New minimally invasive technique for repositioning of a subluxated retropupillary iris-claw IOL using needle-assisted fixation
Celso Costa, Nuno Gouveia, Pedro Fonseca, Miguel Raimundo, Joaquim Murta, João Figueira

TL;DR
A new minimally invasive method using three needles successfully repositions subluxated retropupillary iris-claw IOLs, offering faster recovery and fewer complications.
Contribution
A novel, needle-assisted reenclavation technique for subluxated retropupillary iris-claw IOLs without trocars or sutures.
Findings
The technique was successfully performed on four patients with subluxated IOLs.
All patients regained baseline visual acuity with no post-operative complications over six months.
The method reduces operative time and surgical manipulation, enhancing recovery and safety.
Abstract
This paper presents a modification of the needle-assisted retropupillary fixation technique for iris-claw intraocular lenses (IOLs). We introduce a novel, minimally invasive reenclavation technique for managing subluxated retropupillary iris-claw IOLs. The technique was successfully performed on four patients diagnosed with subluxated retropupillary iris-claw IOLs. This approach involved a novel, minimally invasive reenclavation technique that utilized three needles: one long, straight translimbal needle crossing the anterior chamber and two needles introduced through the pars plana to reposition and securely reenclavate the IOL. All patients experienced immediate and significant visual recovery, with their baseline visual acuities reestablished postoperatively. Importantly, no post-operative complications were observed during the six-month follow-up period, highlighting the safety…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
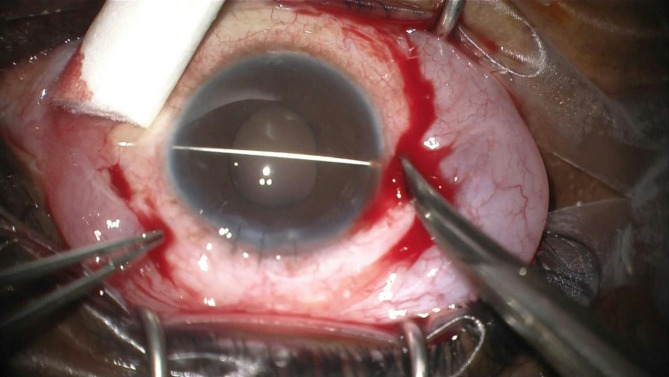 Figure 1
Figure 1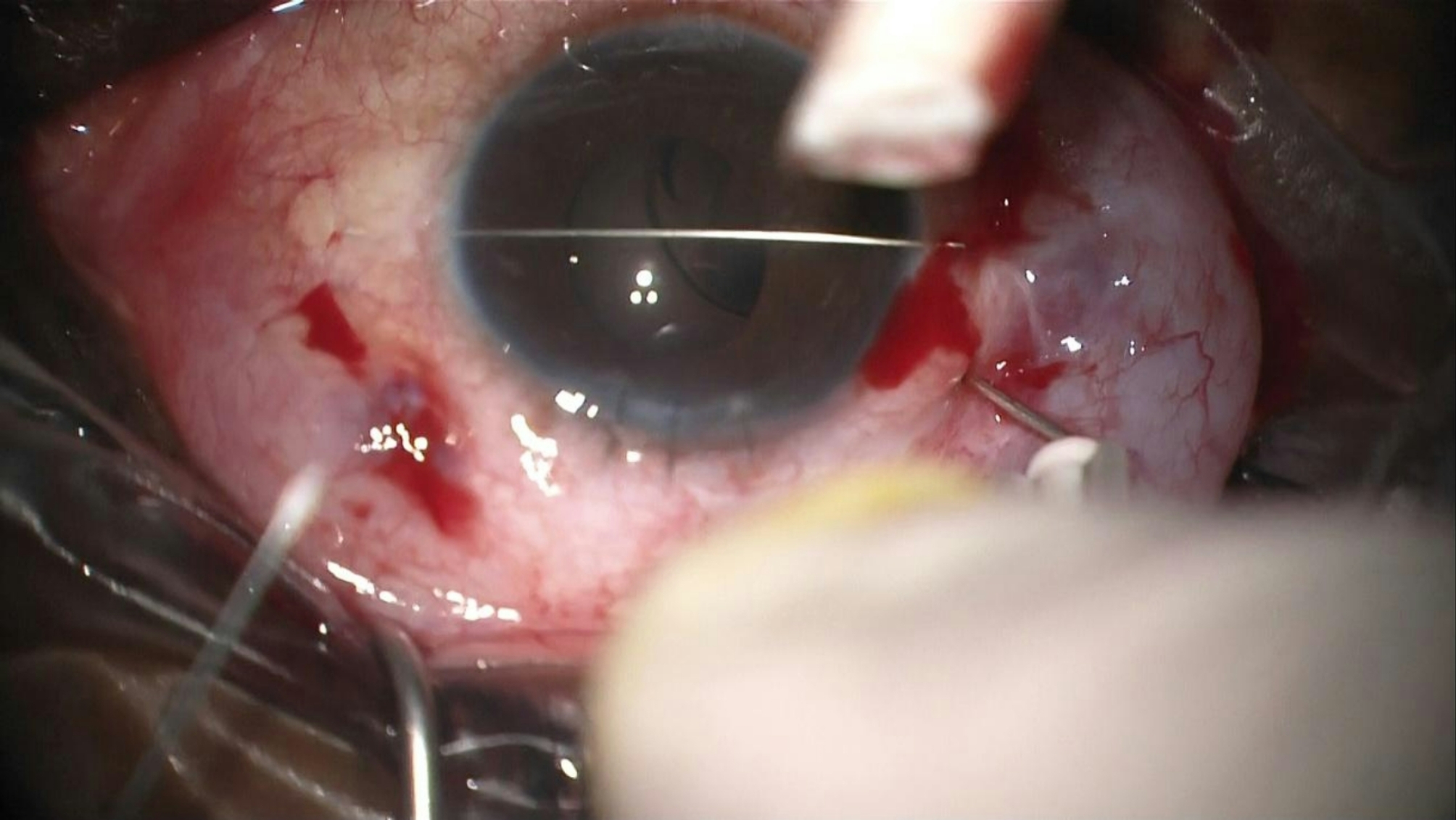 Figure 2
Figure 2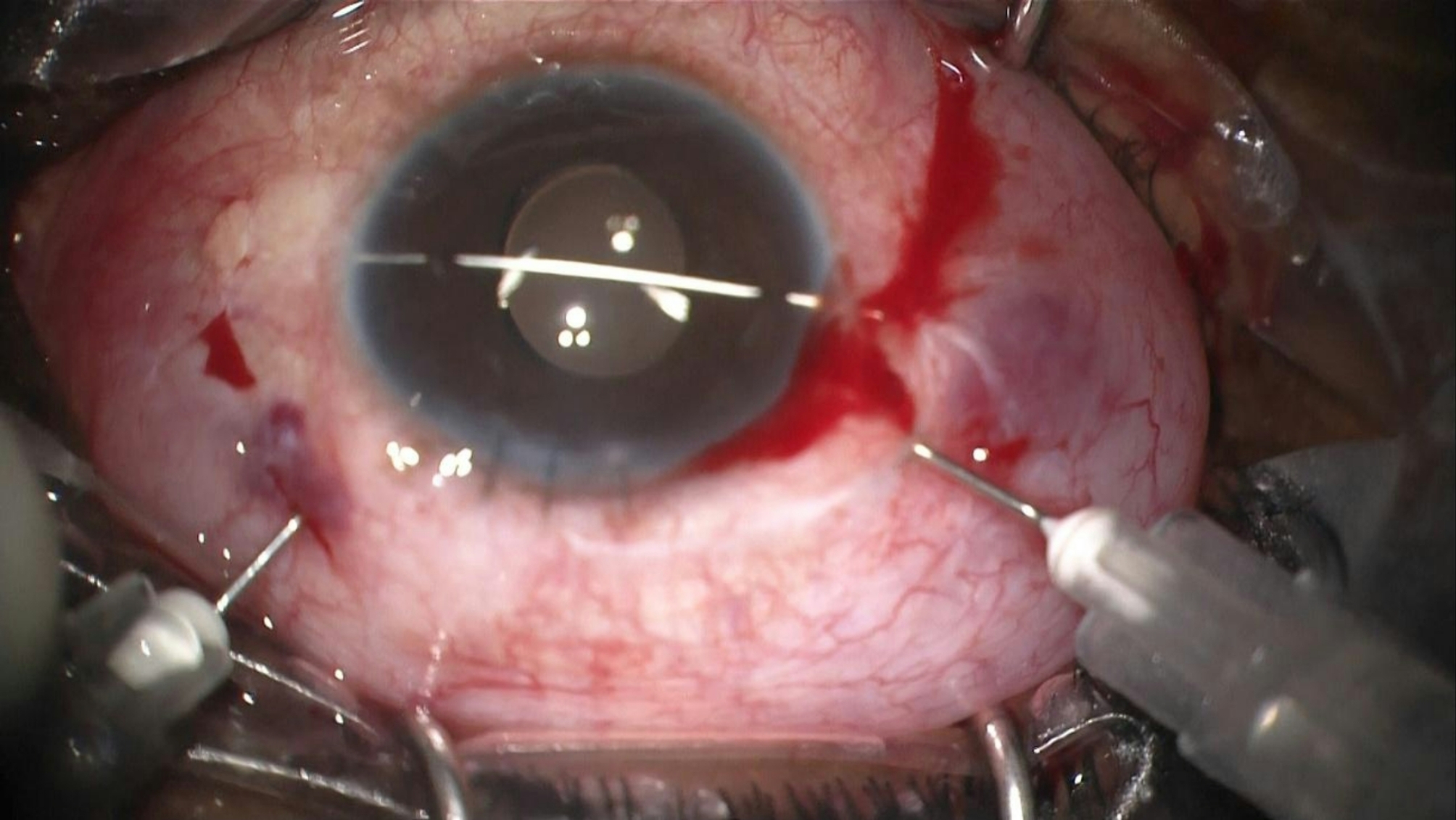 Figure 3
Figure 3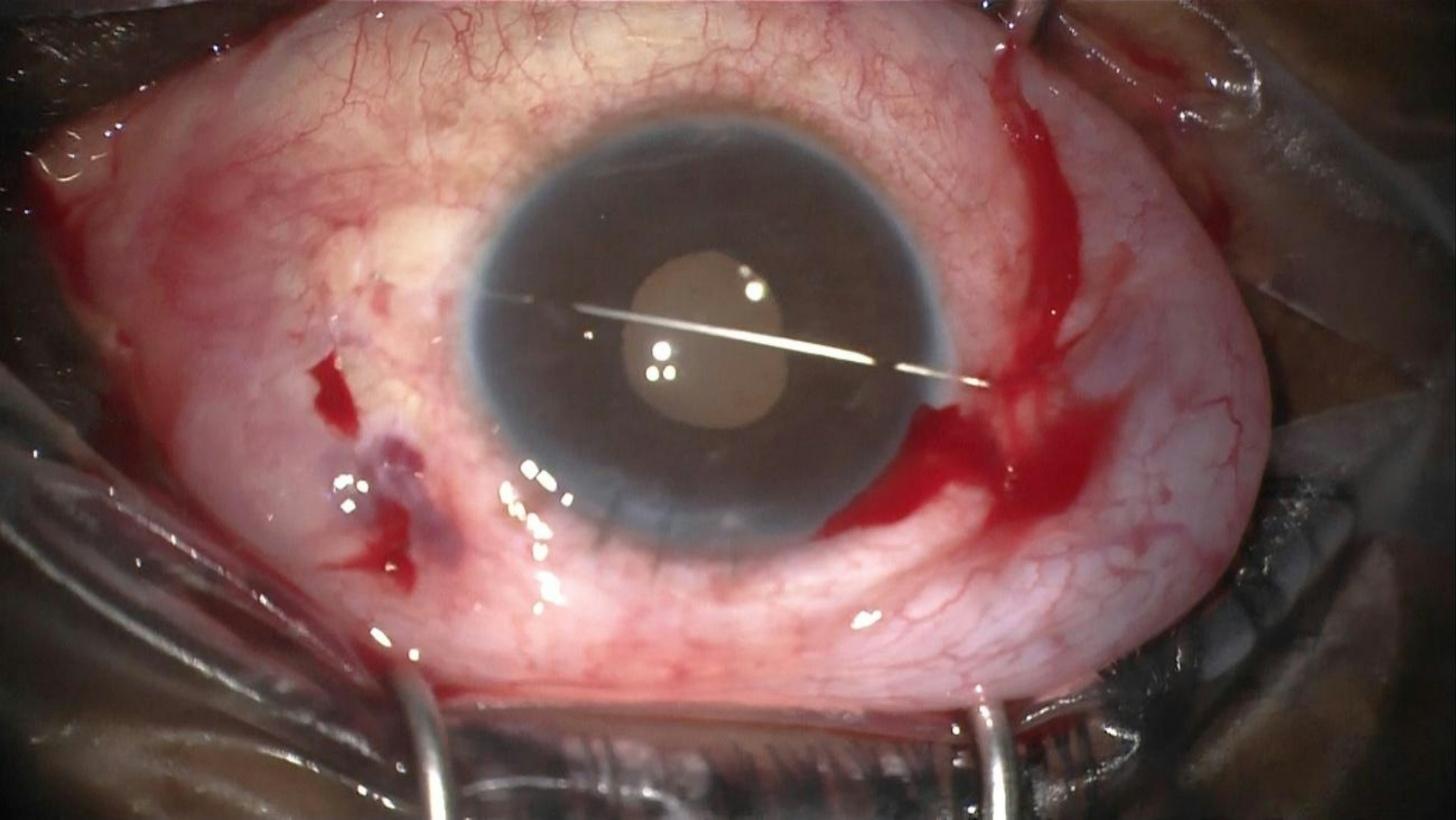 Figure 4
Figure 4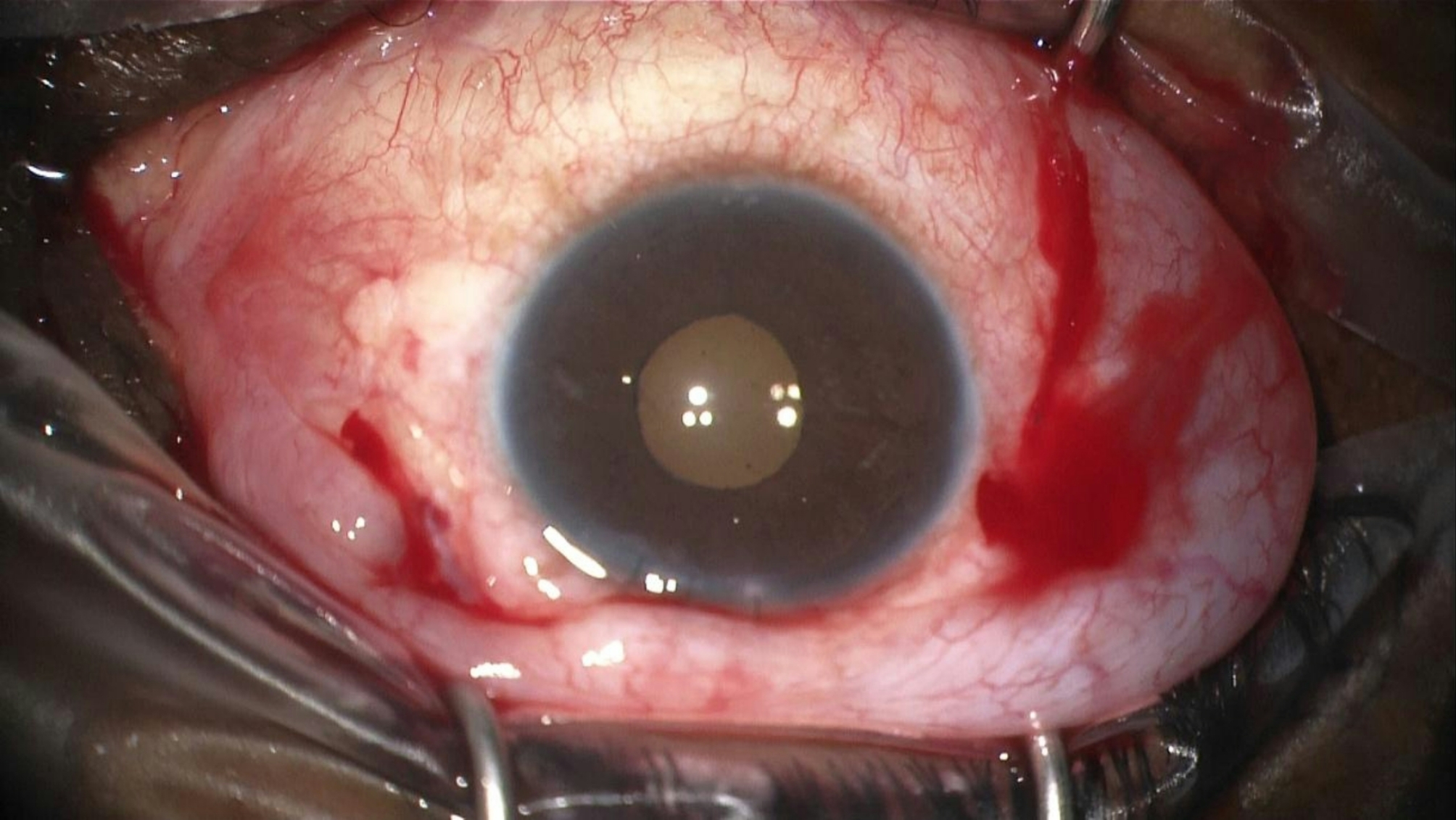 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntraocular Surgery and Lenses · Glaucoma and retinal disorders · Traumatic Ocular and Foreign Body Injuries
Background and purpose
The surgical management of aphakia without capsular support remains challenging. Two primary techniques are commonly employed: scleral fixation of a posterior chamber intraocular lens (SF-PCIOL), either with or without sutures, and iris-claw intraocular lenses (IC-IOL) [1, 2]. More recently, the fixation of IC-IOLs to the posterior iris surface has been introduced [3], offering several advantages. These include positioning behind the iris, away from the corneal endothelium, reduced complications, and improved visual outcomes [4, 5], though this comes with increased technical complexity. The technique can involve using an implantation forceps to hold the center of the IOL, coupled with an enclavation needle that enters through paracentesis at the 2 and 10 o’clock positions to perform the enclavation of the Artisan. Prieto et al. in 2017 [6] described the needle-assisted retropupillary fixation of iris-claw intraocular lenses as an alternative.
This technique begins with the passage of a long straight needle from a 10/0 Prolene suture through the corneal limbus, starting 1 mm behind it, from the 9 o’clock to the 3 o’clock position, crossing the anterior chamber. Using lens forceps, the iris-claw IOL is introduced through a 5.4 mm corneal incision and rotated into the horizontal plane, with its concavity facing the endothelium. The IOL is then positioned behind the iris and tilted towards the posterior iris surface. The anterior chamber needle serves as a pivot to enclave the haptics. Finally, the long straight needle is carefully removed.
There is limited information available in the literature regarding the management of subluxated retropupillary IC-IOLs, a complication that is not uncommon [7], with reported rates ranging from 0 to 37% [8]. Surgical approaches include combinations of full 3-port vitrectomy [9] or an anterior chamber maintainer with the creation of a scleral tunnel or a paracentesis [10]. These more invasive techniques have the disadvantages of increased operating time and cost. We describe a novel, minimally invasive reenclavation technique for managing subluxated retropupillary iris-claw intraocular lenses.
Surgical technique
The technique involves a minimally invasive reenclavation approach using three needles. First, a long straight 0.2 Ph.Eur. STC-6 16 mm reverse cutting needle from a 10/0 Prolene suture is introduced across the anterior chamber, as previously described (Fig. 1). Next, two 27-gauge needles, bent at a 45-degree angle, are introduced through the pars plana, preferably laterally and superiorly (Fig. 2). These needles are used to push each haptic anteriorly towards the posterior iris surface, employing coordinated movements of both hands.
Fig. 1. The long straight unarmed needle of a 10/0 prolene is introduced across the anterior chamber
Fig. 2. Two 27-gauge needles bent at a 45 degrees angle are introduced through the pars plana across the anterior vitreous cavity, moving the IOL to the correct plane
The first needle is passed below the IOL at the point where the haptic is enclavated to the iris. This needle elevates the IOL and holds it in position while the other needle enclavates the iris within the haptic on the opposite side. This maneuver ensures correct positioning and stabilization of the IOL, facilitating the enclavation of the haptic against the anterior chamber needle (Fig. 3). Finally, the straight needle is removed, leaving the IOL in situ and maintaining a round and regular pupil (Figs. 4 and 5).
Fig. 3. Enclavation of the IC-IOL using counter-action from the anterior chamber needle
Fig. 4. The long straight needle functioning as a pivot to enclave both haptics, before removal
Fig. 5. After removing the anterior chamber needle, the IOL remains stable and the pupil round
Patient characteristics and surgical outcomes
We conducted a retrospective, non-comparative consecutive case series study involving four patients (four eyes) treated at our institution between May 2022 and May 2023. These patients presented with spontaneous or traumatic single-haptic subluxated retropupillary iris-claw IOL (Ophtec Artisan Aphakia). Informed consent was obtained from all participants, and the study adhered to the principles outlined in the Declaration of Helsinki for biomedical research. Surgical procedures were performed by two experienced surgeons (MR and JF). Table 1 provides details of the clinical characteristics and outcomes of the patients.
The representative case (Figs. 1, 2, 3, 4 and 5) involves Patient 1, an 85-year-old male who presented to our department with a history of blunt trauma to the left eye two days prior. The patient had undergone cataract surgery in the left eye elsewhere 15 years ago, which resulted in posterior capsule rupture and subsequent extensive anterior vitrectomy and retropupillary artisan aphakia IOL implantation. On examination, his visual acuity was counting fingers without correction, improving to 20/25 with + 9.00D correction. Intraocular pressure was 21 mmHg, and slit-lamp examination revealed a single-haptic dislocation of the retropupillary iris-claw IOL. Fundoscopic examination was unremarkable. Following surgery, the patient experienced an immediate recovery, with visual acuity improving to 20/25 without correction and 20/20 with − 0.50 × 90º refraction. There were no postoperative complications, and the IOL was well-centered. At the 6-month follow-up, the IOL remained well-positioned. A video demonstrating the surgical technique is available as a digital supplement to this manuscript (see Video, Supplemental Digital Content 1).
In our series, only one patient experienced recurrence of the subluxation (Patient 2). He had a history of ocular trauma 10 years ago, followed by traumatic cataract surgery, IOL implantation in the capsular bag, and pars plana posterior vitrectomy due to inferior macula-sparing rhegmatogenous retinal detachment. Subsequently, the retina redetached, and the IOL dislocated. He underwent a new vitrectomy, and the IOL was exchanged for a three-piece IOL in the ciliary sulcus. This sulcus IOL also subluxated, necessitating explantation and retropupillary implantation of an iris-claw IOL. Six months later, one of the haptics of the IOL disengaged from the iris, requiring reenclavation as described in this manuscript (see Video, Supplemental Digital Content 2). Months later, another haptic disengaged from the iris, leading to the decision to fixate the subluxated IOL to the anterior iris surface (with its concavity facing the posterior segment). Upon examination, we discovered that the subluxated haptic had a defect, likely contributing to the repeated disenclavations. With this anterior approach we were able to enclave the haptics with much more iris tissue than with the retropupillary approach, so the IOL is stable, as we are able to prove through direct observation.
Patient 3 had a history of IOL-capsular bag complex subluxation years after cataract surgery. We decided to explant the complex and implant a retropupillary IC-IOL, which subsequently subluxated in the following months. We performed our technique and managed this case successfully.
Patient 4 had a history of ocular trauma with an intraocular metallic foreign body that required immediate surgical intervention. She remained aphakic and used a rigid contact lens for 18 years. More recently, she developed intolerance to the contact lens, prompting us to implant a retropupillary IC-IOL, which subluxated two months later during a dental procedure involving a vibrating drill. This case was successfully managed as described in this report.
Table 1. Clinical results of patients submitted to minimally invasive retropupillary iris-claw intraocular lens using needle-assisted fixationPatient 1Patient 2Patient 3Patient 4Sex/age (years)M/85M/44M/83F/73Pre-operativeUCVACFHMCFCFBCVA (aphakic)20/2520/4020/3220/40IOP21141315PseudoexfoliationNoNoYesNoSubluxation (spontaneous vs. traumatic)TraumaticSpontaneousSpontaneousTraumaticPost-operative (6 months)UCVA20/2520/5020/3220/40BCVA20/2020/4020/2520/25IOP15161215Subluxation recurrenceNoYesNoNoBCVA, best-corrected visual acuity; UVCA, uncorrected visual acuity; IOP, intraocular pressure; HM: hand motion; CF, counting fingers
Discussion and conclusions
The anterior and retropupillary fixation of an iris-claw IOL provides effective options for managing aphakia in the absence of capsular support. According to Mora et al. [5], fixating the IOL behind the iris yields visual outcomes and postoperative complications comparable to anterior IOL fixation. However, Al-Dwairi et al. [4] reported even better outcomes with retropupillary fixation, including reduced IOL decentration or tilt, less postoperative intraocular pressure elevation, lower incidence of macular edema, and improved visual acuity.
The needle-assisted technique simplifies the enclavation process compared to the classic microspatula method [11]. This technique reduces the number of attempts needed to capture the iris, minimizing pigment dispersion and iatrogenic iris damage while promoting a more natural, round pupil shape. Additionally, by ensuring that fixation points are directly opposite and equidistant from the pupil, this approach reduces iris tissue stretching, resulting in less pupil ovalization.
Single-haptic dislocation of a retropupillary IC-IOL may be more common than previously recognized, and the optimal management strategy remains a subject of debate. Our group first performed this technique in 2022, achieving favorable outcomes [12]. Another variation involves the use of two 30-gauge needles, one connected to a viscosurgical device [8]. In our experience, utilizing a single needle behind the IC-IOL complicates the process of correctly positioning, stabilizing, and refixating the lens.
Regarding disenclavation, we hypothesize that in some patients, the iris may become significantly fibrotic. Since it is impossible to directly evaluate the posterior surface of the iris, a fibrotic layer might be present. In such cases, recurrent episodes of disenclavation could occur. Therefore, it is recommended to redo the enclavation, securing the haptic with the use of a thread. Mora et al. [13] considered the presence of any sign of iris atrophy an exclusion criteria in their paper regarding light- and drug-induced pupillary dynamics in eyes with a retropupillary iris-claw intraocular lens, which supports our hypothesis.
Our technique can be performed under local or sub-Tenon anesthesia. This novel, minimally invasive reenclavation method, which requires only three needles, eliminates the need for trocar insertion, infusion cannula, scleral tunnels, corneal paracentesis, viscoelastic, or sutures. Although often unnecessary, the use of an infusion trocar or an anterior chamber maintainer could be considered by surgeons when operating on eyes that have undergone a posterior vitrectomy to maintain stable intraoperative eye pressure, as there may be an increased risk of intraoperative hypotony, especially if difficulties are encountered during the initial attempts at IOL enclavation. The short operative time, reduced surgical costs, and minimal surgical manipulations of our technique make it a relatively straightforward procedure. Additionally, patients experience rapid visual recovery, which is crucial given that these patients often undergo multiple surgeries and require simple yet effective interventions. Anterior vitrectomy is a prerequisite, considering the risk of vitreous traction in non-vitrectomized eyes.
The limitations of our study are inherent to a case series study, as the limited sample size may affect the generalizability of the results. Given the advantages and low complication rates associated with this technique, we advocate for its broader adoption, as well as conducting studies with a larger cohort of patients. This will be essential to identify any potential complications associated with the technique and robustly validate the outcomes.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prieto I. Técnica RP/IP (Técnica Retropupilar de Isabel Prieto). CIRP 2017– Reunião dos Grupos Portugueses de Cirurgia Implanto-refractiva, Superfície Ocular, Córnea e Contactologia; 2017; Albufeira, Portugal. Available: https://www.facoelche.com/enclavamiento-retropupilar-lente-artisan-tecnica-rpip/
- 2Almeida J, Costa TR, Vivas M, Monteiro C, Vaz FT, Silva DS et al. A new approach for single-haptic retropupillary iris-claw lens subluxation - The fencing technique. Eur J Ophthalmol. 2023; 11206721231222792.10.1177/1120672123122279238115710 · doi ↗ · pubmed ↗
- 3Khokhar S, Kumar S, Rani D, Majumdar A. Technique of re-enclavation of post-traumatic disenclaved haptic of posterior iris claw lens in a vitrectomised eye. BMJ Case Rep. 2021;14. 10.1136/bcr-2021-245570.10.1136/bcr-2021-245570 PMC 845833034548303 · doi ↗ · pubmed ↗
- 4Costa C. Needle-guided retropupillary fixation and repositioning of iris-claw intraocular lens. Euretina Congress. 2022; 2022; Hamburg, Germany. Available: https://euretina.org/resource/abstract_2022_needle-guided-retropupillary-fixation-and-repositioning-of-iris-claw-intraocular-lens/