Effects of Tailored Rehabilitation Strategies in a Conservatively Managed Traumatic Brachial Plexus Injury in a 27-Year-Old Male Patient: A Case Report
Anjali Rai, Raghumahanti Raghuveer, Nikita Gangwani, Pradhyum D Kolhe

TL;DR
This case report describes the rehabilitation of a 27-year-old man with traumatic brachial plexus injury and other injuries after a traffic accident.
Contribution
The paper presents a tailored rehabilitation approach for a complex TBPI case with polytrauma.
Findings
The patient showed progressive improvement in range of motion, strength, and endurance.
Multi-sensory strategies and graded motor imagery were effective in enhancing neuromuscular control.
The rehabilitation program offers a reference for early treatment strategies in similar cases.
Abstract
Traumatic brachial plexus injury (TBPI) is a serious neurological condition most often resulting from trauma. This condition is among the most debilitating injuries affecting the upper limb. The injury is typically categorized as preganglionic or postganglionic based on the site of trauma, proximal to or distal to the dorsal root ganglion (DRG). TBPI results in movement deficits of the upper limb with impaired muscle strength and sensitivity. This case report details the extensive rehabilitation of a 27-year-old male patient who was involved in a road traffic accident, resulting in injuries to the left upper extremity characterized by a loss of motor function and sensation. Additionally, the incident caused injuries to the left lower extremity, leading to a mid-shaft femur fracture and fractures of the metatarsals. The patient received a comprehensive clinical evaluation, along with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
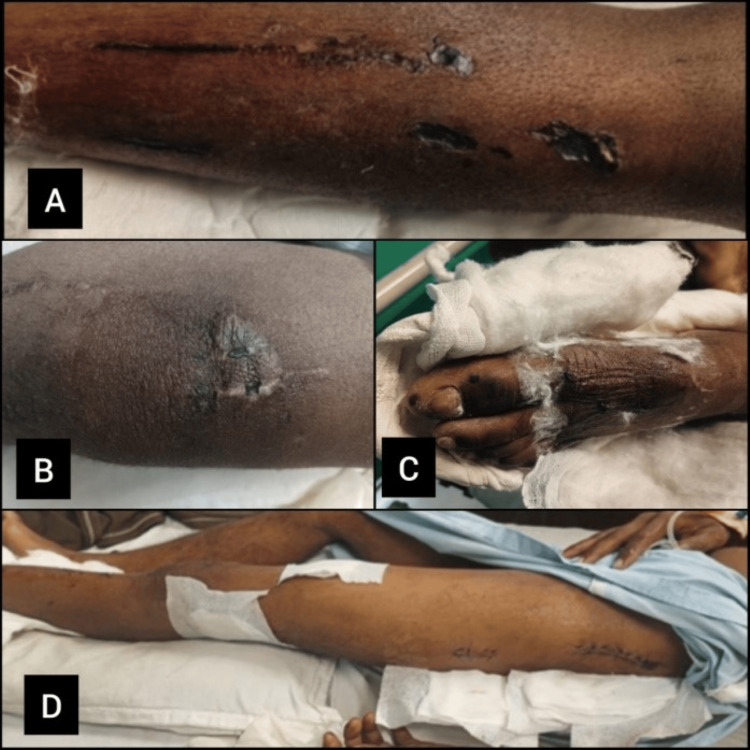 Figure 1
Figure 1 Figure 2
Figure 2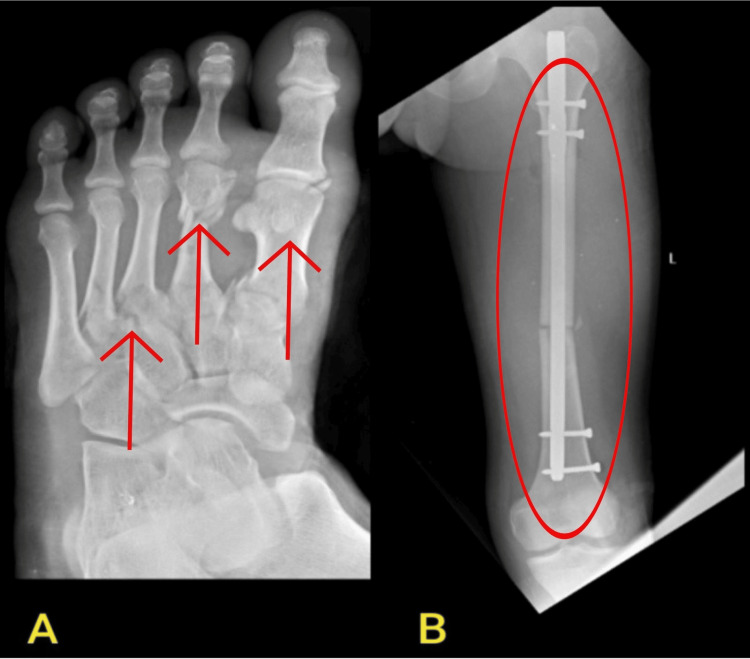 Figure 3
Figure 3| Dates | Events |
| 6/03/24 | Met with a road traffic accident |
| 6/03/24 | Brought to AVBRH casualty with loss of consciousness |
| 6/03/24 | Regained consciousness and was shifted to a ward and medications were prescribed |
| 7/03/24 | X-ray of the left lower extremity was done |
| 12/03/24 | ORIF with femur interlock nailing was done |
| 15/03/24 | MRI cervical spine and MRI of the brachial plexus |
| 13/03/24 | A physiotherapy call was given |
| Movement | Right | Normal | Left |
| Hip flexion with knee flexion | 0-120° | 120-140° | 0-50° |
| Hip flexion with knee extension | 0-900° | 90° | 0-45° |
| Hip extension | 0-25° | 0-30° | 0-10° |
| Hip abduction | 0-40° | 40-45° | 0-15° |
| Hip adduction | 0-25° | 20-25° | 0-20° |
| Hip internal rotation | 0-40° | 30-45° | NA |
| Hip external rotation | 0-40° | 35-50° | NA |
| Knee flexion | 0-130° | 0-135° | 0-20° |
| Knee extension | 135-0° | 135-0° | 20-0° |
| Ankle plantarflexion | 0-50° | 45-55° | 0-20° |
| Ankle dorsiflexion | 0-20° | 15-20° | 0-5° |
| Ankle inversion | 0-30° | 30-35° | 0-15° |
| Ankle eversion | 0-15° | 15-20° | 0-5° |
| Shoulder flexion | 0-170° | 0-180° | 0-5 (trick movement) |
| Shoulder extension | 0-45° | 0-50° | 0-5 (trick movement) |
| Shoulder abduction | 0-170° | 0-180° | 0 |
| Shoulder adduction | 170-0° | 180-0° | 0 |
| Shoulder internal rotation | 0-80° | 0-90° | 0 |
| Shoulder external rotation | 0-80° | 0-90° | 0 |
| Elbow flexion | 0-130° | 0-140° | 0 |
| Elbow extension | 135-0° | 140-0° | 0 |
| Wrist flexion | 0-65° | 0-75° | 0 |
| Wrist extension | 0-65° | 0-70° | 0 |
| Reflex | Nerve | Right | Left |
| Biceps (C5-C6) | Musculocutaneous | ++ | Absent |
| Supinator (C5-C6) | Radial | ++ | Absent |
| Triceps (C7-8) | Radial | ++ | Absent |
| Finger flexion (C7-8) | Median and ulnar nerve | ++ | Absent |
| Knee (L2-4) | Femoral | ++ | N/A |
| Abdominal (T6-T12) | Thoracic spine nerve roots | ++ | ++ |
| Plantar | Sacral nerve | Flexion | Flexion |
| Nerve | Test | Findings |
| Dorsal scapular nerve (C5) | Asking the patient to retract the shoulder and/or elevate the shoulder | The patient was able to perform shoulder elevation |
| Long thoracic nerve (C5-C7) | Wall push-up test for serratus anterior test | The patient was unable to perform the test |
| Suprascapular nerve (upper trunk of BP) | Ask the patient to abduct the shoulder | The patient was unable to perform an abduction |
| Posterior cord nerve (upper subscapular nerve, thoracodorsal nerve, lower subscapular nerve) | Subscapularis muscle: (1) Test: Lift off test. (2) Test: Belly press test | (1) The patient was unable to lift the hand off the lower back. (2) The patient was unable to perform the test |
| Latissimus muscle: Abduct the arm and then ask the patient to adduct the arm against resistance | The patient was unable to perform the adduction | |
| Teres major: Adducting the elevated arm against resistance | The patient was unable to perform the adduction | |
| Teres minor: Horn blowers test (the patient's elbow is flexed 90 degrees, and then the patient is asked to rotate the shoulder) | The patient was unable to perform shoulder rotation | |
| Lateral pectoral nerve (lateral cord) | Ask the patient to perform shoulder flexion, adduction, and Internal rotation) | The patient was unable to perform movement |
| Musculocutaneous nerve (C5-C7) | Flexion and adduction of the shoulder joint, flexion and supination of the elbow joint | The patient was not able to perform movements |
| Axillary nerve (C6-C8) | Lateral and external rotation | The patient was not able to perform |
| Radial nerve (C6-C8) | Extension of elbow joint, wrist extension, finger extension | The patient was unable to perform |
| Median nerve (C5-T1) | Wrist and finger flexion, opposition, flexion, and abduction of the thumb | The patient was unable to perform |
| Ulnar nerve (C8-T1) | Froment’s sign | The patient was unable to perform |
| Goals | Intervention | Rationale | Dosage |
| To develop strategies to manage and cope with pain or discomfort | Patient and caregiver education | Educate the patient about his condition, potential complications, and preventive strategies, as well as the physiotherapy protocol to be followed | - |
| To prevent complications of joint contracture and subluxation | Immobilization through sling or hemi-sling/Elpeau’s bandaging | To prevent joint contracture and uncontrolled limb motion or positions, as well as minimize glenohumeral subluxation | Throughout the day |
| To prevent muscle de-conditioning | Active cervical retraction with the patient sitting with scapulae retracted and unilateral scapular circles | For improving stability and facilitating motor re-education and scapular synergy | 10-15 times, with 5 seconds hold |
| To reduce inflammation and edema and to facilitate nerve regeneration | Low-intensity laser therapy over nerve roots C5, C6, C7, and T1 | It reduces pain and swelling and can progressively improve nerve function | Wavelength, 780 nm power, 250 mV, 450 J/mm2 for 20 minutes |
| To regain neuromuscular control | Joint compression technique. Lateralization training. Rood’s facilitatory technique uses cotton balls (slow-light touch) and rotatory brush (fast brushing) on respective. Sensory re-education with different textures, such as sandpaper, silk, and net). Motor re-education through PNF rhythmic initiation Technique (active assisted D1-D2 flexion/extension) and range of motion exercises of bilateral upper extremity | To improve proprioception, joint stability, and muscle tone. It also enhances limb position awareness, improves motor function, and increases joint stability. Used for implicit motor imagery. This technique increases the modulation of muscle spindle sensitivity to increase muscle activity and regain motor control. For the re-establishment of impaired afferent sensory pathways or to restore sensory integration. To stimulate and improve neuromuscular control and to restore voluntary and active range of motion | 10 repetitions with 30-second holds. 5-10 minutes twice daily. 3-5 times, followed by a 30-second break. 3-5 times, followed by a 30-second break. 10 repetitions of 2 sets |
| To reduce pain and swelling to promote healing and comfort of the lower extremities | Cryotherapy (icing with isometrics of quadriceps). Bandaging around the thigh and shin. Elevation of the affected limb | Reduces pain and swelling by constricting blood vessels, enhancing comfort, & aiding early mobilization. Bandaging supports the limb, prevents swelling, improves venous return, reduces edema, and stabilizes the limb. Elevating the affected limb twice daily and for 7-8 hours during rest promotes venous return, reduces fluid buildup, decreases swelling and pain, and improves rehabilitation effectiveness | For 10-15 minutes twice a day. For 7-8 hours (when the patient is resting). For approximately 7 hours (when the patient is resting) |
| To enhance the strengthening of quadriceps and hip abductors | Strengthening the quadriceps sets with holds. Hamstring sets with holds. Gluteus maximus set with holds | It strengthens and tones the quads for daily activities like walking, stairs, and standing. The hamstring strengthens back thigh muscles, aiding in knee bending, hip extension, and overall stability during various movements. The glute holds target hip extension and stability, enhancing strength for improved walking, running, and standing | 10 repetitions of 2 sets with hold of 10 seconds each |
| To restore full-knee extension to maintain joint mobility and prevent long-term stiffness or contractures | Range-of-motion open kinetic chain exercise: Straight leg raise (in multiple angles), heel slides, prone knee bending, terminal extension in sitting | The range of motion exercises aim to improve flexibility, joint mobility, and functional movement through exercises | 10 repetitions of 2 sets with hold of 10 seconds each |
| To maintain the flexibility of the affected extremity | Stretching the hamstring muscle gastrocnemius and soleus | The hamstring stretch improves knee and hip flexibility, while the gastrocnemius and soleus stretch enhances ankle flexibility and gait efficiency | 30 seconds hold of 3 sets |
| To facilitate a return to normal walking patterns and promote early mobility to prevent complications associated with prolonged immobility | Gait training: Initiate with non-weight bearing with a walker, progress to partial weight bearing (25%) in 2 weeks | Gait training starts with non-weight bearing using a walker for safety, progressing to 25% weight bearing after two weeks to stimulate healing and improve strength and balance, aiding transition to normal gait | Hallway ambulation |
| Goals | Intervention | Rationale | Dosage |
| To enhance recovery of motor function: Retard muscle weakness/wasting and promote muscle re-education | Electrical stimulation, long duration 300 ms interrupted galvanic (IG) stimulation at each motor point | Used for motor relearning and to elicit contraction of targeted muscle/nerve. It also promotes nerve healing and regeneration | 30 contractions at each motor point |
| Gradual restoration of upper extremity strength and endurance | Graded motor imagery technique includes imagination of movements without performing them and mirrors visual feedback | Used to facilitate motor control. It provides immediate feedback and facilitates re-learning through visual and auditory feedback | Each movement, 10 times twice a day |
| Implement strategies for sensory and motor re-education | Sensory re-education utilizing a sensory kit that corresponds to the dermatomal distribution, incorporating various textures and shapes, both with the eyes open and closed | For re-establishment of impaired afferent sensory pathways or to restore sensory integration and to accelerate sensorimotor recovery | 3-5 times, followed by a 30-second break for each dermatome distribution |
| Restoration of functions as soon as neural regulation takes place | Rood's facilitatory approach with (fast tapping over the muscle belly) | For facilitating and re-educating muscles to gain voluntary muscular contractions | 10 repetitions of 2 sets |
| Improving joint mobility: Restore and enhance the range of motion in the affected joints | Wall slides terminal knee extension on Swiss ball patellar mobilization and Mulligan-Bent leg raises for hamstring mobility. Standing - hip flexion, hip extension, hip abduction, hip adduction (without resistance), standing leg curls | The protocol comprises mobility-enhancing exercises. Exercises such as wall slides, terminal knee extension on a Swiss ball, patellar mobilization, Mulligan-Bent leg raise, standing hip flexion, extension, abduction, and adduction, along with standing leg curls, target specific muscle groups to improve joint flexibility, stability, and overall lower limb function, aiding in injury prevention and promoting functional movement patterns | 10 repetitions of 2 sets |
| Improving muscular strength: Rebuild and strengthen the muscles surrounding the affected area | Strengthening the quadricep fixation hamstring curl in standing VMO strengthening. Standing - hip flexion, hip extension, hip abduction, hip adduction (with resistance). Muscle energy technique for quadriceps and the hamstring | The strengthening protocol consists of quadricep fixation for knee stability, hamstring curl in standing for lower limb strength, VMO strengthening for patellar stability, and standing hip flexion, extension, abduction, and adduction with resistance for hip muscle strength and mobility. Additionally, muscle energy technique for the quadriceps and hamstring improves muscle strength, flexibility, and neuromuscular control, contributing to rehabilitation and injury prevention | 10 repetitions of 2 sets |
| Retaining function of physiological movement pattern while walking | Gait training: Initiate partial weight bearing 50-75% with a walker | Initiating gait training with partial weight bearing (50-75%) using a walker for 2-3 rounds in the hallway ensures stability, balance, and confidence, promoting muscle memory and functional recovery for independent ambulation | 2-3 rounds in the hallway |
| To regain neuromuscular coordination and strength | Balance training: Single limb standing. Step-up and step down and stepping sideways | Balance training with single-limb standing, step-ups, and side steps enhances proprioception, stability, and neuromuscular control, reducing fall risk and improving functional mobility | 10 repetitions of 2 sets |
| Promote resorption of the bone and improve endurance: Enhance the natural process of bone resorption to facilitate bone remodeling | Endurance training: Stationary bicycling - in a clockwise direction, as well as an anticlockwise direction | Stationary bicycling in both clockwise and anticlockwise directions for 15 minutes enhances cardiovascular endurance and promotes balanced muscle development | 15 minutes |
| Goals | Intervention | Rationale | Dosage |
| Regain strength and neuromuscular control to facilitate motor re-education | The AO-PNS technique involves the observation of actions accompanied by peripheral nerve stimulation, showcasing a repetitive movement pattern while electrical stimulation is administered | Electrical stimulation not only promotes motor re-education but also facilitates axon growth during the process of nerve repair, thereby expediting motor recovery | 10 repetitions of 2 sets |
| Foster a proactive approach to health and wellness, incorporating regular exercise and preventive measures, for the gradual restoration of movements | Kinesiotherapy exercises are conducted in positions that eliminate or reduce the effects of gravity, with a gradual increase in training intensity using light weights, ultimately advancing to an antigravity position | To maintain and promote range of motion, joint integrity, and strength. To rehabilitate and enhance mobility, endurance, and strength | 10 repetitions of 2 sets |
| Promote strengthening | Isometrics contractions of shoulder flexion, external/internal rotations, adduction and abduction | To enhance muscle activation, as well as promote strengthening | 5 repetitions each with 30 seconds of hold |
| Restoration of muscular strength: Rebuild and enhance muscle strength to support overall function and prevent re-injury | Strengthening exercises: Lower limb heel raises with holds toe raises with holds forward and backward lunges (initially without weights, progresses to with weights), squats (initially without weights, progresses to with weights), clamshell abduction/adduction with a resistance band | Lower limb strengthening exercises enhance stability and strength for weight-bearing activities, while core and pelvic exercises improve overall stability, posture, and functional movement, aiding injury prevention and daily performance | 10 repetitions of 2 sets |
| Optimization of core and pelvic stability: Strengthen the core and pelvic muscles to provide a stable foundation for all movements and reduce the risk of injury | Core and pelvic strengthening: Glute bridge with holds, glute bridge with abduction/adduction core strengthening with isometric holds | The core and pelvic strengthening exercises aim to improve overall stability, posture, and functional movement patterns, aiding in injury prevention and promoting optimal performance in daily activities | 10 repetitions of 2 sets |
| Optimization of coordinated movement patterns along the kinematic chain during movement | Balance training: (1) Static balance: Single-leg stands, tandem stance, beginning with stable surfaces and progressing to unstable surfaces (balance boards, foam pads). (2) Dynamic balance: Single-leg stands with reach and step-ups on unstable surfaces, progressing to dynamic movements like hopping or step-ups on unstable surfaces | Balance training progresses from static exercises like single-leg stands to dynamic movements on unstable surfaces, enhancing stability, coordination, and strength for injury prevention and better daily and sports performance | 10-20 seconds hold, 2-3 sets, 2-3 times per week |
| Developing ergonomic postures, gait, and movements in everyday routine: To promote safe and efficient postures and movements in daily activities to prevent strain and injury | Gait training: Initiate full weight bearing without a walker | Initiating full weight bearing without a walker allows for gradual adaptation to weight bearing, promoting confidence and independence in ambulation | 2 rounds initially, increase according to patient’s convenience |
| Outcomes | Day 1 assessment | After 1month | After 2months |
| VAS | On rest: 5/10 | On rest: 4/10 | On rest: 1/10 |
| On activity: 8/10 | On activity: 6/10 | On activity: 2/10 | |
| ROM (lower extremity) | |||
| Hip flexion | 0-50° | 0-80° | 0-110° |
| Hip extension | 0-10° | 0-20° | 0-30° |
| Hip abduction | 0-15° | 0-30° | 0-40° |
| Hip adduction | 15-0° | 30-0° | 0-40° |
| Knee flexion | 0-20° | 0-60° | 0-100° |
| Knee extension | 20-0° | 60-0° | 100-0° |
| Ankle plantarflexion | 0-20° | 0-30° | 0-40° |
| Ankle dorsiflexion | 0-5° | 0-15° | 0-20° |
| MMT (affected side) | |||
| Lower extremity | 2/5 | 3+/5 | 4/5 |
| MMT (affected side) | |||
| Shoulder flexors | 1/5 | 1+/5 | 1+/5 |
| Shoulder extensors | 0/5 | 1/5 | 1+/5 |
| Shoulder abductors | 0/5 | 1/5 | 1+/5 |
| Shoulder adductors | 0/5 | 1/5 | 1+/5 |
| Barthel index | 30/100 | 50/100 | 80/100 |
| Lower extremity functional scale | 10/100 | 40/00 | 60/100 |
| BPOM | 13 | 16 | 20 |
| UEFS | 4 | 12 | 24 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNerve Injury and Rehabilitation · Spinal Cord Injury Research · Pain Management and Treatment
Introduction
Brachial plexus injury (BPI) is classified as a serious peripheral nerve injury that results in functional impairments of the upper limb and considerable disability in individuals of all ages, including both adults and children. It exerts a substantial influence, resulting in serious and enduring restrictions on arm functionality, thereby impacting daily activities and the overall quality of life for individuals affected [1]. Brachial nerve complex injuries vary in severity and etiology, spanning from mild to severe. Regrettably, traumatic cases of BP injuries are increasing, resulting in significant social and financial burdens and profoundly impacting individuals' quality of life [2]. The occurrence of BPIs has seen a considerable rise, largely attributed to the increase in high-velocity motor vehicle collisions in the 20th and 21st centuries [1]. It is estimated that motorcycle accidents, sporting incidents, or industrial accidents account for 44%-70% of all traumatic BPI (TBPIs). Specifically, 22% of motorcycle injuries result in BPI, accounting for approximately 4.2% of cases [3]. BPIs can result from various factors, including contact sports, automobile accidents, and birth complications. These injuries are broadly categorized into traumatic causes, such as car accidents and contact sports, and non-traumatic causes, such as obstetric palsy. The sensitive neural network can be damaged by stretching, compression, and laceration. Traumatic injuries can be categorized as either closed or open, based on the mechanism that caused them [3]. Closed injuries typically result from stretching or traction forces that violently pull the head and neck away from the shoulder, while open injuries are commonly the result of gunshot or stab wounds [4].
Traumatic injuries to the brachial plexus have a profound impact on the functionality of the upper limb and can result in disability. Common symptoms associated with such injuries may include restricted movement of the upper limb, as well as reduced muscle strength and sensitivity [5]. BPI is fundamentally categorized into preganglionic and postganglionic types, making the early determination of the injury level crucial for choosing the correct treatment strategy [6]. BPIs are categorized based on their distance from the dorsal root ganglion (DRG): postganglionic lesions are considered distal, while preganglionic lesions are deemed proximal. Both types, irrespective of their location, result in a loss of muscular function. Preganglionic injuries cause the nerve to be detached from the spinal cord, separating motor nerve fibers from motor cell bodies in the anterior horn cells. Lesions affecting postganglionic neurons result in the impairment of both motor and sensory nerve cells, causing disruptions in motor action potentials, as well as sensory nerve action potentials (SNAPs) [6].
Recent advances in the management of BPI have recently enhanced the outlook for functional motor recovery [7]. This encompasses conservative management, which is non-surgical, as well as non-conservative management, which involves surgical interventions. The latter includes procedures such as neurolysis, nerve repair, the application of nerve grafts, and nerve transfer, in addition to palliative surgical techniques aimed at achieving optimal functional outcomes. These may involve tendon transfer, functioning-free muscle transplantation, and arthrodesis [8]. In instances of open BPI wounds, prompt surgical intervention is essential. Conversely, for closed BPI wounds, provided that there are no other urgent injuries, immediate surgical repair may not be necessary. This approach involves assessing the condition, addressing pain management, and initiating rehabilitation. In cases where functional recovery or neurological improvement is insufficient, surgical intervention may be contemplated after a period of three to six months. This timeframe provides an opportunity to evaluate the likelihood of natural recovery and to identify the most suitable strategy for achieving the best long-term results [9]. Conservative treatment for BPI includes extensive physical and occupational rehabilitation. Commonly used techniques are joint mobilization, neurosensory motor stimulation, kinesio-taping, electrostimulation, splint immobilization, multi-sensory strategies, and graded motor imagery [10]. A collaborative approach with families is essential, which includes teaching and training them to maintain interventions at home.
Rehabilitation is essential for recovery after a BPI or trauma, with early intervention recommended to limit the risk of further complications. Therapists play an important role in helping patients return to work by making a favorable office environment and applying appropriate adjustments or orthoses to improve functional capacities [11]. A tailored rehabilitation for BPI encompasses several critical aspects: preventing muscle atrophy, managing pain, restoring somatosensory deficits, minimizing developmental disregards, and providing post-operative care.
Case presentation
The examination was divided into sensory and motor assessments, including neurological and musculoskeletal assessments. A physical examination was conducted, and the therapist took written and verbal consent from the patient. The clinical presentation and subsequent surgical events are detailed comprehensively in Table 1 as the timeline of events. A comprehensive musculoskeletal and neurological assessment was performed. Pain assessment using the visual analog scale (VAS) rated his pain 5 out of 10 at rest and 8 out of 10 during activity. The pain was sudden in onset due to trauma, exacerbated by lower extremity movements, and alleviated by rest and medications. The pain was located at the lateral aspect of the thigh from the greater trochanter to the upper lateral aspect of the thigh and over the lateral aspect of the left dorsum of the foot and is described as dull aching. The patient also exhibits paraspinal muscle spasms. His range of motion was painful and incomplete.
On observation, the patient was conscious and oriented. The patient was observed in the highest independent attainable position (i.e., sitting position), and the left shoulder was slightly lower than the right shoulder and in a protracted position. The patient was inspected in a supine position with adequate exposure. Abrasions were present over the anterior surface of a tibial shin, as shown in Figure 1A, and abrasions were present over the left knee, as shown in Figure 1B. Sutures were seen at the following locations: over the dorsal aspect of the ankle (shown in Figure 1C), and a suture line is present from the greater trochanter (shown in Figure 1D) to the upper lateral aspect of the thigh.
Patient wound images1A shows abrasions over the anterior surface of a tibial shin, 1B shows abrasions over the left knee, 1C shows sutures present over the dorsal aspect of the ankle, and 1D shows the suture line present from the greater trochanter.
On palpation, tenderness grade I is present from the greater trochanter to the upper lateral aspect of the thigh, over the lower lateral aspect of the thigh, and the dorsal aspect of the ankle. Manual muscle testing (according to the Kendall muscle grading system) of the left (affected side) lower extremity: hip flexors, hip abductors, and ankle dorsiflexion were grade = 2+ (moves through a partial range of motion against gravity), whereas hip extensors, hip adductors, knee flexors, knee extensors, ankle plantar flexor, evertors, and invertors show grade = 2 (supported in the horizontal plane - movement in partial range), according to the Kendall muscle grading system. Manual muscle testing of the left (affected side) upper extremity was done - shoulder flexors and extensors only flicker were grade = 1, whereas shoulder abductors, shoulder adductors, shoulder internal and external rotators, elbow flexors, elbow extensors, wrist flexors, and extensors were grade = 0 (no contraction). Sensory examination revealed loss of superficial and deep sensations of the left upper extremity from C5 to T1 of the left affected extremity.
Upon examination, the range of motion of the bilateral affected and unaffected upper and lower extremities is shown in Table 2. All the normal ranges are also given as references.
Reflexes
Reflexes of bilateral upper and lower extremities are shown in Table 3.
Individual nerve testing of the brachial plexus
Individual nerve testing of the brachial plexus from the C5 root to the T1 root is done, and all the findings are listed in Table 4.
Investigations
Magnetic resonance imaging (MRI) of the brachial plexus in Figure 2 and X-ray of the left foot in AP view and the left side shaft of femur were shown in Figure 3.
MRI of the brachial plexusMagnetic resonance imaging (MRI) shows T2 hyperintense cystic lesions noted at the roots of the left C6, C7, and C8 nerve levels, continuing along the nerve roots and reaching up to the left scalene triangle, showing signs of pseudomeningocele. Edema was noted in the left scalene triangle and in the rest of the trunk, divisions, and cords.
X-ray of the left foot in the AP view and the left side shaft of the femurA: Left foot in the AP view showing the 1st, 3rd, and 4th metatarsal fracture, 2nd metatarsal comminuted fracture, and 1st proximal phalanx fracture. B: Left side in the AP view showing open reduction internal fixation with femur interlock nailing for the fracture of the femoral shaft on the left side.
Physiotherapy management
A tailored phase-wise rehabilitation protocol was designed as per the above case scenario. Early pain management and joint stabilization prevent complications and set the stage for more intensive rehabilitation. Sensory and motor re-education starts as soon as possible to maximize the potential for recovery. Lower limb exercises are essential to restore function, prevent complications associated with immobility, and prepare eventful weight-bearing activities. Phase I (0-4 weeks) is given in Table 5.
The rehabilitation of Phase II from four weeks to eight weeks is given in Table 6.
The rehabilitation program of Phase III (8-12 weeks) is given in Table 7.
Outcome measure
The outcome measures throughout the rehabilitation, which was measured as day one assessment, after one-month assessment, and after two-month assessment were given in Table 8.
Discussion
BPIs are one of the uncommon conditions that are often classified as obstetric or traumatic injuries. Motorcycle accidents frequently rank among the leading causes of traumatic BPIs, particularly in adult populations. This injury to the plexus causes issues with atrophy of associated muscle groups, neurologic degeneration, and lack of sensory and motor dysfunction [12]. BPIs are challenging and involve extensive, long-term comprehensive rehabilitation. Patients often have trouble with daily activities, including returning to work, particularly when the occupation requires manual labor [13]. The primary factor contributing to traumatic BPIs resulting from road traffic accidents is the occurrence of closed injuries. Additionally, Jain et al. noted that the dominant hand is often more frequently impacted [14]. The functional outcomes of the injury are influenced by various factors, including the severity, extent, and type of nerve damage. Consequently, different patterns of injury may result in a range of neurological disorders [2]. Rich et al. mentioned that road traffic accidents can result in traumatic BPIs, which are frequently a component of a complex polytrauma presentation, including fractures and dislocations of either the upper or lower extremity [13]. The study of Solomen et al. mentioned that the mechanism of injury was forced lateral neck flexion and head traction simultaneously, which was managed conservatively. The physiotherapy rehabilitation started late in this case and caused some sort of complications, which also delayed the prognosis of the patient [15]. Additionally, Rich et al. documented a case involving a 28-year-old patient who experienced polytrauma, resulting in multiple injuries to both the upper and lower extremities. They concluded that, due to the intricacy of the polytrauma, the rehabilitation would indicate sooner. The postponement of rehabilitation may potentially exacerbate post-traumatic nerve inflammation and impede the rate of nerve regeneration [13].
In the case report presented, the forces of traction, compression and direct impact applied to the patient's neck and shoulder during the injury may have played a role in the formation of both pre- and postganglionic BPIs. As the patient was managed conservatively, we set an early comprehensive rehabilitation approach firstly to minimize the possible secondary complications such as muscle atrophy and joint stiffness. Joint stiffness is reduced, and it also accelerates the rate of nerve regeneration, leading to a better prognosis for the patient's motor and sensory recovery. To develop a plan of care, problems were identified, goals were set, and intervention was planned as needed to minimize secondary complications and for a better prognosis regarding functional motor and sensory recovery. A comprehensive rehabilitation approach focused on pain management, strategies for sensory and motor re-education, the gradual restoration of lower extremity strength and endurance, and the development of neuromuscular control. As the patient is managed conservatively, immobilization is given through sling or hemi-sling/Velpeau’s bandaging. In a scoping review, de Santana Chagas et al. mentioned that scapular muscle strengthening should be considered to gain function in the upper limb as, due to injury, it can be biomechanically imbalanced and start causing complications. Scapular strengthening for improving stability and facilitating motor re-education and scapular synergy is presented. Additionally, electrotherapeutic modalities such as low-level laser therapy and electrical stimulation are found to be effective when given on individual motor points. Laser therapy helps in reducing pain due to its anti-inflammatory actions, which result in micro-stimulation. Graded motor imagery and biofeedback strategies were used to stimulate and improve neuromuscular control and to restore voluntary and active range of motion. Sensory re-education techniques using different textures, such as sandpaper, silk, and net, are employed to re-establish impaired afferent sensory pathways and restore sensory integration.
Conclusions
This case report underscores the critical need for a thorough and prompt rehabilitation strategy for patients suffering from TBPIs, especially those undergoing conservative treatment. By implementing customized rehabilitation techniques that emphasized pain alleviation, sensory and motor re-education, and the progressive enhancement of strength and neuromuscular coordination, notable advancements in both functional motor and sensory recovery were achieved. The application of diverse rehabilitation methods, such as electrotherapeutic modalities, graded motor imagery, and sensory re-education was vital in facilitating the patient's recovery. This rehabilitation program serves as a guideline for formulating early goal-oriented treatment strategies for patients with conservatively managed BPIs, highlighting the possibility of enhanced outcomes through a systematic and multidisciplinary methodology.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Treatment options for brachial plexus injuries ISRN Orthop Sakellariou VI Badilas NK Stavropoulos NA 314137201420142496712510.1155/2014/314137 PMC 4045367 · doi ↗ · pubmed ↗
- 2Review of rehabilitation protocols for brachial plexus injury Front Neurol Li H Chen J Wang J Zhang T Chen Z 10842231420233713907010.3389/fneur.2023.1084223 PMC 10150106 · doi ↗ · pubmed ↗
- 3Injuries of the terminal branches of the infraclavicular brachial plexus: patterns of injury, management and outcome J Bone Joint Surg Br Hems TE Mahmood F 7998049420122262859510.1302/0301-620X.94B 6.28286 · doi ↗ · pubmed ↗
- 4Adult brachial plexus injury: evaluation and management Orthop Clin North Am Limthongthang R Bachoura A Songcharoen P Osterman AL 5916034420132409507410.1016/j.ocl.2013.06.011 · doi ↗ · pubmed ↗
- 5Traumatic bilateral brachial plexus injury Cureus Kokkalis Z Papagiannis S Kouzelis A Diamantakis G Panagopoulos A 014202210.7759/cureus.24626 PMC 915092135664378 · doi ↗ · pubmed ↗
- 6Adult brachial plexus injuries: mechanism, patterns of injury, and physical diagnosis Hand Clin Moran SL Steinmann SP Shin AY 13242120051566806210.1016/j.hcl.2004.09.004 · doi ↗ · pubmed ↗
- 7Physical therapeutic treatment for traumatic brachial plexus injury in adults: a scoping review PM R de Santana Chagas AC Wanderley D de Oliveira Ferro JK Alves de Moraes A Morais de Souza FH da Silva Tenório A Araújo de Oliveira D 1201501420223354360310.1002/pmrj.12566 · doi ↗ · pubmed ↗
- 8Nerve reconstruction: a cohort study of 93 cases of global brachial plexus palsy Indian J Orthop Bhatia A Shyam AK Doshi P Shah V 1531604520112143087110.4103/0019-5413.77136 PMC 3051123 · doi ↗ · pubmed ↗