Utilization of Cardiovascular Procedures, Consultation Services, and Cardioprotective Medications Among Type 2 Myocardial Infarction Patients
Harsh Goel, Meera V. Kapadia, Karan V. Goenka, Caroline M. Schaefer, Frances L. Revere, James L. Januzzi, Saumil S. Datar, Cian P. McCarthy, Adwait G. Mehta

TL;DR
Patients with type 2 myocardial infarction receive fewer cardiovascular tests and medications compared to those with type 1 myocardial infarction in the U.S.
Contribution
This study is the first to compare cardiovascular resource utilization between T2MI and T1MI patients using a large U.S. database.
Findings
T2MI patients were significantly less likely to receive P2Y12 inhibitors, beta blockers, statins, and SGLT2i/GLP-1 agonists.
T2MI patients were less likely to undergo echocardiograms and coronary angiograms compared to T1MI patients.
The study highlights disparities in secondary prevention for T2MI patients in the U.S.
Abstract
Coronary atherosclerosis and recurrent cardiovascular events are common among individuals with type 2 myocardial infarction (T2MI). However, cardiovascular resource utilization among T2MI patients is unclear. The aim of the study was to characterize cardiovascular resource utilization among T2MI patients across the United States. Using Optum’s de-identified Clinformatics Data Mart Database, cardiovascular procedures, physician services, and prescriptions within 6 months postdischarge were compared among patients with T2MI vs type 1 myocardial infarction (T1MI) between October 1, 2017, and June 30, 2020. Multivariable logistic regression examined the odds of resource utilization in T2MI vs T1MI and identified predictors of utilization for T2MI. We identified 140,344 patients with myocardial infarction; 121,738 patients (87%) had T1MI and 18,606 (13%) had T2MI. All participants had 183…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
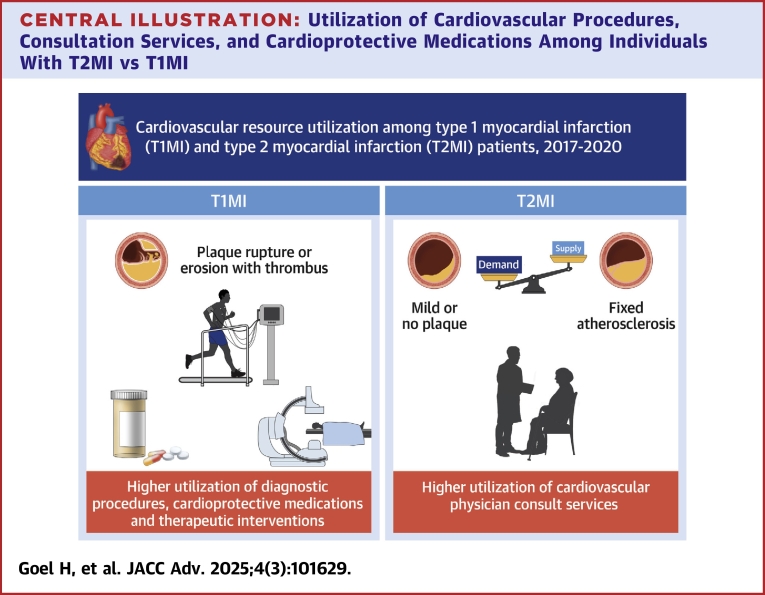 Figure 1
Figure 1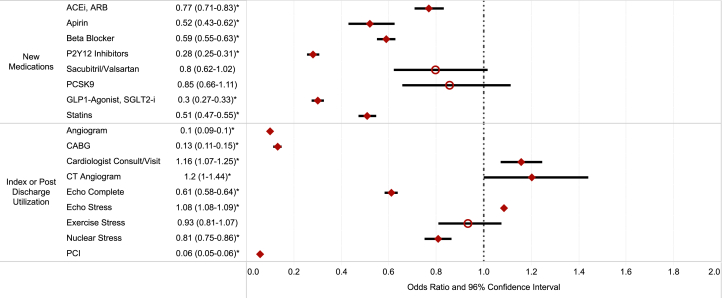 Figure 2
Figure 2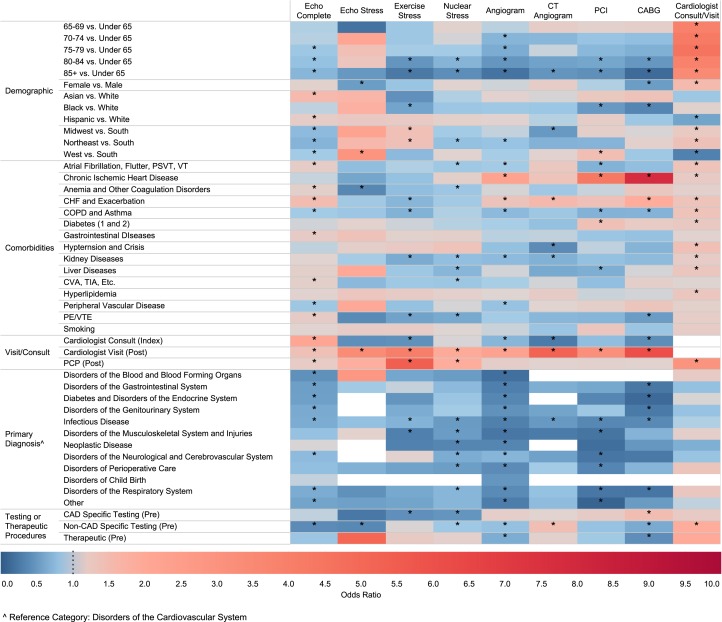 Figure 3
Figure 3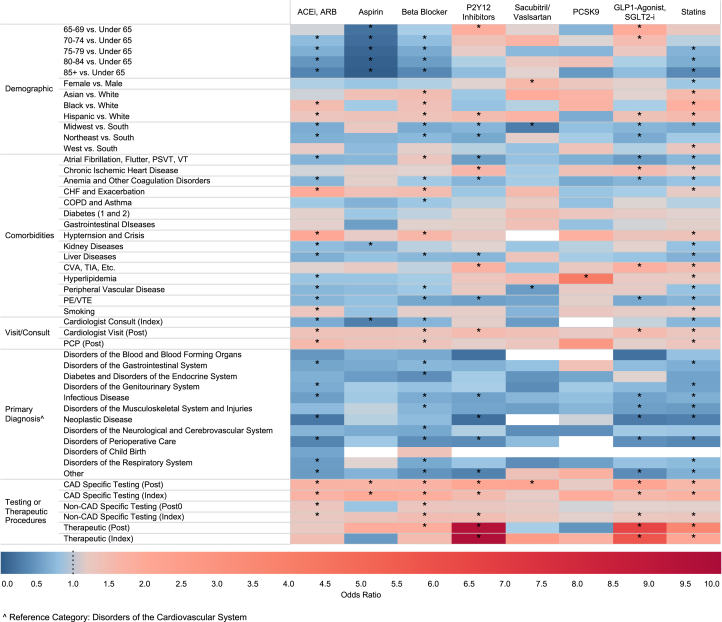 Figure 4
Figure 4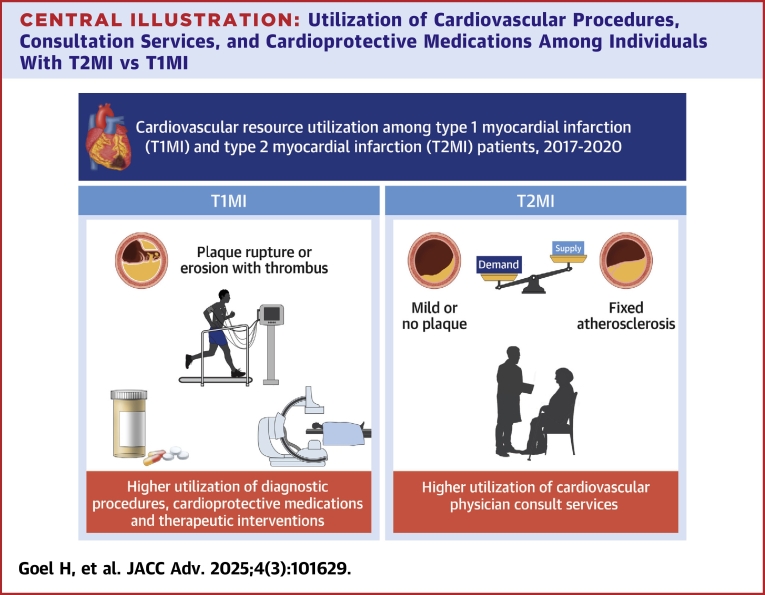 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Health and Mental Health · Acute Myocardial Infarction Research · Heart Failure Treatment and Management
Approximately 3-quarters of a million individuals experience a myocardial infarction (MI) in the United States every year. The pathophysiology of these MIs is diverse, with 5 distinct subtypes outlined in the Universal Definition of MI.1 For instance, type 1 MI (T1MI) is characterized by acute plaque rupture or erosion leading to acute thrombus formation. In contrast, type 2 MI (T2MI) is a heterogenous condition caused by a demand/supply mismatch from a variety of potential acute medical illnesses distinctly occurring in the absence of atherothrombosis.2 These 2 forms of MI are the most frequently encountered.
It is recognized that T2MI is prevalent, with several studies suggesting this form of MI may be as common, if not more so, than T1MI.3^,^4 In addition to being common, approximately 1-third of individuals who experience a T2MI have a recurrent major adverse cardiovascular event within 5 years of diagnosis.5 Recent prospective studies have revealed that the vast majority of individuals with T2MI have a high prevalence of coronary artery plaque including noncalcified plaque, which may be modifiable.3^,^6
Despite their high risk of recurrent cardiovascular events and high coronary plaque burden, single-center studies from large academic centers have suggested that individuals with T2MI often do not receive the same amount of diagnostic or therapeutic resources as T1MI.7, 8, 9, 10, 11 However, it is uncertain if these testing and treatment patterns are consistent across a broad range of health care facilities across the United States. Furthermore, studies to date have predominantly focused on inpatient hospitalization; data regarding resource utilization and medication fills postdischarge is lacking. This is important, as it is plausible that utilization of such resources may have been deferred to the outpatient setting after the patient recovers from their hospitalization.
Given these observations, we sought to characterize utilization patterns of cardiovascular resources in a nationally representative cohort of persons diagnosed with T2MI across the United States. The availability of an International Classification of Disease-10 (ICD-10) diagnosis code for T2MI since October 2017 facilitated such an analysis, which aimed to compare cardiovascular-specific diagnostic and therapeutic procedures, physician services, and cardioprotective medication prescription fill rates among patients with T2MI and T1MI and identify predictive factors for each among T2MI individuals.
Methods
This study was institutional review boards exempt by review of the University of Texas Health Science Center at Houston, as Optum’s de-identified Clinformatics Data Mart Database (CDM) database is publicly available and contains deidentified patient information.
Data source
This was a retrospective observational study using CDM. CDM is a large national database that includes approximately 67 million geographically diverse individuals from all 50 states in the United States. Data included in the database are deidentified and managed in accordance with Optum customer data use agreements. Individuals are included in the database by virtue of their commercial or Medicare Advantage insurance coverage. The database captures patient demographics, comorbidities, medical and prescription claims, resource utilization, and clinician information, with claims undergoing verification and adjudication.
Study population and patient characteristics
ICD-10-Clinical Modification (ICD-10-CM) diagnostic codes were utilized to identify individuals hospitalized with T1MI (121.0, 121.1, 121.2, 121.3, 12.4, 121.9) or T2MI (121.A1) in CDM from October 1, 2017, to June 30, 2020. ICD codes for T1MI, T2MI, and other clinical diagnoses were aggregated using the Clinical Classifications Software Refined. As a component of the Healthcare Cost and Utilization Project, the Clinical Classifications Software Refined groups over 700,000 ICD-10-CM codes into 530+ diagnostic categories (Supplemental Tables 1 to 3). Data included patient demographics, geographic region, comorbidities, index admission diagnosis, cardiovascular testing, procedures, and cardioprotective medication utilization before, during, and within 6 months of the index MI hospitalization. Analysis was limited to individuals with at least 6 months of continuous enrollment before and after hospitalization. Those under the age of 18 years, individuals with Medicare Supplements, or out-of-network claims were excluded.
Cardioprotective medications
Cumulative fill rates for cardioprotective medications within 6 months of discharge were determined using the standardized American Hospital Formulary Service classification system and the National Drug Code directory. Cardioprotective medications included antiplatelet medications like aspirin or purinergic receptor (P2Y_12_) inhibitors (clopidogrel, prasugrel, ticagrelor), beta-blockers, angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARBs), sacubitril/valsartan (Entresto), cholesterol-lowering medications (statins, ezetimibe, proprotein convertase subtilisin/kexin type 9 [PCSK-9] inhibitors), and diabetes medications such as sodium glucose co-transporter 2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) agonists. For each medication class, new prescriptions of each medication within 6 months of hospital discharge were compared to baseline prescription prior to their index MI hospitalization. Importantly, prior use of a specific medication did not preclude a patient from inclusion in analyses for other medication classes for which they had no preadmission prescriptions. This approach ensured that each medication class analysis was restricted to newly initiated treatments postdiagnosis. Nonstandard dosages and combination preparations of aspirin were excluded. Nonstandard formulations of beta-blockers (ie, eyedrops) were excluded.
Cardiovascular testing, procedures, and physician services
The ICD-10 Revision Procedure Coding System (ICD-10-PCS), Current Procedural Terminology codes, Healthcare Common Procedure Coding System (Supplemental Table 4), and CDM protocols were utilized to identify cardiovascular diagnostic and therapeutic procedures (collectively known as procedures) performed in-hospital and up to 6 months postdischarge, as well as cardiovascular specialty consultations during the initial admission and follow-up visits (diagnostic cardiovascular procedures included 2-dimensional echocardiogram complete, echocardiogram stress test, exercise stress test, nuclear stress test, diagnostic coronary angiogram, and computed tomography coronary angiogram). Therapeutic cardiovascular procedures encompassed coronary angiograms with therapeutic or interventional procedures (percutaneous coronary intervention [PCI]) and coronary artery bypass graft (CABG). Additionally, primary care physician (PCP) visits up to 6 months postdischarge were recorded.
Statistical analysis
Comparative analyses of patients with a primary or secondary diagnosis of isolated T1MI vs those with a primary or secondary diagnosis of isolated T2MI were conducted. Patients with a dual index diagnosis of T1MI and T2MI were excluded as the primary goal of our analyses was to understand how resource utilization differs for these 2 subtypes of MI. A sensitivity analysis was performed comparing the characteristics of individuals with T2MI and those with a dual index diagnosis of T1MI and T2MI, which revealed their characteristics to be similar (Supplemental Table 5). Comparative analyses examined demographics, geographic region, comorbidities, index admission diagnoses arranged in groups, cardioprotective medication use before (defined as prescription fills within 6 months prior to hospitalization) and during index admission or up to 6 months after hospitalization, as well as cardiovascular procedures before (defined as procedures performed within 6 months of hospitalization) and during index admission or up to 6 months after hospitalization. Comparison was done regarding the utilization of cardiovascular physician services during index admission and PCP/cardiovascular visits up to 6 months postdischarge. Continuous variables were analyzed using Student’s t-test and categorical variables with the chi-square or Fisher’s exact test.
Regression analysis utilizing multivariable logistic regression was used to determine unadjusted and adjusted ORs for new cardioprotective medication prescription, cardiovascular procedures, and cardiology or PCP service utilization in patients with isolated T2MI vs isolated T1MI. Utilization was defined as at least 1 new medication fill, procedure or physician encounter during the index admission or up to 6 months postdischarge from the hospital. Medication prescription ORs were calculated as the odds of new medication prescriptions in T2MI divided by the odds of new medication prescriptions in T1MI, with an OR <1 indicating lower odds of prescription fills. Similarly, OR for cardiovascular procedures and consultation were calculated as the odds of new procedures or consultations in T2MI divided by the odds of new procedures or consultations in T1MI, with an OR <1 indicating lower odds of procedures or consultation. For this analysis, patients were excluded who: 1) died during the index hospitalization; 2) discharged to hospice services; or 3) had a dual diagnosis of T2MI and T1MI.
For the regression analysis, 2 separate models with different covariates and outcomes were used. In the first model, assessing the OR of cardioprotective medication fills, control variables included demographics (gender, age, and race), geographic region, comorbidities, admission diagnostic group, index and postdischarge (within 6 months) cardiac procedures, index cardiology consults, and postdischarge cardiology and PCP follow-ups (within 6 months of discharge). In the second model, evaluating the OR of cardiovascular diagnostic tests, revascularization procedures, and cardiovascular physician evaluations, control variables included demographics (gender, age, race), geographic region, comorbidities, admission diagnostic group, preadmission cardiac diagnostic and therapeutic procedures, index cardiology consults, and postdischarge cardiology and PCP follow-ups (within 6 months of discharge). In both models, cardiac procedures were grouped into 3 categories: coronary artery disease (CAD) specific (echocardiogram stress test, exercise stress test, nuclear stress test, angiogram, and computed tomography coronary angiogram), non-CAD specific (echocardiogram), and therapeutic (PCI and CABG). The analyses were conducted using SAS 9.4.
Results
Patient characteristics
There were 140,344 individuals hospitalized with an isolated T1MI or T2MI over the 33-month study period: 121,738 (87%) had T1MI alone and 18,606 (13%) had T2MI alone (Table 1). All participants had 183 days postdischarge follow-up.Table 1. Baseline Characteristics of Patients With Myocardial InfarctionMI TypeP ValueT1MI (n = 121,738)T2MI (n = 18,606)Age, y**<0.001** Under 6527,993 (22.99)2,638 (14.18) 65-6917,422 (14.31)2,087 (11.22) 70-7420,471 (16.82)2,751 (14.79) 75-7919,185 (15.76)3,030 (16.29) 80-8415,478 (12.71)2,853 (15.33) 85+21,189 (17.41)5,247 (28.2) Mean ± SD72.25 ± 11.8275.94 ± 11.38Sex**<0.001** Female50,640 (41.6)9,346 (50.23) Male71,098 (58.4)9,260 (49.77)Race**<0.001** Asian3,122 (2.56)455 (2.45) Black16,082 (13.21)2,980 (16.02) Hispanic13,404 (11.01)1,710 (9.19) White89,130 (73.21)13,461 (72.35)U.S. region**<0.001** Midwest26,754 (21.98)4,015 (21.58) Northeast15,641 (12.85)3,779 (20.31) South56,991 (46.81)7,190 (38.64) West22,352 (18.36)3,622 (19.47)Charlson comorbidity index4 (2, 6)5 (3, 7)<0.001Comorbiditiesa Atrial fibrillation, flutter, PSVT, VT47,915 (39.36)10,370 (55.73)<0.001 Chronic ischemic heart disease106,164 (87.21)10,775 (57.91)<0.001 Hyperlipidemia104,462 (85.81)14,671 (78.85)<0.001 Smoking31,799 (26.12)4,042 (21.72)<0.001 Peripheral vascular disease22,321 (18.34)3,920 (21.07)<0.001 CVA, TIA, carotid stenosis, intracranial atherosclerotic disease36,010 (29.58)6,488 (34.87)<0.001 Pulmonary embolism/venous embolism or thrombosis9,940 (8.17)2,870 (15.43)<0.001 Diabetes (1 and 2)60,848 (49.98)9,549 (51.32)0.001 COPD and asthma42,498 (34.91)8,716 (46.85)<0.001 Anemia and other coagulation disorders42,802 (35.16)9,724 (52.26)<0.001 CHF and exacerbation62,228 (51.12)12,005 (64.52)<0.001 Liver diseases14,085 (11.57)3,340 (17.95)<0.001 Kidney diseases59,196 (48.63)13,028 (70.02)<0.001 Hypertension and crisis112,097 (92.08)17,484 (93.97<0.001 Gastrointestinal diseases12,038 (9.89)3,247 (17.45)<0.001Values are n (%), mean ± SD, or median (Q1,Q3).CVA = cerebrovascular accident; CHF = congestive heart failure; COPD = chronic obstructive pulmonary disease; MI = myocardial infarction; PSVT = paroxysmal supraventricular tachycardia; TIA = transient ischemic attack; T1MI = type 1 MI; T2MI = type 2 MI; VT = ventricular tachycardia.aPresent within 6 months of index admission.
Individuals with isolated T2MI were older (mean age 75.9 ± 11.4 years vs 72.3 ± 11. years), more commonly female (50.2% [9,346/18,606] vs 41.6% [50,640/121,738]), and more likely to be Black (16.0% [2,980/18,606] vs 13.2% [16,082/121,738]) than those with isolated T1MI.
Individuals with T2MI had a higher burden of comorbidities than those with T1MI as suggested by their Charlson comorbidity index (median weighted index of 5 [IQR: 3-7] vs 4 [IQR: 3-7]). Individuals with T2MI had a higher prevalence of prior arrhythmias (55.7% [10,370/18,606] vs 39.4% [47,915/121,738]), heart failure (64.5% [12,005/18,606] vs 51.1% [62,228/121,738]), kidney disease (70.0% [13,028/18,606] vs 48.6% [59,196/121,738]), prior cerebrovascular disease (34.9% [6,488/18,606] vs 29.6% [36,010/121,738]), than persons with T1M1. Conversely, certain atherosclerotic risk factors such as smoking (26.1% [31,799/121,738] vs 21.7% [4,042/18,606]), hyperlipidemia (85.8% [104,462/121,738] vs 78.9% [14,671/18,606]), and established chronic ischemic heart disease (87.2% [106,164/121,738] vs 57.9% [10,775/18,606]) were more common in individuals with T1MI than those with T2MI (Table 1). Individuals with T2MI were more likely to be admitted to a medical or surgical floor and less likely to be admitted to a cardiology floor than individuals with T1MI (Supplemental Table 6).
Cardioprotective medications prior to admission, while differing by statistical significance due to the large sample size, were numerically relatively similar among individuals with T2MI and T1MI including statins (45.1% [8,397/18,606] vs 43.8% [53,323/121,738], P < 0.001), ACEI/ARB (41.5% [7,727/18,606] vs 42.8% [52,048/121,738], P = 0.002), and beta blockers (44.6% [8,291, 18,606] vs 38.5% [46,860/121,738] P < 0.001), respectively (Supplemental Table 7).
Cardiovascular procedures prior to admission also differed by statistical significance but were numerically similar for most tests. However, a greater number of individuals with T2MI underwent an echocardiogram within 6 months of admission (41.1% [7,637/18,606] vs 28.4% [34,562/121,738]) (Supplemental Table 7).
Primary hospital diagnosis by MI subtype
Infectious diseases, diseases of the cardiovascular system, and respiratory system were the most common diagnostic groups among individuals with T2MI. In contrast, disorders of the cardiovascular system were the most common primary diagnostic group among individuals with T1MI (Table 2).Table 2. Primary Hospital Admission Diagnosis by MI SubtypeMI SubtypeP ValueT1MI (n = 121,738)T2MI (n = 18,606)Primary diagnosis**<0.001** Disorders of the blood and blood-forming organs and disorders involving the immune mechanism210 (0.17)177 (0.95) Disorders of the cardiovascular system97,879 (80.4)6,080 (32.68) Disorders of the gastrointestinal system1,901 (1.56)1,048 (5.63) Diabetes and disorders of the endocrine system, nutrition, and metabolism659 (0.54)278 (1.49) Disorders of the genitourinary system1,122 (0.92)730 (3.92) Infectious diseases11,083 (9.1)6,494 (34.9) Disorders of the musculoskeletal system and injuries1,735 (1.43)738 (3.97) Neoplastic diseases733 (0.6)392 (2.11) Disorders of the neurological and cerebrovascular system928 (0.76)452 (2.43) Disorders of perioperative care2,245 (1.84)503 (2.7) Disorders of the respiratory system2,176 (1.79)1,210 (6.5) Other1,047 (0.86)495 (2.66)Values are n (%).Abbreviations as in Table 1.
Diagnostic testing and cardiology evaluation according to MI subtype
Individuals with T2MI underwent fewer diagnostic tests during their index hospitalization and within 6 months postdischarge compared to T1MI (Table 3, Figure 1). This included diagnostic echocardiography (71.8% [10,179/14,176] vs 82.9% [82,551/99,593], adjusted OR: 0.61; 95% CI: 0.58-0.64) and invasive coronary angiogram (11.7% [1,664/14,176] vs 76.6% [76,327/99,593], adjusted OR: 0.1; 95% CI: 0.09-0.11).Table 3. New Diagnostic Test, Therapeutic Procedure, or Cardiology Consultation According to MI SubtypeProcedures During Index Admit or Within 6 Mo of DischargeT1MI (na = 99,593)T2MI (na = 14,176)Odds of Procedure/Intervention in T2MI vs T1MIUnadjustedAdjustedbEcho complete82,551 (82.89)10,179 (71.80)0.53 (0.51-0.55)0.61 (0.58-0.64)Echo stress477 (0.48)47 (0.33)0.69 (0.51-0.93)0.92 (0.67-1.25)Stress exercise3,245 (3.26)275 (1.94)0.59 (0.52-0.67)0.93 (0.81-1.07)Stress nuclear9,388 (9.43)1,253 (8.84)0.93 (0.88-0.99)0.81 (0.75-0.86)Angiogram76,327 (76.64)1,664 (11.74)0.04 (0.04-0.04)0.10 (0.09-0.10)CT angiogram1,132 (1.14)172 (1.21)1.07 (0.91-1.26)1.20 (1.00-1.44)PCI49,470 (49.67)258 (1.82)0.02 (0.02-0.02)0.06 (0.05-0.06)CABG18,292 (18.37)210 (1.48)0.07 (0.06-0.08)0.13 (0.11-0.15)Cardiology consult86,275 (86.63)12,913 (91.09)1.58 (1.49-1.68)1.16 (1.07-1.25)Values are n (%) or OR (95% CI). New diagnostic or therapeutic procedure or cardiology evaluation up to 6 months postdischarge from index MI admission.CABG = coronary artery bypass graft; CT = computed tomography; ECHO = echocardiogram; PCI = percutaneous coronary intervention; other abbreviations as in Table 1.aPatients who expired in hospital, were discharged to hospice, or did not have 6 months of continuous enrollment were excluded.bAdjusted for all demographics, comorbidities, primary diagnostic group, cardiac procedures, and physician evaluations.Figure 1. Multivariable Logistic Regression Comparing Odds of Cardiovascular Medications, Procedures, and Consultations for T2MI vs T1MIUtilizing multivariable logistic regression, unadjusted and adjusted OR were determined for new cardioprotective medication prescriptions, procedures, and cardiology or PCP services utilization in patients with isolated T2MI vs T1MI within 6 months of the index hospitalization. ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; CABG = coronary artery bypass graft; CT = computed tomography; ECHO = echocardiogram; GLP = glucagon-like peptide-1; MI = myocardial infarction; P2Y12 = purinergic receptor inhibitor; PCI = percutaneous coronary intervention; PCP = primary care physician; PCSK9 = paraprotein convertase subtilisin/kexin type 9; red circle = statistically insignificant; red diamond = statistically significant; SGLT2-i = sodium glucose co-transporter 2 inhibitor; T1MI = type 1 MI; T2MI = type 2 MI.
Conversely, patients with T2MI were more frequently evaluated by a cardiologist during hospitalization or as outpatients up to 6 months postdischarge (91.1% [12,913/14,176] vs 86.6% [86,275/99,593], adjusted OR: 1.16; 95% CI: 1.07-1.25) as compared to patients with T1MI. They were also slightly more likely to undergo a computed tomography coronary angiogram (1.2% [172/14,176] vs 1.1% [1,132/99,593], adjusted OR: 1.20; 95% CI: 1.07-1.25) (Table 3, Figure 1).
In a sensitivity analysis comparing T1MI to primary diagnosis T2MI (Supplemental Table 8), individuals with primary diagnosis T2MI were still less likely to undergo an echocardiogram (75.0% [481/641] vs 82.9% [82,551/99,593], adjusted OR: 0.55; 95% CI: 0.46-0.67) and an invasive angiogram (28.2% [181/641] vs 76.6% [76,327/99,593], adjusted OR: 0.12; 95% CI: 0.09-0.14) than those with T1MI. However, they were more likely to undergo a nuclear stress test (17.0% [109/461] vs 9.4% [9,388/99,593], adjusted OR: 1.56; 95% CI: 1.26-1.93).
Invasive treatment of MI according to MI subtype
A substantially lower number of individuals with T2MI underwent PCI (1.8% [258/14,176] vs 49.7% [49,470/99,593], adjusted OR: 0.06; 95% CI: 0.05-0.06) and CABG (1.5% [210/14,176] vs 18.4% [18,292/99,593], adjusted OR: 0.13; 95% CI: 0.11-0.15) during index admission and within 6 months postdischarge as compared to T1MI (Table 3, Figure 1).
The portion of individuals undergoing revascularization (PCI or CABG) following an initial angiogram (computed tomography coronary angiogram or invasive angiogram) was significantly higher in T1MI patients compared to T2MI patients (79.3% [60,596/76,385] vs 23.8% [414/1,740] P < 0.001) (Supplemental Table 9).
In a sensitivity analysis, comparing T1MI to primary diagnosis T2MI (Supplemental Table 8) individuals with T2MI, individuals with primary diagnosis T2MI were also less likely to undergo PCI (5.9% [38/641] vs 49.7% [49,470/99,593], adjusted OR: 0.08; 95% CI: 0.06-0.12) and CABG (5.0% [32/641] vs 18.4% [18,292/99,593], adjusted OR: 0.25; 95% CI: 0.17-0.37) than persons with T1MI.
Cardioprotective medication utilization according to MI subtype
Postdischarge, T2MI patients had significantly lower fill rates for secondary preventive therapies compared to T1MI patients across all major cardioprotective drug categories (Table 4, Figure 1), among those naïve to these medications at admission (ie, no prescription fill 6 months prior to MI hospitalization).Table 4. New Secondary Prevention Prescriptions According to MI SubtypeT1MI (na = 99,593)T2MI (na = 14,176)Odds of New Prescription in T2MI vs T1MIUnadjustedAdjustedbACEI or ARB naive55,667 (55.89)7,952 (56.09) New prescription19,036 (34.20)1,030 (12.95)0.29 (0.27-0.31)0.77 (0.71-0.83)Aspirin naive98,345 (98.75)14,040 (99.04) New prescription7,566 (7.69)158 (1.13)0.14 (0.12-0.16)0.52 (0.43-0.62)Beta-blocker naive60,817 (61.07)7,630 (53.82) New prescription38,219 (62.84)2,070 (27.13)0.22 (0.21-0.23)0.59 (0.55-0.63)P2Y_12_ inhibitor naïve84,998 (85.35)12,515 (88.28) New prescription44,833 (52.75)603 (4.82)0.05 (0.04-0.05)0.28 (0.25-0.31)Sacubitril/valsartan naive97,390 (97.79)13,939 (98.33) New prescription1,212 (1.24)90 (0.65)0.52 (0.42-0.64)0.80 (0.62-1.02)PCSK9i or ezetimibe naive97,534 (97.93)13,956 (98.45) New prescription2,269 (2.33)74 (0.53)0.22 (0.18-0.28)0.85 (0.66-1.11)GLP1-agonist or SGLT2-i naive85,341 (85.69)12,418 (87.60) New prescription30,202 (35.39)595 (4.79)0.09 (0.08-0.10)0.30 (0.27-0.33)Statin naive54,913 (55.14)7,554 (53.29) New prescription32,434 (59.06)1,439 (19.05)0.16 (0.15-0.17)0.51 (0.47-0.55)Values are n (%) or OR (95% CI). New prescriptions up to 6 months postdischarge from index MI admission.ACEI = angiotensin converting enzyme inhibitor; ARB = angiotensin receptor blocker; GLP1 = glucagon-like peptide-1; P2Y12i = purigenic receptor inhibitor; PCSK9i = paraprotein convertase subtilisin/kexin type 9 inhibitor; SGLT2-i = sodium glucose co-transporter 2 inhibitor.aPatients who expired in hospital, discharged to hospice or did not have 6 months of continuous enrollment were excluded.bAdjusted for all demographics, comorbidities, primary diagnostic group, cardiac procedures, and physician evaluations.
Among medication naïve individuals at the time of the index event, within 6 months of their hospitalization, individuals with T2MI were significant less likely to fill a new prescription for ACEI/ARBs (13.0% [1,030/7,952] vs 34.2% [19,06/55,667], adjusted OR: 0.77; 95% CI: 0.71-0.83), statins (19.1% [1,439/7,554] vs 59.1% [32,434/54,913], adjusted OR: 0.51; 95% CI: 0.47-0.55), P2Y_12_ inhibitors (4.8% [603/12,515] vs 52.8% [44,933/84,998], adjusted OR: 0.28; 95% CI: 0.25-0.31), beta blockers (27.1% [2,070/7,630] vs 62.8% [38,219/60,817], adjusted OR: 0.59; 95% CI: 0.55-0.63), nonstatin lipid-lowering medications such as PCSK9i or ezetimibe (0.5% [74/13,956] vs 2.3% [2,269/97,534], adjusted OR: 0.85; 95% CI: 0.66-1.11) or SGLT2i or GLP-1 agonists (4.8% [595/12,418] vs 35.4% [30,202/85,341], adjusted OR: 0.3; 95% CI: 0.27-0.33) as compared to individuals with T1MI, respectively (Table 4, Figure 1).
Predictors of new cardiovascular procedure and consultation following T2MI
Predictors of new cardiovascular procedures or consultations following T2MI are illustrated in (Figure 2, Supplemental Figures 1 to 9). Advancing age was strongly associated with utilization of cardiology consultations. In contrast, advancing age was associated with reduced utilization of diagnostic and therapeutic procedures. Females were more likely to receive postdischarge cardiology consultations but less likely to undergo stress echocardiogram and CABG. Racial disparities were also noted with Black individuals with T2MI having lower odds of undergoing exercise tolerance test, PCI, and CABG compared to White individuals. Compared to White individuals, Hispanic and Asian individuals were more likely to have an echocardiogram, while a Hispanic patient was less likely to have a cardiology consultation during admission or as an outpatient.Figure 2. Predictors of Cardiovascular Procedures and Consultations Among T2MI PatientsHeat map showing individual variables' effect on procedure or physician service utilization: blue (OR <1), red (OR >1), darker shades (OR further from 1). ∗Statistically significant. White boxes indicate covariates with null values. Cardiac procedures were grouped into 3 categories: CAD specific (echocardiogram stress test, exercise stress test, nuclear stress test, angiogram, and computed tomography coronary angiogram), non-CAD specific (echocardiogram), and therapeutic (PCI and CABG). CAD = coronary artery disease; CHF = congestive heart failure; COPD = chronic obstructive pulmonary disease; CVA = cerebrovascular accident; PE = pulmonary embolism; Pre = pre-hospitalization; PSVT = paroxysmal supraventricular tachycardia; TIA = transient ischemic attack; VT = ventricular tachycardia; VTE = venous thromboembolism; other abbreviations as in Figure 1.
Similar to medication fill rates, comorbidities had varying levels of influence on the likelihood of procedures and consultation (Figure 2, Supplemental Figures 1 to 9). Patients with heart failure were more likely to be evaluated with diagnostic echocardiography. In addition, patients with heart failure and chronic ischemic heart disease were more likely to undergo invasive coronary angiogram, PCI, and CABG. Conversely, patients with kidney disease and chronic obstructive lung disease or asthma were less likely to undergo procedures.
Admission and postdischarge follow-up significantly impacted procedure likelihood. An index cardiology consultation was associated with a high odd of echocardiogram but a lower likelihood of exercise stress test, invasive coronary angiogram, and CABG. Postdischarge cardiologist visit was associated with higher odds of all examined procedures. Similarly, a postdischarge primary care provider visit was linked to higher odds of echocardiogram, exercise stress test, nuclear stress, and cardiology consultation.
Primary diagnosis during admission also played a role. Patients admitted with diagnoses other than cardiovascular disorders had lower odds of undergoing procedures and consultation. To varying degrees, preadmission CAD-specific and non-CAD-specific therapeutic procedures were associated with a statistically significant reduction in utilization of procedures.
Predictors of new cardiovascular medication prescription following T2MI
Predictors of new cardiovascular prescription fill for each individual medication group are illustrated in Figure 3 and Supplemental Figures 10 to 17 for individuals with T2MI. Advancing age was a predictor for lack of new prescriptions of aspirin, statins, beta blockers, and ACEI/ARB prescription, but advanced age did not predict the odds of a new prescription of P2Y_12_ inhibitor, adjunct lipid-lowering therapy, or sacubitril/valsartan. Females were less likely to be prescribed statins. Black individuals with T2MI were more likely than White individuals to receive a new prescription for an ACEI/ARB, beta blocker, and statin following their index event. Compared to White individuals, Hispanic individuals with T2MI were more likely to receive a new prescription for an ACEI/ARB, beta-blocker, P2Y12i, GLP1 agonist, SGLT2i, and statins.Figure 3. Predictors of Cardiovascular Medication Utilization Among T2MI PatientsHeat map showing individual variables' effect on new cardioprotective medication prescription fill: blue (OR < 1), red (OR > 1), darker shades (OR further from 1). ∗Statistically significant. White boxes indicate covariates with null values. Cardiac procedures were grouped into three categories: CAD specific (echocardiogram stress test, exercise stress test, nuclear stress test, angiogram, and computed tomography coronary angiogram), non-CAD specific (echocardiogram), and therapeutic (PCI and CABG). ETT = exercise tolerance/stress test; Index = index hospitalization; P2Y12 = purigenic receptor inhibitor; PCI = percutaneous coronary intervention; PCSK9 = paraprotein convertase subtilisin/kexin type 9; PE = pulmonary embolism; Post = postdischarge; PSVT = paroxysmal supraventricular tachycardia; other abbreviations as in Figures 1 and 2.
Comorbidities had varying effects on the odds of prescription fill according to the class of medication (Figure 3, Supplemental Figures 10 to 17). For instance, individuals with heart failure were more likely to be prescribed an ACEI/ARB, beta blocker, and statin. A postdischarge PCP or cardiologist visit was associated with higher odds of a new ACEI/ARB, beta blocker, and statin medication fill within 6 months of the T2MI event. Having an admission diagnosis other than a disorder of the cardiovascular system was associated with a lower likelihood of being prescribed a new cardiovascular medication.
Diagnostic testing and therapeutic interventions, both during the index admission and postdischarge, were generally associated with new medication prescriptions, demonstrating varying positive ORs and levels of statistical significance.
Discussion
In this national study of individuals with T1MI and T2MI in the United States, significant differences in cardiovascular resource utilization were observed within 6 months of the index event (Central Illustration), aligning with findings from smaller, single-center studies but adding important information focused on the postdischarge period to 6 months following the event. Individuals with T2MI were significantly less likely to receive new prescriptions for cardioprotective therapies following their MI. Additionally, T2MI patients were less likely than T1MI patients to undergo cardiac testing and revascularization procedures during both the index hospitalization and within 6 months postdischarge. Finally, in an effort to understand these gaps, we describe predictors of new cardiovascular prescriptions, procedures, and consultations among individuals with T2MI.Central IllustrationUtilization of Cardiovascular Procedures, Consultation Services, and Cardioprotective Medications Among Individuals With T2MI vs T1MIFigure illustrating key differences in evaluation and treatment of these subtypes of MI. Abbreviations as in Figure 1.
Although noncardiovascular mortality is higher among individuals with T2MI than among those with T1MI, recurrent cardiovascular event rates are not inconsequential with 1-third of individuals experiencing a recurrent MI, stroke, or cardiovascular death over 5 years.5 Indeed, crude recurrent cardiovascular event rates for T2MI are comparable to T1MI.5^,^12^,^13 Accordingly, efforts to mitigate cardiovascular risk following a T2MI event are needed. Recent studies indicate a high burden of coronary artery disease and heart failure among individuals with T2MI suggesting a potential role for investigations and therapies to mitigate cardiovascular risk.6^,^14 For instance, the prospective DEMAND-MI (Determining the Mechanism of Myocardial Injury and Role of Coronary Disease in Type 2 Myocardial Infarction) study observed that 68% of consecutively enrolled T2MI patients had coronary artery disease with obstructive disease identified in 30% by invasive coronary angiography.6 Similarly, the DEFINE-TYPE 2 MI (DEFINing the prEvalence and characteristics of coronary artery disease among patients with TYPE 2 Myocardial Infarction using CT-FFR) study detected coronary plaque in 92% of individuals with T2MI by coronary computed tomographic angiography.3 The most recent American College of Cardiology/American Heart Association MI guidelines do not segregate treatment for non-ST segment elevation MI according to the subtype of MI (T1MI vs T2MI).15 However, small observational studies predominantly from single hospital systems have noted low utilization of secondary preventative therapies among individuals with T2MI at the time of hospital discharge.5^,^9^,^10^,^16^,^17
The ICD-10 code for T2MI created an opportunity to extend findings from single-center studies, which were typically small and usually only included results to the time of hospital discharge. This analysis of a large U.S. cohort shows that T2MI patients are significantly less likely to receive cardiovascular diagnostic and therapeutic resources than T1MI patients, both during hospitalization and up to 6 months postdischarge, a timepoint at which functional recovery from the hospitalization would have been expected to have occurred. Accordingly, opportunities to increase resource utilization for T2MI patients and implementation trials could clarify the benefits. To our knowledge, these data are among the first to evaluate postdischarge patterns of care in T2MI, an increasingly prevalent and highly morbid diagnosis.
Noteworthy findings in this study include the observation that cardiovascular consultation services were utilized more frequently in T2MI compared to T1MI, highlighting the diagnostic challenges in distinguishing between the 2.18 The discrepancy may be attributed to specific patient care and the corresponding role of cardiovascular physicians, either as “primary” providers or in more consultative roles. We observed that individuals with T2MI were more likely to be admitted to a medicine or surgical ward and less likely to a cardiology unit as compared to T1MI. An initial cardiology evaluation was associated with lower utilization of cardioprotective medications such as ACEI/ARBs, aspirin, beta-blockers, and statins, perhaps due to the lack of standardized guidelines. However, postdischarge diagnostic and therapeutic procedures were more common in patients who had a cardiology evaluation after discharge. Advancing age reduced the likelihood that an individual with a T2MI would be started on secondary preventative therapies. Given that individuals with T2MI tend to be older than those with T1MI and also have more medical comorbidities, understanding the cause and approach to manage this observation is important; further studies examining the net benefit of secondary preventative therapies for T2MI in this older population are needed. Furthermore, in this study, individuals with T2MI who underwent cardiovascular testing were more likely to be initiated on secondary preventative therapies. This raises the hypothesis that performing a coronary and structural heart disease evaluation in this population may result in escalation in secondary preventative treatment. Indeed, in the DEMAND MI study, coronary artery disease and structural heart disease were frequently newly discovered and often led to a change in medical therapy.6 Whether this testing and treatment initiation improves outcomes, however, remains uncertain. Clinical trials are being initiated to better understand the impact of noninvasive cardiovascular testing on T2MI patient outcomes (NCT05419583). Similar to prior studies,19^,^20 very low rates of inpatient invasive coronary angiography and revascularization occurred among individuals with T2MI in this study; extending previous work, this study also found very few patients undergo invasive angiography and revascularization after discharge and hospital recovery. Although it is important to note that approximately 24% (414/1,740) of patients with T2MI who underwent angiography subsequently received revascularization therapy, either through PCI or CABG. These data highlight the uncertainty regarding the role of revascularization for T2MI. An ongoing clinical trial is exploring the role of early invasive coronary angiography among individuals with T2MI.21
This study has several unique strengths. Firstly, this large, nationally representative dataset encompasses a diverse range of health care facilities, providing comprehensive insights. Secondly, several key predictors influencing medication fills in T2MI patients were identified by meticulously analyzing variables such as patient demographics, comorbidities, and primary diagnoses, offering a precise reflection of current clinical decision-making in T2MI management. Lastly, by using insurance claims data, actual patient-specific pharmaceutical filling patterns were captured, an important strength as nonadherence to cardiovascular medications is common.22
Despite its strengths, this study is subject to several limitations that merit consideration. First, ICD coding was used to identify MI events, and thus, misdiagnosis of T1MI or T2MI is a possibility. Limited studies to date have suggested higher agreement for T1MI ICD-10 codes than T2MI codes and adjudicated events using the 4th Universal definition of MI.23 Although claims data demonstrates modest agreement with adjudicated cases of MI,24 less is known regarding the accuracy of MI ICD-10 coding specifically in CDM. Second, prescriptions were identified via pharmacy claims; however, it is possible that patients may obtain medications over-the-counter. For instance, the rates of aspirin prescriptions were substantially lower than anticipated despite exploring various dataset permutations using American Hospital Formulary Service and National Drug Codes; this may be due to over-the-counter use of the drug. Indeed, a prior survey of patients in the United States revealed that 84% of patients receive aspirin over-the-counter rather than through their insurance.24 Third, while measuring prescription fills are a well-accepted metric of medication use and adherence,25 they have limitations. Patients may not take their medications exactly as prescribed, and the lack of medical record access precluded ability to assess health care providers' intentions regarding prescriptions, which are typically indicated in discharge summaries or discharge orders. Thus, discharging providers may have intended to treat patients with prescribed medications that were not filled by patients for various reasons. Lastly, as the database primarily includes commercially insured individuals with regional variations, the results may not necessarily generalize to individuals of lower socioeconomic status or certain geographical regions.
Conclusions
Despite a high expected prevalence of coronary artery disease and elevated rates of recurrent cardiovascular events, patients with T2MI were significantly less likely to be prescribed cardioprotective medications, undergo cardiovascular testing, and undergo revascularization when compared to those with T1MI. This discrepancy underscores the urgent need for clinical trials to identify optimal management strategies for T2MI, including whether enhanced cardiovascular resource utilization can improve outcomes for affected individuals.
Funding support and author disclosures
Dr Revere provided institutional support for data access and expertise. Dr Januzzi is supported in part by the Adolph Hutter Professorship at Harvard Medical School. Dr McCarthy is supported by a 10.13039/100000050National Heart, Lung, and Blood Institute Career Development Award (K23HL167659). Dr Januzzi reports a board position with Imbria Pharma, grant support from Abbott, Applied Therapeutics, AstraZeneca, BMS, Novartis Pharmaceuticals, consulting income from Abbott Diagnostics, Beckman-Coulter, Jana Care, Janssen, Novartis, Prevencio, Quidel, and Roche Diagnostics and serves on clinical endpoint committees/data safety monitoring boards for Abbott, AbbVie, Amgen, CVRx, Medtronic, Pfizer, and Roche Diagnostics. Dr McCarthy has received consulting fees/honorarium from Abbott Laboratories, Roche Diagnostics, HeartFlow, Inc, and New Amsterdam Pharma. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.PerspectivesCOMPETENCY IN PRACTICE BASED LEARNING: Despite a high expected prevalence of coronary artery disease and elevated rates of recurrent cardiovascular events, patients with T2MI were significantly less likely to be prescribed cardioprotective medications or undergo cardiovascular testing and revascularization when compared to those with T1MI.TRANSLATIONAL OUTLOOK: This discrepancy underscores the urgent need for clinical trials to identify optimal management strategies for T2MI, including whether enhanced cardiovascular resource utilization can improve outcomes for affected individuals.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Martin S.S.Aday A.W.Almarzooq Z.I.2024 heart disease and stroke statistics: a report of US and global data from the American Heart Association Circulation 14982024 e 347e 91310.1161/CIR.000000000000120938264914 PMC 12146881 · doi ↗ · pubmed ↗
- 2Thygesen K.Alpert J.S.Jaffe A.S.Fourth universal definition of myocardial infarction (2018)Circulation 138202018 e 618e 65110.1161/CIR.000000000000061730571511 · doi ↗ · pubmed ↗
- 3Mc Carthy C.P.Murphy S.P.Amponsah D.K.Coronary computed tomographic angiography with fractional flow reserve in patients with type 2 myocardial infarction J Am Coll Cardiol 821720231676168710.1016/j.jacc.2023.08.02037777947 · doi ↗ · pubmed ↗
- 4Ola O.Akula A.De Michieli L.Clinical impact of high-sensitivity cardiac troponin T implementation in the community J Am Coll Cardiol 772520213160317010.1016/j.jacc.2021.04.05034167641 PMC 9090513 · doi ↗ · pubmed ↗
- 5Chapman A.R.Shah A.S.V.Lee K.K.Long-term outcomes in patients with type 2 myocardial infarction and myocardial injury Circulation 1371220181236124510.1161/CIRCULATIONAHA.117.03180629150426 PMC 5882250 · doi ↗ · pubmed ↗
- 6Bularga A.Hung J.Daghem M.Coronary artery and cardiac disease in patients with type 2 myocardial infarction: a prospective cohort study Circulation 1451620221188120010.1161/CIRCULATIONAHA.121.05854235341327 PMC 9010024 · doi ↗ · pubmed ↗
- 7De Filippis A.P.Chapman A.R.Mills N.L.Assessment and treatment of patients with type 2 myocardial infarction and acute nonischemic myocardial injury Circulation 1402020191661167810.1161/CIRCULATIONAHA.119.04063131416350 PMC 6855329 · doi ↗ · pubmed ↗
- 8Eggers K.M.Baron T.Chapman A.R.Gard A.Lindahl B.Management and outcome trends in type 2 myocardial infarction: an investigation from the SWEDEHEART registry Sci Rep 1312023719410.1038/s 41598-023-34312-737137939 PMC 10156703 · doi ↗ · pubmed ↗