DNAH9 variants in children with post-infectious bronchiolitis/bronchitis obliterans
Yuhong Guan, Xiaoyan Zhang, Xiaolei Tang, Haiming Yang, Shunying Zhao

TL;DR
This study explores how DNAH9 gene variants may be linked to a rare lung disease in children following severe infections.
Contribution
The study identifies twelve DNAH9 variants in children with post-infectious bronchiolitis/bronchitis obliterans.
Findings
Six pediatric patients with DNAH9 variants were found to have PIBO after severe infections.
DNAH9 mutations included nonsense, splice site, and missense variants, all with low allele frequencies.
The variants were predicted to be harmful or of uncertain significance, suggesting a possible role in PIBO.
Abstract
Post-infectious bronchiolitis/bronchitis obliterans (PIBO) is a chronic irreversible obstructive lung disease that results in obstruction and/or obliteration of small airways. Previous reports have indicated that PCD-related gene mutations contribute to PIBO incidence. However, the relationship between DNAH9 variants and PIBO remains unclear. This study aimed to evaluate the association between DNAH9 mutations and the incidence of PIBO. In our cohort, 126 PIBO patients conducted Whole Exome Sequence (WES) test and twelve variants of DNAH9 gene were identified. Detailed clinical information, high-resolution computerized tomography and/or electronic bronchoscopy findings of the six pediatric children carried DNAH9 variants were systematically collected, meticulously reviewed, and rigorously analyzed. Clinical evaluation revealed three patients with bronchiolitis obliterans, two patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
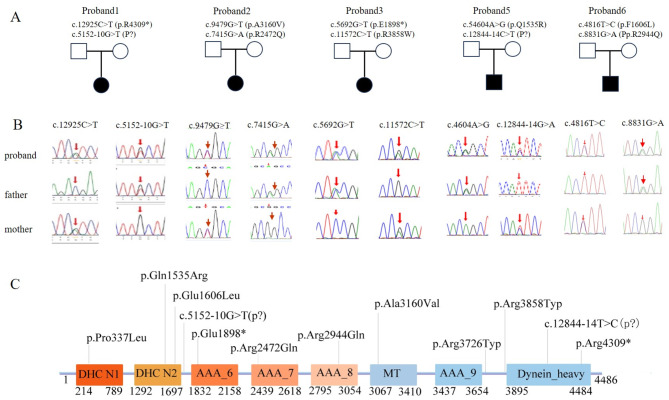 Figure 1
Figure 1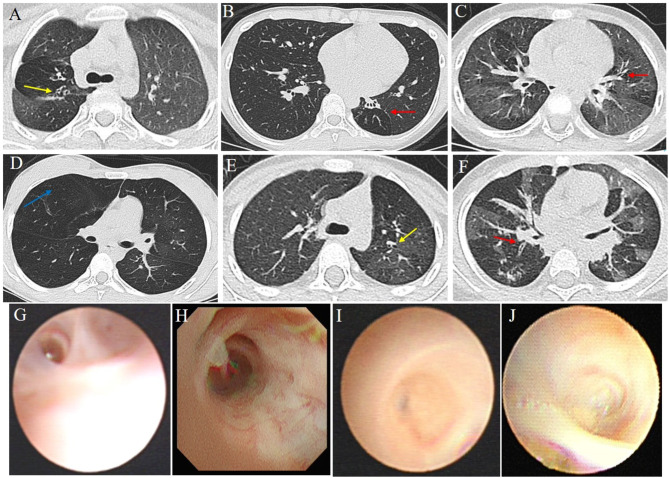 Figure 2
Figure 2- —http://dx.doi.org/10.13039/501100006739Capital Foundation of Medical Development
- —http://dx.doi.org/10.13039/100009110Natural Science Foundation of Xinjiang Uygur Autonomous Region
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Respiratory viral infections research
Introduction
Primary ciliary dyskinesia (PCD) is a rare genetic disorder characterized by considerable genetic and clinical diversity. Common clinical manifestations include chronic wet cough, recurrent wheezing, perennial nasal congestion, and laterality defects, with bronchiectasis affecting over 80% of PCD patients [1]. To date, more than 50 PCD-related genes have been identified [2]. Among these, DNAH9, which encodes a heavy chain of axonemal dynein, plays a pivotal role in ciliary motility by harnessing energy derived from ATPase-induced ATP hydrolysis to enable the generation of a sliding force by motile cilia. Notably, DNAH9 mutations have been associated with PCD in individuals presenting with situs abnormalities, mild respiratory manifestations, and severe asthenospermia [3–5]. Additionally, DNAH9 polymorphisms have been linked to asthma and bronchial hyperresponsiveness, particularly in response to early-life exposure to tobacco smoke [6].
Post-infectious bronchiolitis/bronchitis obliterans (PIBO) is a chronic obstructive pulmonary disease often arising after childhood bouts of severe lower respiratory tract infections, with PIBO susceptibility influenced by complex genetic and environmental factors that remain poorly understood [7]. Various hypotheses, including genetic predisposition (‘risk alleles’) and immune dysregulation, have been proposed as potential contributors to PIBO development [8, 9]. For example, Giubergia et al. reported an increased frequency of polymorphisms in the mannose-binding lectin 2 (MBL2) gene in PIBO patients as compared to healthy controls, underscoring the significant role of genetic factors in PIBO pathogenesis [10]. Similarly, variants of other PCD-related genes, such as CCDC39 and DNAH1, have been implicated in PIBO development [11, 12], with rapid advancements in sequencing techniques expected to lead to accelerated identification of novel disease-causing gene variants. This study explores the possible impact of DNAH9 variants on PIBO progression in children.
Materials and methods
Subjects
A hospital-based retrospective analysis was conducted on data for 126 children with PIBO and 118 were performed WES test at Beijing Children’s Hospital from during December 2017 to February 2023. Twelve variants of DNAH9 were identified in six patients. Clinical information, including detailed medical histories and findings of physical and accessory examinations, was collected by experienced pediatricians. The study protocol was reviewed and approved by the Ethics Committee of Beijing Children’s Hospital, China (Approval no. (2024)-Y-090-D). Informed consent was obtained from the parents of all study participants.
The diagnosis of post-infectious bronchiolitis obliterans was established based on the following diagnostic criteria: (1) history of an acute and severe lower respiratory tract infection; (2) repeated or persistent cough, wheezing, or shortness of breath over the 6 weeks after acute infection with decreased exercise tolerance; (3) mosaic perfusion signs, air trapping, bronchial wall thickening, bronchiectasis, or atelectasis on chest HRCT; (4) obstructive ventilatory dysfunction on pulmonary function tests; (5) exclusion of other chronic lung diseases occurring prior to BO onset, such as asthma and bronchopulmonary dysplasia [13, 14].
In this study, a history of Mycoplasma pneumoniae (MP) infection was confirmed if both of the following criteria were met: (1) serum anti-MP IgM titer ≥ 1:320 and/or ≥ 4-fold increase in anti-MP IgM titre between acute and recovery stages; (2) positive results of MP polymerase chain reaction (PCR) testing of pharyngeal swabs. Patients were diagnosed with adenovirus (ADV) pneumonia based on positive respiratory multiplex PCR test results obtained for adenovirus.
Genetic analysis
We performed WES on affected individuals followed by validation of segregation of candidate variants through analysis of parental variant profiles using Sanger sequencing (Fig. 1b and c). Variant filtering was performed based on a minor allele frequency (MAF) cutoff of < 0.01 in the gnomAD database as previously reported [11]. After genomic DNA samples were prepared, exonic DNA sequences were enriched using the NimbleGen 2.0 probe sequence capture array (Roche) then sequencing was performed using the Illumina HiSeq2500 platform (Illumina). Raw sequence data underwent quality assessment using the manufacturer’s recommended base-calling method then low-quality sequence reads (quality scores < 20) were discarded. The remaining sequence reads were aligned to the National Center for Biotechnology Information human reference genome (hg19) using Burrows-Wheeler alignment.
Fig. 1. Sanger confirmation and mapping of rare damaging mutations in the DNAH9 genes in five subjects. (A) Pedigrees of families 1–3,5,6 indicating the affected individuals and the segregation of DNAH9 recessive variants. (B) Sanger sequencing on DNAH9 variants in the patients and their unaffected parents of patient 1–3,5,6. (C) Predicted protein model of DNAH9 with the distinct domains and indication of DNA fragment distribution for protein-protein interaction experiments
Variant calling based on single-nucleotide polymorphisms and insertions and deletions was performed using SAMtools and Pindel, respectively. Candidate missense mutations were evaluated for pathogenicity using SIFT (http://sift.bii.a-star.edu.sg/), PolyPhen-2 (http://genetics.bwh.harvard.edu/pph2/), and Mutation Taster (http://www.mutationtaster.org/). Splice-site changes were assessed using MaxEntScan (http://hollywood.mit.edu/burgelab/maxent/Xmaxentscan_scoreseq.html) and dbscSNV (http://www.liulab.science/dbscsnv.html) software packages. Variant evaluation followed American College of Medical Genetics and Genomics (ACMG) guidelines. Candidate causal variants of DNAH9 (GenBank: NM_001372.3) were confirmed using Sanger sequencing before parental carrier screening was performed.
Results
Clinical features of PIBO patients with DNAH9 variants
In this study, we enrolled six children diagnosed with bronchiolitis/bronchitis obliterans, along with the parents of five of them, resulting in the inclusion of five unrelated family trios and one sporadic case without parental samples for segregation analysis (Table 1; Fig. 1). Detailed clinical information and genetic results of recruited PIBO patients and parents were systematically reviewed; all recruited parents were unaffected and healthy (Fig. 1).
Table 1. Clinical features of the individuals with DNAH9 variantsP1P2P3P4P5P6Male/FemaleFFFFMMAge at present(y)59.83.114.34.41History------MP+--/+-Pulmonary BronchiectasisNYYYYN Bronchiolitis/bronchitis obliteransYYYYYY AtelectasisYNNNYN PFTNormalObstructiveObstructiveMIXNAObstructive FEV1/R_5_ (%pred)84.777.1162.415.3-- FVC/R_20_ (%pred)85.582.373.550.9-- FEF_25 − 75_ (%pred)/R_5 − 20_67.249.91.315.0--nNO (nl/min)136.498.6108.8331.8/48.9AthmaNYNNNNNRDNNNNNNSINNNNNNSinusitisYNNNYNOtitis mediaNNNNNNHearing lossNNNNNNMP: Mycoplasma pneumoniae; PFT: pulmonary function test; nNO: nasal nitric oxide; NRD: Neonatal respiratory distress; SI: situs inversus; NA: not available
Phenotypic characteristics of patients are summarized in Table 1. Among the six patients, four were male and two were female, with PIBO ages of onset ranging from 11 months to 13 years. The observed average age of presentation was 6.1 years.
In our cohort, five patients presented with an acute course of cough and fever (patients P1, P2, P3, P5, P6), with three of them also experiencing wheezing. The remaining patient presented with cough, dyspnea, and decreased exercise tolerance (P4). Patient P1 had a history of wheezing and skin allergy. Notably, none of the six patients exhibited signs of situs inversus (SI) or heterotaxy syndrome, while sinusitis was observed in three patients. Results of allergen tests and immunological assays were within normal ranges for all six patients. Three of the six patients were confirmed to be infected with M. pneumoniae, two with adenovirus, and one with both M. pneumoniae and adenovirus.
Nasal nitric oxide (nNO) levels were within the normal range for four patients, whereas one patient exhibited a relatively lower level (48.9 nl/min) than the typical cut-off value for PCD used in prior studies (77 nL/min). The nNO level of the remaining patient was not determined. HRCT showed mosaic perfusion, air-trapping, bronchial wall thickening in the lungs, confirming the diagnosis of bronchiolitis obliterans in three patients (Fig. 2). Additionally, bronchoscopy findings revealed the presence of subsegmental bronchitis obliterans and bronchiectasis in four patients, while pulmonary function tests revealed obstructive ventilation dysfunction in four patients (Fig. 2).
Fig. 2. Thorax CT imaging and of the six study subjects (A-F). Upper and lower rows indicate patient (1–6) images, respectively. Red arrows indicate mosaic attenuation patterns and Bronchiectasis. Yellow arrow indicates a large bronchiectasis and bronchial wall thickening. Blue arrow indicate emphysema. Bronchoscopy revealed presence of subsegmental bronchitis obliterans in four patients (G-J)
Genetic analysis
WES analysis was conducted to identify potential PIBO-related variants, resulting in detection of twelve compounds heterozygous DNAH9 variants in six unrelated patients. These variants included the following: c.12,925 C > T (p.Arg4309*), c.5152-10G > T (-), c.4604 A > G (p.Gln1535Arg), c.12844-14T > C (-), c.4816T > C (p.Phe1606Leu), c.8831G > A (p.Arg2944Gln), c.9479 C > T (p.Ala3160Val), c.7415G > A (p.Arg2472Gln), c.5692G > T (p.Glu1898*), c.11,572 C > T (p.Arg3858Trp), c.11,176 C > T (p.Arg3726Trp), c.1010 C > T (p.Pro337Leu). Among these variants, two were nonsense mutations, two were near splice acceptor sites, and eight were missense variants. Eight variants were classified as likely pathogenic variants, while four were deemed of uncertain pathogenic significance based on ACMG guidelines (Table 2).
Table 2. The pathogenicity of DNAH9 variants in PIBO patientscDNA change (Protein change)dbSNPSourceGnomAD (East Asian)Poly-phen2scoreMutation-TasterscoreSIFT ScoreACMGRefP1c.12,925 C > T(p.R4309*)NAM0.00007---PCurrentc.5152-10G > T(P? )NAPNone---VUSCurrentP2c.9479 C > T(p.A3160V)rs770572516MNone1.000Pro-D0.999 D-3.765 DVUSCurrentc.7415G > A(p.R2472Q)rs188772907P0.000890.034B0.726D-2.079 NVUSCurrentP3c.5692G > T(p.E1898*)-PNone---PCurrentc.11,572 C > T(p.R3858W)rs779372233M0.000021.000Pro-D0.999 D-7.480DVUSCurrentP4c.11,176 C > T(p.R3726W)rs3760436-0.00631.000 Pro-D0.999 D-7.517 DVUS35,050,399c.1010 C > T(p.P337L)Rs3744574-0.00560.026 B0.999 D-5.815DVUSCurrentP5c.4604 A > G(p.Q1535R)rs147183329P0.00341.000Pro-D0.999 D-3.664 DVUSCurrentc.12844-14T > C(P? )NAM0.00072---VUSCurrentP6c.4816T > C(p.F1606L)rs765169895M0.000330.884Pro-D0.999 D-5.474 DVUSCurrentc.8831G > A(p.R2944Q)rs550801585P0.00100.909 Pro-D0.625 D-2.851 DVUSCurrentD: Deleterious; N: Neutral; B: Benign
Pathogenicity analysis of DNAH9 variants conducted using SIFT and Mutation Taster bioinformatics tools revealed that all eight DNAH9 missense variants were deleterious with regard to disease-causing potential, while PolyPhen-2 analysis of these variants predicted that six of them were probably deleterious. Notably, c.1010 C > T (p.Pro337Leu) and c.7415G > A (p.Arg2472Gln) missense variants affected evolutionarily highly conserved amino acids within the DNAH9 dynein heavy chain 1 (DHC1) and ATPase domains, respectively. Similarly, the c.8831G > A (p.Arg2944Gln) and c.9479 C > T (p.Ala3160Val) missense variants affected amino acids within the AAA + ATPase domain, while c.12,925 C > T (p.Arg4309*) and c.11,572 C > T (p.Arg3858Trp) variants altered amino acids within the C-terminal domain.
Parental carrier testing
Parental carrier testing demonstrated that each parent of five of the six patients carried one of the mutations in a trans configuration, indicating an inherited pattern. However, parental samples for patient P6 were unavailable for DNA analysis. Importantly, no mutations related to primary immunodeficiency disease or cystic fibrosis transmembrane conductance regulator (CFTR)-related disorders were identified in these subjects.
Discussion
In this study, we identified biallelic variants in the DNAH9 genes of six unrelated Chinese patients with PIBO with the objective of assessing their potential roles as genetic contributor to the incidence of PIBO in children. DNAH9 encodes an axonemal dynein heavy chain that is critical for ciliary motility. Previous research by Zheng et al. demonstrated that Dnah9 KD mice exhibited increased mucin secretion, compromised lung function, substantial inflammation and outer dynein arm (ODA) defects [15]. Typically, patients with DNAH9 mutations present with mild respiratory symptoms, sinusitis, and occasional ciliarelated complex congenital heart disease [3, 4, 16, 17]. However, some DNAH9 mutations have been associated with chronic wet cough, asthma, bronchial hyperresponsiveness, and even jejunal atresia in rare cases [6, 13, 17, 18]. These findings underscore the considerable phenotypic variability associated with DNAH9 mutations across individuals.
While sinusitis is a common feature among patients with DNAH9 mutations, it is noteworthy that four patients in the current study had normal nNO levels despite the presence of ciliary function-disrupting DNAH9 mutations. This result suggests that residual ciliary activity may be sufficient to maintain normal nNO levels, as consistent with the observation that none of the six patients had experienced recurrent respiratory infections. However, despite their mild respiratory symptoms, all six patients developed PIBO following bouts of severe ADV- and/or MP-infected pneumonia. Interestingly, the DNAH9 variants identified in these individuals were either absent or occurred at low MAFs (< 0.005) in the gnomAD database, underscoring their potential rarity and clinical significance.
Notably, the c.1010 C > T (p.Pro337Leu) variant identified in patient P6 encodes an amino acid residue found within domain 1 of DNAH9 dynein heavy chain 1 (DHC1) within a region known to interact with full-length CCDC114 and contribute to ciliary dysfunction. Furthermore, the variant c.11,176 C > T (p.Arg3726Trp) has been previously implicated in complex congenital heart disease [16], highlighting its potential pathogenicity. Unfortunately, due to our patients’ poor lung function and young ages, transmission electron microscopy for assessing ciliary structure was not available in this study.
PIBO is a chronic and irreversible obstructive airway disease caused by damage to small airways following a lower respiratory tract infection [19]. Disease pathogenesis has been linked to certain genetic risk factors, including PCD-related genes [20]. Interestingly, inflammatory cytokines such as IL-1α and IL-8 may participate in the development of PIBO and ADV/MP infection-induced pneumonia [21–23]. Moreover, an analysis of immune function-related cytokine profiles of Dnah9 knock-down (KD) mice demonstrated significantly decreased levels of several cytokines, including GM-CSF, IL-1α, and TNFα [15], suggesting a link between DNAH9 mutations and altered cytokine profiles that may support lung lesion development. Previous research revealed that higher levels of Matrix metalloproteinases (MMPs) and lower concentrations of TIMPs were associated with airway remodeling at least in half of the children and in two third of the adults with PCD [24]. Mycoplasma pneumoniae in adult community-acquired pneumonia increases matrix metalloproteinase-9 serum level and induces its gene expression in peripheral blood mononuclear cells [25, 26]. Although children with DNAH9 mutations typically exhibit milder respiratory symptoms, it is may because that DNAH9 is located at the distal end of the cilia, where the cilia still retain partial motile function. In the absence of infection, they can maintain adequate airway clearance function. However, during virus and/or Mycoplasma pneumoniae (MP) infections, excessive airway inflammation and epithelial damage are triggered. This may achieve by inducing the release of inflammatory factors, modulating goblet cell mucus secretion in the airways, and increasing the level of matrix metalloproteinases, thereby leading to airway remodeling and epithelial-mesenchymal transition regeneration which finally lead to BO.
In summary, findings from this and other studies emphasize the pivotal role of DNAH9 variants in PIBO pathogenesis. However, further recruitment of PIBO cases with DNAH9 variants is needed to broaden our comprehension of PCD phenotypes. Additionally, more investigations are warranted to elucidate PIBO pathogenic mechanisms, explore genotype–phenotype correlations, understand the interplay between PIBO and ciliary dysfunction, and unravel the pathophysiological mechanisms associated with DNAH9 dysfunction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.