.001 | |||
| Government, nonfederal | 2670.0 (9.0%) | 2110.0 (9.1%) | 560.0 (8.7%) | |
| Private, non‐profit | 24 045.0 (80.9%) | 19 205.0 (82.4%) | 4840.0 (75.3%) | |
| Private, investor‐own | 3015.0 (10.1%) | 1990.0 (8.5%) | 1025.0 (16.0%) | |
| Transfer out indicator | < 0.001 | |||
| Not a transfer | 26 790.0 (90.1%) | 21 825.0 (93.6%) | 4965.0 (77.3%) | |
| Different acute care hospital | 160.0 (0.5%) | 60.0 (0.3%) | 100.0 (1.6%) | |
| Another type of health facility | 2780.0 (9.4%) | 1420.0 (6.1%) | 1360.0 (21.2%) | |
| Characteristic | Overall | Crude | Weighted | ||||
|---|---|---|---|---|---|---|---|
| Non‐urgent | Urgent |
| Non‐urgent | Urgent |
| ||
| In‐hospital mortality | 1.8% | 1.0% | 4.8% | < 0.001 | 1.1% | 4.2% | < 0.001 |
| Cardiogenic shock | 5.1% | 2.3% | 15.3% | < 0.001 | 2.5% | 12.5% | < 0.001 |
| Pulmonary artery catheterization | 12.5% | 9.4% | 23.8% | < 0.001 | 9.8% | 21.5% | < 0.001 |
| Intra‐aortic balloon pump | 1.7% | 0.9% | 4.7% | < 0.001 | 1.0% | 3.8% | < 0.001 |
| Percutaneous ventricular assist device | 0.5% | 0.1% | 1.9% | < 0.001 | 0.1% | 1.8% | < 0.001 |
| Extracorporeal membrane oxygenation | 0.2% | 0.0% | 0.6% | < 0.001 | 0.0% | 0.4% | < 0.001 |
| Renal replacement therapy | 2.7% | 2.1% | 4.7% | < 0.001 | 2.8% | 3.8% | 0.135 |
| Mechanical ventilation | 4.3% | 2.3% | 11.8% | < 0.001 | 2.5% | 9.6% | < 0.001 |
| Acute stroke | 0.9% | 0.7% | 1.6% | 0.004 | 0.7% | 1.9% | 0.004 |
| In‐hospital cardiac arrest | 0.6% | 0.5% | 1.2% | 0.005 | 0.5% | 1.1% | 0.026 |
| Major bleeding | 1.0% | 0.5% | 2.8% | < 0.001 | 0.5% | 2.7% | < 0.001 |
| Pericardial complication | 0.8% | 0.7% | 1.1% | 0.120 | 0.6% | 0.7% | 0.836 |
| Length of hospital stay (days) | 2.0 (1.0−4.0) | 2.0 (1.0−3.0) | 7.0 (3.0−14.0) | < 0.001 | 2 (1−3) | 6 (2−12) | < 0.001 |
| Total charges ($) | 176 600 (125 295−268 242) | 159 482 (119 688−236 155) | 256 961 (171 691−398 663) | < 0.001 | 164 653 (121 281−243 251) | 229 160 (154 865−344 221) | < 0.001 |
| Outcomes | Crude model | Adjusted model | ||||
|---|---|---|---|---|---|---|
| RR | 95% CI |
| RR | 95% CI |
| |
|
| ||||||
| Non‐urgent | Ref. | Ref. | ||||
| Urgent | 4.89 | 3.36−7.12 | < 0.001 | 3.67 | 2.39−5.62 | < 0.001 |
|
| ||||||
| Non‐urgent | Ref. | Ref. | ||||
| Urgent | 6.81 | 5.41−8.55 | < 0.001 | 4.95 | 3.73−6.57 | < 0.001 |
|
| ||||||
| Non‐urgent | Ref. | Ref. | ||||
| Urgent | 2.53 | 2.22−2.89 | < 0.001 | 2.19 | 1.87−2.57 | < 0.001 |
|
| ||||||
| Non‐urgent | Ref. | Ref. | ||||
| Urgent | 5.40 | 3.65−7.98 | < 0.001 | 3.97 | 2.53−6.23 | < 0.001 |
|
| ||||||
| Non‐urgent | Ref. | Ref. | ||||
| Urgent | 18.14 | 6.95−47.29 | < 0.001 | 17.24 | 6.37−46.66 | < 0.001 |
|
| ||||||
| Non‐urgent | Ref. | Ref. | ||||
| Urgent | 14.51 | 3.08−68.27 | < 0.001 | 10.93 | 2.25−53.19 | 0.003 |
|
| ||||||
| Non‐urgent | Ref. | Ref. | ||||
| Urgent | 2.21 | 1.62−3.02 | < 0.001 | 1.38 | 0.90−2.12 | 0.136 |
|
| ||||||
| Non‐urgent | Ref. | Ref. | ||||
| Urgent | 5.12 | 4.03−6.51 | < 0.001 | 3.79 | 2.80−5.11 | < 0.001 |
|
| ||||||
| Non‐urgent | Ref. | Ref. | ||||
| Urgent | 2.20 | 1.27−3.82 | 0.005 | 2.56 | 1.32−4.97 | 0.005 |
|
| ||||||
| Non‐urgent | Ref. | Ref. | ||||
| Urgent | 2.47 | 1.29−4.75 | 0.007 | 2.25 | 1.08−4.69 | 0.03 |
|
| ||||||
| Non‐urgent | Ref. | Ref. | ||||
| Urgent | 5.22 | 3.15−8.67 | < 0.001 | 5.18 | 2.97−9.06 | < 0.001 |
|
| ||||||
| Non‐urgent | Ref. | Ref. | ||||
| Urgent | 1.64 | 0.87−3.07 | 0.124 | 1.08 | 0.53−2.18 | 0.836 |
- —L.V. is funded by the Instituto de Salud Carlos III, Spain (CM20/00104 and JR22/00004).
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiac Structural Anomalies and Repair · Infective Endocarditis Diagnosis and Management
Introduction
1
Mitral regurgitation (MR) is one of the most common valvular heart diseases in the general population [1], particularly in patients with heart failure [2]. MR is a factor associated with poor prognosis, with increased mortality and hospital readmissions, especially in the presence of reduced left ventricular ejection fraction [3].
Transcatheter mitral valve edge‐to‐edge repair (TEER) has emerged as a promising alternative to surgery for patients with severe primary or secondary MR and favorable valve anatomy, particularly those considered high risk or ineligible for conventional surgery due to advanced age, significant comorbidities or anatomical constraints [4, 5]. This lesser invasive approach involves the percutaneous placement of a mitral valve clip to reduce regurgitation by approximating the mitral valve leaflets [6].
While the majority of TEER procedures are planned and performed electively to optimize patient selection and preparation [7, 8], there are scenarios where urgent intervention is required, such as acute decompensation leading to severe MR‐related symptoms, acute exacerbation of heart failure or hemodynamic instability [9]. Despite the increasing use of TEER, there is a paucity of studies in the literature specifically addressing the outcomes of urgent TEER procedures.
Previous research has highlighted the poorer outcomes associated with urgent invasive cardiovascular procedures compared to elective procedures [10]. However, the unique considerations and outcomes associated with urgent TEER remain less explored.
Using a robust data set that includes a wide range of patient demographics, clinical characteristics and procedural details, we aim to elucidate the impact of urgency on TEER outcomes. Therefore, our study aimed to compare in‐hospital outcomes in patients undergoing urgent versus non‐urgent TEER using a contemporary nationwide database.
Methods
2
We conducted a retrospective study using the National Inpatient Sample (NIS) database during the period 2016−2019. The NIS is a publicly available database of the Health Care Utilization Project, which contains data for 20% of discharge records from community hospitals across the United States. Admissions of adults who underwent in‐hospital TEER using the appropriate ICD‐10 procedure codes were included (Supporting Information S1: Table 1). Admissions with missing data for covariates were excluded. Patients were divided into two groups, urgent and non‐urgent TEER, for comparison. For the definition of the type of TEER procedure (urgent vs. non‐urgent), we used the variable “ELECTIVE” from the NIS database which has two categories: non‐elective versus elective admission.
The primary outcome was in‐hospital mortality, and the secondary outcomes were cardiogenic shock, pulmonary artery catheterization, intra‐aortic balloon pump (IABP), percutaneous ventricular assist device (PVAD), extracorporeal membrane oxygenation (ECMO), renal replacement therapy, mechanical ventilation, acute stroke, major bleeding, pericardial complication, length of hospital stay, and total charges (Supporting Information S1: Table 1). Sociodemographic characteristics, comorbidities (based on Elixhauser Comorbidity Index), and hospital characteristics were reported.
Categorical variables were expressed as frequencies and percentages and continuous variables as median (interquartile range [IQR]). A chi‐squared test with Rao & Scott's second‐order correction and Wilcoxon rank‐sum test were used to compare categorical and continuous variables, respectively. Inverse probability of treatment weighting (IPTW) was used to assess the differences between urgent and non‐urgent groups, balancing demographics, comorbidities, and hospital characteristics. The balance of baseline covariates was compared using the standardized mean difference (cut‐off < 0.1 for appropriate balance) (Supporting Information S1: Figure 1). A log‐binomial model was used to estimate the adjusted risk ratios (aRR) with their 95% confidence intervals (CI). In addition, we performed a trend analysis on cases of TEER and urgent admissions, examining quarterly data each year using the Cochran‐Armitage Trend Test. The R 4.3.2 software was used for all analyses, considering a two‐tailed p < 0.05 as statistically significant.
Results
3
Demographics and Characteristics
3.1
This study involved 30 390 weighted admissions of adults who underwent TEER. Of these, 29 730 were included in the final analysis, with 6425 (21.6%) classified as urgent admissions (Figure 1). The median age of the cohort was 79 years (IQR 71−85), with 45.8% being female and 77.7% identifying as white (Table 1). The most prevalent comorbidities among this cohort were hypertension (81.8%), atrial fibrillation (59.4%), and dyslipidemia (58.6%). Patients with urgent admissions exhibited a higher comorbidity burden, particularly in extracardiac conditions such as renal failure (50.4% vs. 34.2%), diabetes (32.1% vs. 24%), and chronic pulmonary disease (31.1% vs. 22.3%), all of which were statistically significant differences (p < 0.001). The median Elixhauser Comorbidity Index was also higher in the urgent admission group (7.00 vs. 5.00, p < 0.001).
Flow diagram for the selection of study participants.
Procedures and Outcomes
3.2
The median length of stay for all admissions was 2 days (IQR 1−4), with a majority of procedures conducted in large urban teaching hospitals. Notably, a higher proportion of urgent admissions were transferred to another hospital (21.2% vs. 6.1%, p < 0.001) (Table 2).
The overall in‐hospital mortality rate for TEER admissions was 1.8%, with urgent admissions demonstrating a significantly higher in‐hospital mortality rate after IPTW adjustment (aRR 3.67, 95% CI 2.39–5.62) compared to non‐urgent admissions (Table 2, Table 3, and Figure 2). Similarly, patients admitted urgently were at a higher risk of developing cardiogenic shock (aRR 4.95, 95% CI 3.73−6.57), acute stroke (aRR 2.56, 95% CI 1.32−4.97), and compared to non‐urgent admissions, in‐hospital cardiac arrest (aRR 2.25, 95% CI 1.08−4.69) and major bleeding (aRR 5.18, 95% CI 2.97−9.06) were also more frequent among urgent admissions (Table 3 and Figure 2).
(A) Adjusted proportions and (B) adjusted relative risks for primary and secondary outcomes according to urgent and non‐urgent groups. aRR = adjusted relative risk; CI = confidence interval.
Furthermore, the utilization of invasive procedures was more common among urgent‐TEER patients, including IABP (aRR 3.97, 95% CI 2.53−6.23), PVAD (aRR 17.24, 95% CI 6.37−46.66), and mechanical ventilation (aRR 3.79, 95% CI 2.80−5.11) (Figure 2). No significant difference was observed between the two groups with respect to renal replacement therapy and pericardial complications (Table 3 and Figure 2). Urgent admissions were associated with longer median length of stay (median 6 vs. 2 days, p < 0.001) and higher total costs (median 164 653, p < 0.01) compared to non‐urgent admissions (Table 2).
A statistically significant increase in the utilization of TEER was observed over time (p < 0.001), while the proportion of urgent admissions remained unchanged across the study period (p = 0.652) (Supporting Information S1: Figure 2). Likewise, there was no temporal change in the length of hospital stay (p = 0.425) and total charges (p = 0.950) (Supporting Information S1: Table 2).
Discussion
4
In this nationwide study, we found that urgent admissions represented nearly a quarter of all cases of patients undergoing TEER. Inpatients undergoing urgent TEER had a higher risk of in‐hospital mortality, an increased requirement of mechanical circulatory support, and other in‐hospital complications, along with a higher utilization of hospital resources.
MR plays a significant role in the setting of acute decompensated heart failure, both in terms of its frequency and its impact on prognosis [3, 11]. Given the relevance of MR and the risk profile of patients with acute HF, the approach of performing a less invasive therapeutic option such as TEER is of interest [11, 12]. Our study has documented an increased risk of adverse clinical events associated with the performance of TEER procedures in an emergency setting. Similar results were observed in patients undergoing cardiac surgery in terms of a worse outcome of urgent interventions. In this urgent group, a previous study found that those who received surgical mitral valve repair had a somewhat lower risk of mortality and complications than those who underwent mitral valve replacement surgery [13]. The question remains as to whether the prognosis of these patients can truly be improved with TEER in this emergency setting compared to medical treatment alone [14].
Previous studies have shown mixed results for urgent versus non‐urgent TEER in the short‐ and long‐term [15, 16, 17, 18]. Al‐khadra et al. used administrative data and found no significant differences in in‐hospital mortality (4.4% vs. 2.8%, p = 0.051) and cardiac complications between the two groups after propensity score matching [15]. Similarly, a study conducted in Spain on 85 patients with degenerative and functional MR reported no differences in mortality, MR reduction, and improvement in the New York Heart Association class at 30 days between urgent and non‐urgent TEER [16]. Furthermore, mortality was similar between both groups at a 2‐year follow‐up (17.6% vs. 25.1%, p = 0.864). In contrast, in a more recent NIS cohort (2016−2017), in‐hospital mortality was found to be significantly higher in urgent versus non‐urgent TEER (4.5% vs. 1.6%, p < 0.001) [18]. Overall, these discrepancies can be explained by the use of different ICD‐10 codes to define the TEER, the type of analysis employed (crude vs. confounder‐adjusted), the study period considering the recent approval of the MitraClip device and the experience of the operators performing the procedure.
It is reasonable to assume that patients undergoing urgent TEER present a higher‐risk profile compared to those with non‐urgent indications [7, 8, 19]. This higher‐risk profile likely encompasses multiple factors beyond comorbidities alone. The observed increase in mortality and complication rates among patients undergoing urgent TEER may be attributed to the more severe clinical status at the time of intervention. We found that patients requiring urgent TEER often present with acute decompensation of heart failure and significant hemodynamic instability with cardiogenic shock in 12%, necessitating prompt intervention. These clinical factors, including the severity of MR, left ventricular dysfunction, and associated comorbidities may impact procedural outcomes [20, 21]. Factors such as hemodynamic instability, organ dysfunction, and the need for mechanical circulatory support can contribute to increased peri‐procedural risks and post‐procedural complications [13, 17].
Clinical Implications
5
It is essential to optimize the clinical situation of patients before the TEER procedure, if possible, particularly in those with urgent admissions. A recent study observed that in patients with MR following acute myocardial infarction, cardiogenic shock was not a factor associated with a worse outcome. This work highlighted the importance of achieving hemodynamic stability as a primary goal before TEER, if this is feasible [22]. Also, a further study demonstrated that patients with cardiogenic shock and MR who underwent TEER exhibited acceptable survival and procedural success [20]. However, it is highly advisable to exercise caution when interpreting these results, as they are likely to be selected cases.
Our study highlights the importance of robust risk stratification tools to identify patients at higher risk of adverse outcomes when undergoing urgent TEER. Factors such as comorbidities, hemodynamic stability, and severity of MR should be carefully evaluated to guide treatment decisions and improve patient's optimization before and after TEER [19, 21].
The optimal timing of interventions is a crucial consideration. The decision to perform TEER urgently versus electively should be informed by a comprehensive assessment of individual patient characteristics, including the severity of symptoms, hemodynamic status, and overall clinical stability. Balancing the potential benefits of early intervention with the inherent risks associated with urgent procedures is crucial. A multidisciplinary approach involving cardiologists, cardiac surgeons, and other specialists is often required for the management of patients with severe MR [23]. It is crucial that these teams work together to conduct a thorough risk assessment, develop an effective treatment plan, and provide comprehensive care following the procedure [24].
The majority of TEER procedures were conducted in large urban teaching hospitals, indicating a concentration of specialized care in these settings. Interestingly, while there was an overall increase in TEER utilization over time, the proportion of urgent admissions remained stable, suggesting consistent patient selection criteria for urgent interventions.
It should be noted that our study has certain limitations, primarily due to the retrospective design and reliance on administrative data. There is a possibility that unmeasured confounding variables may have influenced our findings. Furthermore, important clinical parameters such as MR etiology, echocardiographic or hemodynamic data, specific TEER implant characteristics, and medication usage during hospitalization were not captured in our analysis. Additionally, the short‐term nature of our study precludes assessment of long‐term outcomes.
Conclusions
6
In conclusion, adult inpatients undergoing urgent TEER implantation had an increased risk of in‐hospital death and other short‐term complications. However, prospective multicenter studies evaluating long‐term outcomes are required to guide the care of patients with severe MR requiring urgent intervention.
Author Contributions
Carlos Diaz‐Arocutipa involved in concept/design. Carlos Diaz‐Arocutipa involved in data acquisition. Carlos Diaz‐Arocutipa, Cesar Joel Benites‐Moya, Javier Torres‐Valencia, Adhya Mehta, and Lourdes Vicent involved in data analysis/interpretation. Carlos Diaz‐Arocutipa and Lourdes Vicent drafted the article. Cesar Joel Benites‐Moya, Javier Torres‐Valencia, and Adhya Mehta critically revised the article. Carlos Diaz‐Arocutipa, CBM, Javier Torres‐Valencia, Adhya Mehta, and Lourdes Vicent approved the article.
Ethics Statement
Not applicable because only information from published studies was used.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Supporting information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1V. T. Nkomo , J. M. Gardin , T. N. Skelton , J. S. Gottdiener , C. G. Scott , and M. Enriquez‐Sarano , “Burden of Valvular Heart Diseases: A Population‐Based Study,” Lancet 368, no. 9540 (2006): 1005–1011.16980116 10.1016/S 0140-6736(06)69208-8 · doi ↗ · pubmed ↗
- 2A.‐C. Martin , M.‐C. Bories , N. Tence , et al., “Epidemiology, Pathophysiology, and Management of Native Atrioventricular Valve Regurgitation in Heart Failure Patients,” Frontiers in Cardiovascular Medicine 8 (2021): 713658.34760937 10.3389/fcvm.2021.713658 PMC 8572852 · doi ↗ · pubmed ↗
- 3S. Arora , K. Sivaraj , M. Hendrickson , et al., “Prevalence and Prognostic Significance of Mitral Regurgitation in Acute Decompensated Heart Failure,” JACC: Heart Failure 9, no. 3 (2021): 179–189.33309575 10.1016/j.jchf.2020.09.015PMC 8075289 · doi ↗ · pubmed ↗
- 4T. A. Mc Donagh , M. Metra , M. Adamo , et al., “2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure,” European Heart Journal 42, no. 36 (2021): 3599–3726.34447992 10.1093/eurheartj/ehab 368 · doi ↗ · pubmed ↗
- 5A. Vahanian , F. Beyersdorf , F. Praz , et al., “2021 ESC/EACTS Guidelines for the Management of Valvular Heart Disease,” European Heart Journal 43, no. 7 (2022): 561–632.34453165 10.1093/eurheartj/ehab 395 · doi ↗ · pubmed ↗
- 6J. Hausleiter , T. J. Stocker , M. Adamo , N. Karam , M. J. Swaans , and F. Praz , “Mitral Valve Transcatheter Edge‐to‐Edge Repair,” Euro Intervention 18, no. 12 (2023): 957–976.36688459 10.4244/EIJ-D-22-00725 PMC 9869401 · doi ↗ · pubmed ↗
- 7G. W. Stone , J. Lindenfeld , W. T. Abraham , et al., “Transcatheter Mitral‐Valve Repair in Patients With Heart Failure,” New England Journal of Medicine 379, no. 24 (2018): 2307–2318.30280640 10.1056/NEJ Moa 1806640 · doi ↗ · pubmed ↗
- 8J.‐F. Obadia , D. Messika‐Zeitoun , G. Leurent , et al., “Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation,” New England Journal of Medicine 379, no. 24 (2018): 2297–2306.30145927 10.1056/NEJ Moa 1805374 · doi ↗ · pubmed ↗