Aseptic meningitis in the setting of giant cell arteritis (GCA): a case report
Lehashenee Thirukumar, Robin Sia, Justin Jackson, John Burston

TL;DR
A 76-year-old woman with giant cell arteritis showed aseptic meningitis symptoms, highlighting a rare but important clinical association.
Contribution
This case report adds to the understanding of GCA complications by linking it to CSF pleocytosis and aseptic meningitis.
Findings
CSF pleocytosis occurred alongside GCA without abnormal neuroimaging findings.
High-dose corticosteroids improved symptoms, supporting GCA as the underlying cause.
Ultrasound confirmed GCA with a non-compressible halo sign in the temporal artery.
Abstract
Giant cell arteritis (GCA) is a vasculitis primarily affecting medium- and large-sized arteries. The diagnosis may be challenging and lead to delays in treatment. Cerebrospinal fluid (CSF) pleocytosis is an uncommon association but may occur due to central nervous system (CNS) vasculitis or pachymeningitis. We describe a case fulfilling the criteria for diagnosing GCA, associated with CSF pleocytosis and normal neuroimaging. A 76-year-old woman presented to our regional hospital with three weeks of fever, confusion and fatigue. Two days later, she developed a right temporal headache with scalp tenderness. Preliminary investigations, including an FDG-PET scan, were unrevealing. Cerebrospinal fluid sampling demonstrated an isolated mononuclear pleocytosis. Brain magnetic resonance imaging (MRI) and an extensive panel of investigations failed to identify a cause, and a diagnosis of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
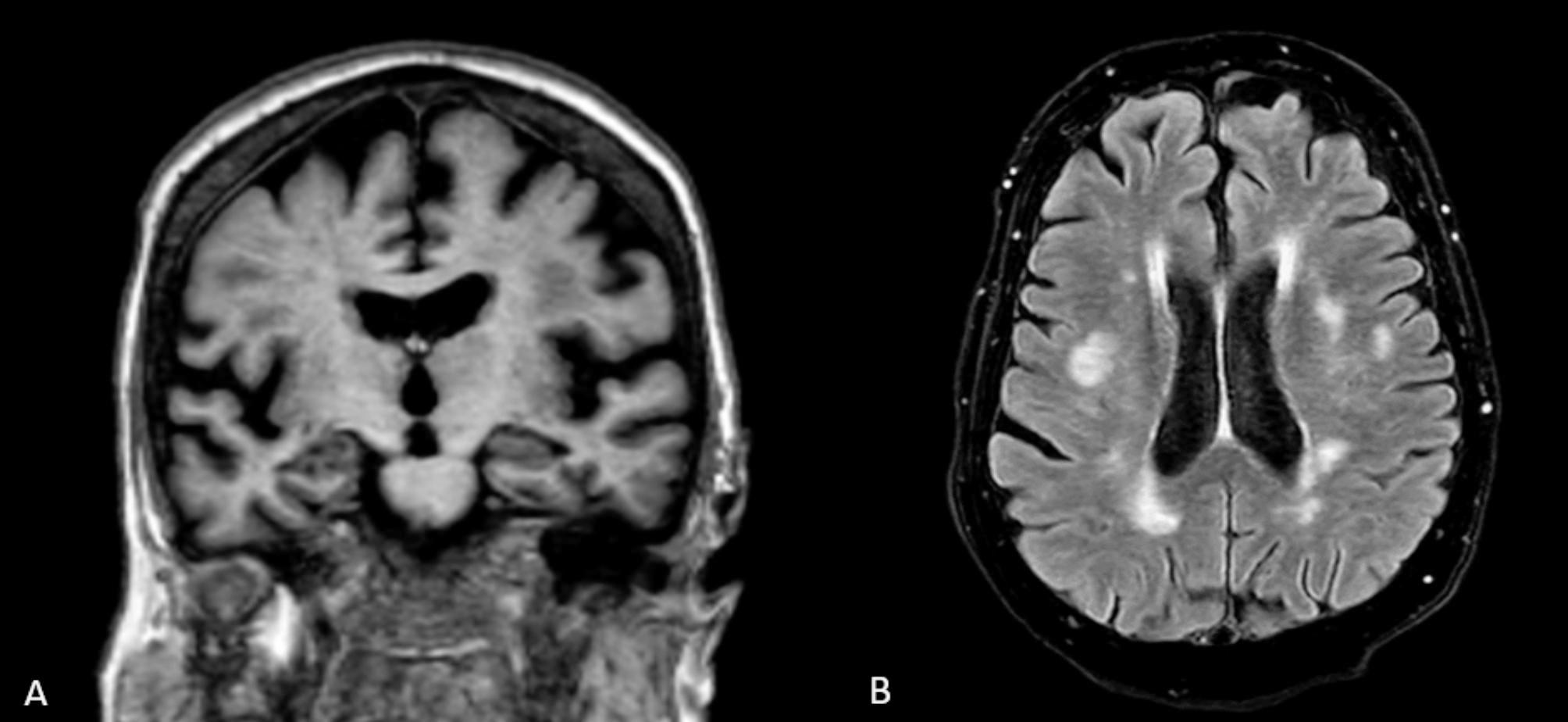 Figure 1
Figure 1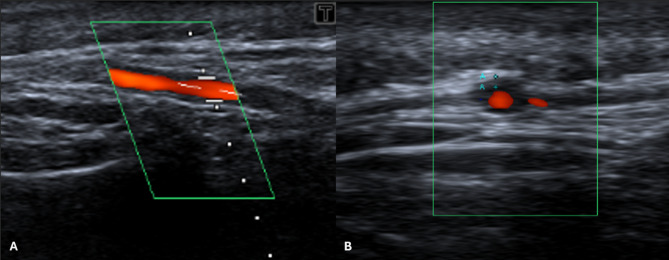 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Amyloidosis: Diagnosis, Treatment, Outcomes · IgG4-Related and Inflammatory Diseases
Background
Aseptic meningitis is characterised by meningeal inflammation with cerebrospinal fluid (CSF) analysis demonstrating pleocytosis but with negative Gram staining and cultures [1]. Viruses, including enteroviruses and herpesviruses, are the most prevalent infectious cause. Non-infectious causes include medications or may be linked to systemic inflammatory disorders such as systemic lupus erythematosus (SLE), sarcoidosis, and Behçet syndrome [2].
GCA, previously known as temporal arteritis, is a form of vasculitis affecting large and medium-sized vessels. Involvement of the temporal artery and other large vessels such as branches of the aorta and vertebral arteries are the hallmark of GCA, which often manifests clinically as headache, visual abnormalities, jaw claudication, and scalp tenderness [3]. Rare complications such as tongue necrosis and tongue claudication can also occur. Constitutional symptoms, such as fever, malaise, and fatigue are not uncommon [4]. Cerebrospinal fluid pleocytosis is an uncommon association with GCA but is recognised to occur in the context of central nervous system (CNS) vasculitis or pachymeningitis. These cases have been associated with focal neurology and/or neuroimaging changes.
Here, we describe a case of aseptic meningitis without focal neurology or MRI abnormalities occurring in association with GCA.
Case presentation
A 76-year-old Caucasian woman presented to our hospital with three weeks of quotidian low-grade fevers associated with mild chills, nausea, fatigue, loss of weight, anorexia, and confusion. Her past medical history included well-controlled type 2 diabetes, hypertension, previous cigarette smoking and a cervical spine fusion. She had no recent travel history or sick contacts. She lived at home alone and was independent in self-care.
On presentation, she was mildly confused but was not in distress. Examination of the lymphoreticular, neurological, cardiovascular, and respiratory system was unremarkable. Neck examination was limited by her previous spinal fusion. Two days after admission, she complained of a right temporal headache associated with overlying tenderness. There was no jaw claudication, visual disturbance, or proximal muscle weakness. Further examination demonstrated no carotid bruit, equal blood pressure in both arms and an absence of peripheral synovitis.
Full blood count and serum biochemistry were normal. Multiple sets of blood cultures were negative. Her C-reactive protein (CRP) was 148 mg/L and her erythrocyte sedimentation rate (ESR) was 58 mm/hr. An extensive panel of investigations was conducted as described in Table 1.
Computer tomography (CT) of the chest, abdomen, and pelvis as well as fluorodeoxyglucose-positron emission tomography (FDG-PET) did not identify an occult source of infection or malignancy. Mildly avid bilateral mediastinal and hilar lymph nodes were seen on the FDG-PET, raising the possibility of neurosarcoidosis. The patient proceeded to bronchoscopy with endobronchial biopsy which yielded only benign epithelium and collagenous tissue and no evidence of granulomatous inflammation.
CSF analysis revealed a normal protein and glucose with a lymphocytic pleocytosis of 48 × 10^6^ cells per litre. The Gram stain was negative, there was no growth on CSF cultures and a viral PCR panel was also negative. A diagnosis of aseptic meningitis was made. Magnetic resonance imaging (MRI) of the brain performed on day 2 (without contrast) and on day 65 (with and without contrast) excluded pachymeningitis, identifying only stable chronic small vessel ischemic changes (Fig. 1).
Table 1. Diagnostic investigations undertaken which were negative or within normal limitsAutoimmune markersParaneoplastic and neuronal antibodiesInfective ScreeningOther serum markersCSF analysisBroncho-alveolar lavageAnti-CCPRheumatoid factorAnti-dsDNAANAMPO-ANCAPR3-ANCAENA antibodiesHLA-B*51ANNA-1/anti-HuANNA-2/anti-RiAnti-PCA-1/YoAnti-PCA-2Anti-CV2/CRMP5Anti-PCA-TrAnti-Ma/TaAnti-GADAnti-AmphiphysinHIV serologySyphilis serologyRespiratory viral PCRCMV PCREBV PCRTB IGRAWhipple’s serologySerum ACELDHCreatinine kinaseSerum PEP and free light chainsTSHVitamin B12Enterovirus, HSV, VZV, EBV and CMV PCRCryptococcal antigenFungal cultureFlow cytometryBacterial cultureAFB staining and cultureAtypical pneumonia PCRCytologyHistopathologyFlow cytometryNote: Serum ammonia and immunoglobulin (Ig)G4 levels were not measuredAbbreviations: CCP, Cyclic citrinullated peptide; dsDNA, Double stranded DNA; ANA, Antinuclear antibody; MPO-ANCA, Myeloperoxidase-antineutrophil cytoplasm autoantibody; PR3-ANCA, Proteinase 3-antineutrophil cytoplasm autoantibody; ENA, Extractable nuclear antigen; PCA, Purkinje cell cytoplasmic antibody; CRMP5, Collapsin response mediator protein 5; GAD, Glutamic acid decarboxylase; IGRA, Interferon-gamma release assay; ACE, Angiotensin converting enzyme; LDH, Lactate dehydrogenase; PEP, Protein electrophoresis; TSH, Thyroid-stimulating hormone; HSV, Herpes simplex; VZV, Varicella-Zoster; EBV, Epstein–Barr virus; CMV, Cytomegalovirus; PCR, Polymerase chain reaction; AFB, Acid fast bacilli
Fig. 1. Non-contrast MRI of the brain on day 65 of admission. (A) Coronal view with age-related parenchymal changes without focal hippocampal atrophy. (B) Axial view showing mild chronic small vessel ischemic changes in the cerebral white matter
In view of the development and persistence of the right temporal headache, an ultrasound of the right temporal artery was performed. It demonstrated a non-compressible hypoechoic halo sign of 0.5 mm – exceeding the normal cut-off of 0.42 mm [5] – suggestive of GCA (Fig. 2).
Fig. 2. Duplex ultrasound of the right temporal artery. (A) Longitudinal view with visible thickening of the vessel wall. (B) Transverse view with halo sign indicative of GCA
The patient was commenced on intravenous methylprednisolone 1 g for three days and subsequently treated with oral prednisolone 60 mg daily with an ongoing weaning dose. She demonstrated significant improvement in her right temporal headache within days. Her fever, which had resolved within the first week of admission, remained absent. Inflammatory markers, including CRP and ESR, showed a downward trend and eventually normalised. A repeat lumbar puncture was not performed, and therefore, CSF was not retested post-treatment. However, despite these improvements, the patient’s confusion persisted. She developed persistent cognitive impairment, which required ongoing supportive management.
Discussion and conclusions
Aseptic meningitis, a syndrome with an acute or subacute onset, is defined as meningeal inflammation consisting of clinical features of meningitis, such as fever, headache, nausea or vomiting and neck stiffness, in conjunction with a CSF pleocytosis and negative Gram stain and cultures [1]. Our patient fulfilled the clinical and CSF criteria for aseptic meningitis.
The 2022 ACR/EULAR Classification Criteria state that a diagnosis of GCA can only be made in patients aged 50 and above [3]. According to these classification criteria, either a positive temporal artery biopsy or a halo sign elicited on temporal artery ultrasound generates the greatest diagnostic weight, scoring 5 points. Additional points are given for evidence of extracranial vessel involvement, such as visual loss, jaw claudication or scalp tenderness, as well as investigation findings including a raised ESR or CRP [3]. Our patient’s presentation scored 12 points, well above the 6 points required to support the diagnosis of GCA. In patients with a high pre-test probability and positive imaging findings, additional investigations such as temporal artery biopsy may not be required [6].
Given the challenging assessment of a confused patient, rare association of CSF pleocytosis with GCA and an FDG-PET scan which did not reveal evidence of vasculitis, there was a delay in confirming the diagnosis in our patient. While the 2023 EULAR recommendations state that FDG-PET can be used as an alternative for evaluating cranial arteries in patients with possible GCA, ultrasound of the temporal and axillary arteries remains the first-line imaging modality [6]. Ultrasound has been shown to be more sensitive at detecting GCA than FDG-PET. In low risk-of-bias (RoB) studies, ultrasound had a greater pooled sensitivity than FDG-PET at 88% compared to 76% [7]. This is supported by Nielsen et al., the only low RoB study that directly compared ultrasound with FDG-PET, and reported a sensitivity of 91% for ultrasound compared to 79% for FDG-PET when assessing both cranial and extracranial arteries [8].
Neurologic complications in GCA are uncommon, and typically manifest as neuropathies or, rarely, ischemic strokes [9–15]. CSF abnormalities have previously been reported in GCA, including hyperproteinorrachia, elevated CSF interleukin-6 levels and mononuclear pleocytosis [11–20]. In contrast to our patient, CSF pleocytosis is often identified in association with focal neurology and evidence of intracranial vasculitis and ischaemic changes visualised on MRI [11–15]. A case report from 1980, prior to the widespread availability of MRI, reports an abnormal radioisotope brain scan and CSF findings consistent with intracranial vasculitis in association with GCA [16]. Patients have also been described with GCA-associated hypertrophic pachymeningitis, where, in addition to CSF abnormalities, contrast-enhanced MRI revealed enhancing dural thickening [19, 20]. Kutty et al. postulate that vascular inflammation of the dural arteries may result in dural thickening and CSF pleocytosis [19, 20]. Roelcke et al. reported a case of meningoradiculitis resulting in bilateral cranial nerve VII palsies with a CSF pleocytosis in association with giant cell arteritis [18].
Our case provides evidence that temporal arteritis may also result in a CSF pleocytosis in the absence of focal neurology or neuroimaging changes. Aseptic meningitis may result in leptomeningeal contrast enhancement on MRI, but is often absent in cases with little to no dysfunction of the blood-CSF barrier, which was likely in our patient given her normal CSF protein levels [21].
Table 2 describes the reported cases of CSF pleocytosis in association with GCA and illustrates the spectrum of neurological and clinical manifestations.
Table 2. Cases of GCA with CSF pleocytosis and their associated neurological findingsAuthorsPatient ageGCA featuresFocal neurologyCSF findingsNeuroimagingHirsch et al [11]47Headache, fever, weight loss, fatigue, elevated ESRLeft hemiparesisHyperproteinorrachia and pleocytosisAngiography: marked stenoses in intracranial arteriesSalvarani et al [12]72 (case 2)Headache, jaw claudication, elevated ESRSpastic dysarthria, apraxia of speech, gait ataxiaHyperproteinorrachia and pleocytosisMRI: multiple widespread ischaemic infarctsLarivière et al [13]59 (case 2)Headache, fever, weight loss, jaw claudication, scalp dysesthesia, diplopia, amaurosis, elevated CRPLeft hemidysesthesia, and horizontal diplopiaPleocytosisMRI: multiple small acute ischemic lesions, left frontal lobe ischaemia72 (case 4)Headache, weight loss, jaw claudication, scalp hyperesthesia, left amaurosis, elevated CRPLeft upper limb paresis, gait ataxiaHyperproteinorrachia and pleocytosisMRI: bilateral cerebellar infarctsParra et al [14]56Headache, weight loss, tender temporal arteries, raised CRP and ESRLeft central facial palsy, spastic tetraparesis, impaired awarenessPleocytosisMRI: multiple watershed infarcts, intracranial dissectionsRoelcke et al [18]63Headache, neck stiffness, fever, jaw claudication, tender temporal artery, raised ESRBilateral 7th nerve palsyHyperproteinorrachia and pleocytosisMRI: right cerebellar tentorium meningeal enhancement; normal parenchymaKutty et al [20]53Headache, fever, right orbital pain, raised CRP and ESRAbsentHyperproteinorrachia and pleocytosisMRI: focal enhancement of duraPresent case76Headache, fever, weight loss, fatigue, scalp tenderness, elevated CRP and ESRAbsentPleocytosisMRI: no acute infarct
Although GCA-induced cognitive impairment may be reversed when treatment is initiated early, our patient’s lingering confusion and cognitive deficits may have been caused by irreversible neural injury that occurred during the diagnostic delay. In GCA, the intense inflammatory process – exacerbated by age-related vascular changes – can cause microvascular damage and neuronal injury resulting in neurological aging that may not recover even after systemic inflammation is controlled [22]. Some reports, such as by Lahaye et al., demonstrated significant cognitive recovery with early intervention [23]. However, delayed treatment or pre-existing cerebrovascular pathology may lead to permanent deficits [22–24]. Additionally, while strokes are well-known causes of cognitive decline in GCA [24], our patient’s MRIs did not reveal any new infarcts, suggesting that a more subtle, diffuse inflammatory insult may be responsible. This is similar to the neuropsychiatric sequelae observed in a small case series of aseptic meningitis, where some patients experienced persistent cognitive impairment despite the resolution of acute inflammation [25]. Thus, even though the clinical and biochemical features of GCA improved, the irreversible damage incurred during the acute phase may account for her enduring cognitive impairment. Furthermore, the age-related involutional changes observed on the initial MRI Brain may have represented heretofore subclinical cognitive decline which was exacerbated by the protracted delirium associated with her illness.
Despite our extensive investigations, we acknowledge the possibility of an explanation other than GCA for the CSF pleocytosis present in our patient. However, the temporal association, lack of an alternate diagnosis and other reports of CSF pleocytosis in association with GCA strengthen the probability that GCA was the causal pathology.
In conclusion, our case alerts clinicians to the importance of considering GCA as a potential cause of aseptic meningitis and strengthens the associations between GCA and a CSF pleocytosis. Ultrasound of the temporal and axillary arteries represents a non-invasive and relatively inexpensive investigation modality and was key to achieving a diagnosis in our patient. Timely recognition and prompt initiation of steroids is necessary in GCA to prevent clinical deterioration and complications.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
Supplementary Material 4
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Larivière D, Sacre K, Klein I, Hyafil F, Choudat L, Chauveheid M-P, et al. Extra- and intracranial cerebral vasculitis in giant cell arteritis: an observational study. Medicine. 2014;93(28).10.1097/MD.0000000000000265 PMC 460311325526454 · doi ↗ · pubmed ↗
- 2Parra J, Domingues J, Sargento-Freitas J, Santana I. Extensive intracranial involvement with multiple dissections in a case of giant cell arteritis. BMJ Case Rep. 2014;2014.10.1136/bcr-2014-204130 PMC 398755624728901 · doi ↗ · pubmed ↗
- 3Boisch G, Duda S, Hartmann C, Weßling H. Hypertrophic pachymeningoencephalitis associated with temporal giant cell arteritis. BMJ Case Rep. 2018;2018.10.1136/bcr-2018-225304 PMC 616965330262524 · doi ↗ · pubmed ↗
- 4Watanabe R, Hashimoto M. Aging-Related vascular inflammation: giant cell arteritis and neurological disorders. Front Aging Neurosci. 2022;14.10.3389/fnagi.2022.843305 PMC 903928035493934 · doi ↗ · pubmed ↗
- 5Solans-Laqué R, Bosch-Gil JA, Molina-Catenario CA, Ortega-Aznar A, Alvarez-Sabin J, Vilardell-Tarres M. Stroke and Multi-Infarct dementia as presenting symptoms of giant cell arteritis: report of 7 cases and review of the literature. Medicine. 2008;87(6).10.1097/MD.0b 013e 3181908 e 9619011505 · doi ↗ · pubmed ↗
- 6Gunst J, Andersen H, Hjerrild S, Marinovskij E, Deutch S, Schembri A, et al. Neuropsychiatric symptoms among adult patients with aseptic meningitis: A prospective case series. Acta Psychiatrica Scandinavica. 2015;133.10.1111/acps.1253926685715 · doi ↗ · pubmed ↗