Comparing the efficacy and safety of bridging therapy vs. monotherapy in patients with minor stroke: a meta-analysis
Abdulsalam Aleid, Saud Aldanyowi, Abdulmajeed Aljabr, Sami Almalki, Awn Alessa, Mostafa Alhodibi, Mohammed Alsuwaylih, Yousef Alanazi, Abbas Almutair

TL;DR
This study compares the effectiveness and safety of bridging therapy versus monotherapy in minor stroke patients, finding similar efficacy but differences in bleeding risks.
Contribution
The study provides a meta-analysis comparing bridging therapy and monotherapy in minor stroke treatment, highlighting safety differences.
Findings
Bridging therapy and IVT monotherapy showed similar efficacy in functional outcomes.
IVT monotherapy had lower risk of symptomatic intracranial hemorrhage compared to bridging therapy.
Mortality rates were comparable across treatment groups, though bridging therapy showed a non-significant trend for better outcomes.
Abstract
The two main therapeutic approaches for stroke treatment are endovascular thrombectomy, which involves mechanically removing the thrombus, and bridging therapy, which uses intravenous thrombolytics (IVT) prior to endovascular thrombectomy (EVT). This study aimed to compare monotherapy (EVT or IVT alone) with bridging therapy (IVT+EVT) in terms of efficacy and safety outcomes in patients with minor ischemic stroke. After a thorough screening, eight studies were included for qualitative synthesis and meta-analysis, comprising a total of 3,117 patients across the treatment arms. The main outcomes of interest were the efficacy of treatment modality, the rate of intracerebral hemorrhage (ICH), and mortality. In terms of functional outcomes measured by the Modified Rankin Score (mRs) 0-1, no significant difference was observed when comparing IVT monotherapy with bridging therapy (IVT+EVT),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
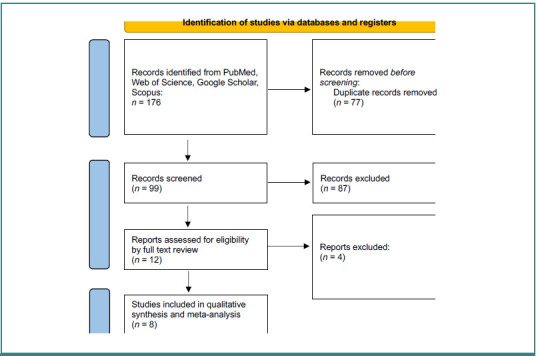 Figure 1
Figure 1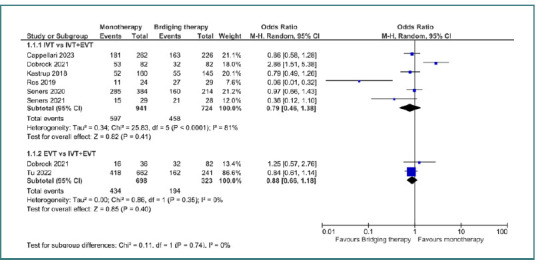 Figure 2
Figure 2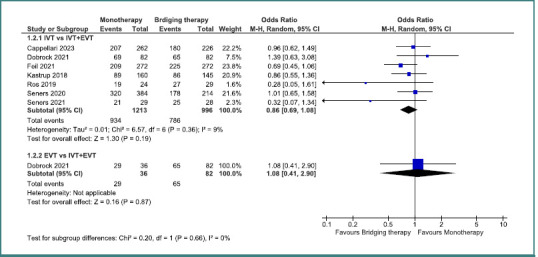 Figure 3
Figure 3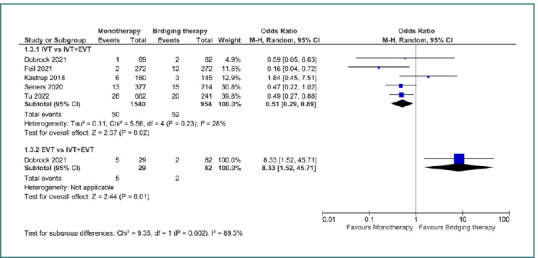 Figure 4
Figure 4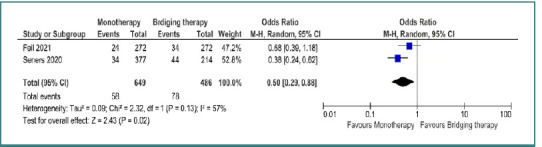 Figure 5
Figure 5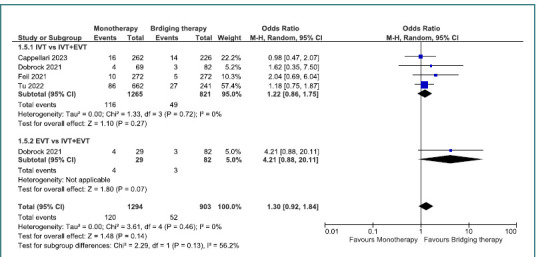 Figure 6
Figure 6| Study name | Representativeness of the exposed cohort (★) | Selection of the non exposed cohort (★) | Ascertainment of exposure (★) | Demonstration that outcome of interest was not present at start of study (★) | Comparability of cohorts on the basis of the design or analysis (max★★) | Assessment of outcome (★) | Was follow-up long enough for outcomes to occur? (★) | Adequacy of follow up of cohorts (★) | Quality level |
|---|---|---|---|---|---|---|---|---|---|
| Dobrocky | ☆ | - | ☆ | ☆ | ☆ | ☆ | - | Moderate | |
| Cappellari | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | High |
| Tu | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | High |
| Seners | ☆ | - | ☆ | ☆ | ☆ | ☆ | ☆ | - | Moderate |
| Kastrup | ☆ | - | ☆ | ☆ | ☆☆ | ☆ | ☆ | - | High |
| Da Ros | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | ☆ | High | |
| Seners | ☆ | - | ☆ | ☆ | ☆ | ☆ | ☆ | - | Moderate |
| Feil | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | High |
| Study ID | Design | Sample size | Age, mean (SD) | Gender, male/female | |||
|---|---|---|---|---|---|---|---|
| Monotherapy | IVT+EVT | Monotherapy | IVT+EVT | Monotherapy | IVT+EVT | ||
| Dobrocky | Cohort | 84, MT: 39 | 85 | 67.7, EVT: 73.1 | 71.1 (30.6–97.3) | IVT: 52/32, EVT: 52/33 | 20/19 |
| Cappellari | Cohort | 262 | 226 | NR | NR | NR | NR |
| Tu | Cohort | EVT:662 | 241 | 65.9(10.5) | 65.7(10.8) | 473/189 | 183/58 |
| Seners | Cohort | 384 | 214 | 71.3 (14.3) | 64.5 (16.6) | 167/217 | 111/113 |
| Kastrup | Cohort | 160 | 145 | 72 (12) | 71 (13) | 67/93 | 65/80 |
| Da Ros | Cohort | 24 | 29 | 68 | 70 (23–92) | 15/9 | 13/16 |
| Seners | Cohort | 29 | 28 | 71 | 67 (56–75) | 18/11 | 18/10 |
| Feil | Cohort | 272 | 272 | 69.4 (13.7) | 68.6 (14) | 154/118 | 154/118 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Venous Thromboembolism Diagnosis and Management · Intracerebral and Subarachnoid Hemorrhage Research
INTRODUCTION
Stroke remains one of the leading causes of mortality and long-term disability worldwide [1]. With an aging population, the global incidence of stroke is expected to increase [2,3]. Acute ischemic stroke occurs due to a thrombus formation, and the primary treatment strategies include endovascular thrombectomy (EVT), which physically removes the thrombus and bridging therapy, where intravenous thrombolytics (IVT) are administered before EVT [4]. The severity of stroke can be assessed through various methods, including the National Institutes of Health Stroke Scale (NIHSS) score [5]. According to the NIHSS, a stroke is considered if the score is below 5 [5]. Despite its classification as 'minor', about 30% of these patients experience lasting disabilities after 90 days [6,7].
Stroke centers and countries vary in how they approach the clinical management of minor ischemic strokes. Intravenous thrombolysis (IVT) remains the recommended treatment for disabling acute ischemic stroke, regardless of the NIHSS score [8]. Although large vessel occlusion (LVO) typically results in severe strokes, approximately 10–20% of patients with minor strokes have LVO due to strong collateral circulation [9,10]. Neurological deficits occur in about 20–40% of these patients, which increases their risk of a poor outcome [11-13]. The current recommendation for patients with LVO and NIHSS scores above 5 is to combine endovascular thrombectomy with IVT [14]. However, few randomized trials have included patients with NIHSS scores of 5 or less, and results from both single-center and multicenter studies have been inconclusive [15-17]. Consequently, the benefit of combination therapy versus IVT alone in these patients remains unclear. A meta-analysis by the HERMES study group found no significant advantage of EVT over standard therapy, including IVT, in patients with NIHSS scores below 10 [14,18]. Nevertheless, observational studies suggest that early thrombectomy may lead to better outcomes in mild stroke compared to optimal medical treatment followed by rescue thrombectomy in cases of deterioration [19,20]. There is also a potential for increased risk of intracerebral hemorrhage (ICH) with combined therapy. Therefore, we performed this systematic review and meta-analysis to evaluate the efficacy and safety of monotherapy (EVT or IVT) versus bridging therapy (IVT & EVT) in patients with minor ischemic stroke.
MATERIAL AND METHODS
This systematic review and meta-analysis followed the Cochrane Handbook for Systematic Reviews and the guidelines outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. The study protocol was registered in the International Prospective Register of Systematic Reviews (ID: CRD42024548143) [21,22].
Database searching
We systematically searched PubMed, Web of Science, Google Scholar, and Scopus for eligible articles from inception to 2023. The search strategy employed the following keywords: “Thrombolysis” AND “Thrombectomy” AND “Stroke” AND (“Minor” OR “Mild”).
Screening process
After conducting the database search, we eliminated duplicates using EndNote version 7 [23]. The remaining articles were uploaded into Rayyan software [24] to facilitate screening. Two authors independently screened the titles and abstracts to assess eligibility, followed by a full-text review of the selected studies. Any disagreements were resolved by a third author (Figure 1).
PRISMA flow diagram of screened articles
Eligibility criteria
We applied predefined inclusion and exclusion criteria during the screening process. We included observational studies and randomized controlled trials (RCTs) that compared monotherapy, whether IVT or EVT, with bridging therapy (IVT+EVT) in patients with minor or mild ischemic stroke (NIHSS score 1–4). Studies that did not compare these two treatment strategies, which involved higher NIHSS scores, case reports, or reviews, were excluded.
Quality assessment
For the included observational cohort studies, the New Castle Ottawa Scale (NOS) was employed to evaluate quality. Studies scoring between 0 and 3 were classified as low quality, 4–6 as moderate, and 7–9 as high quality [25].
Data extraction
Four independent authors used Microsoft Excel to extract baseline information such as study design, sample size, age, and gender, along with outcomes like the Modified Rankin Score (mRS) 0–1, mRS 0–2, mortality, symptomatic intracranial hemorrhage (sICH), and ICH. Any discrepancies were addressed by an author not involved in the data extraction process.
Statistical analysis
We conducted a meta-analysis using Review Manager (RevMan) version 5.4, pooling dichotomous variables to calculate odds ratios (ORs) with corresponding 95% confidence intervals (CIs). A P value ≤ 0.05 was considered statistically significant. Heterogeneity was assessed using the I^2^ statistic, with significance determined by the P value.
RESULTS
Database searching and screening
The database search yielded 176 articles, of which 77 were duplicates and subsequently removed. A total of 99 articles were screened by title and abstract, and 87 articles were excluded during this process. A full-text review was conducted on 12 articles, and 8 articles were included for the qualitative synthesis and meta-analysis. The total number of patients in both treatment arms across the 8 included studies was 3,117 patients (Figure 1).
Quality assessment
According to NOS, five studies were classified as high quality, while three were considered moderate quality [17,26-32] (Table 1).
Baseline characteristics
All included studies were cohort studies, comparing monotherapy (IVT or EVT) versus bridging therapy (IVT+EVT). The baseline characteristics of the included articles are summarized in Table 2.
Meta-analysis
For mRS 0–1, no significant difference was found when comparing IVT monotherapy to bridging therapy (IVT+EVT), with an odds ratio of 0.79 (95% CI, 0.46–1.38; P = 0.41). Similarly, no significant difference was detected between EVT monotherapy and bridging therapy (OR = 0.88; 95% CI, 0.66–1.18; P = 0.4) (Figure 2). For mRS 0–2, no statistically significant differences emerged between IVT monotherapy and bridging therapy, with an OR of 0.86 (95% CI, 0.69–1.08; P = 0.19), and EVT monotherapy versus bridging therapy which yielded an OR of 1.08 (95% CI, 0.41–2.9; P = 0.87) (Figure 3).
Comparison between bridging therapy and monotherapy regarding mRs 0–1
Comparison between bridging therapy and monotherapy regarding mRs 0–2
In terms of symptomatic intracerebral hemorrhage, IVT was associated with a lower risk of sICH compared to bridging therapy, with an OR of 0.51 (95% CI, 0.29–0.89; P = 0.02), whereas EVT was linked to a higher risk of sICH when compared to bridging therapy, with an OR of 8.33 (95% CI, 1.52–45.71; P = 0.01) (Figure 4).
Comparison between bridging therapy and monotherapy regarding symptomatic intracranial hemorrhage
IVT was also associated with a reduced risk of ICH compared to bridging therapy, with an OR of 0.5 (95% CI, 0.29–0.88; P = 0.02) (Figure 5).
Comparison between bridging therapy and intravenous thrombolysis (IVT) regarding intracranial hemorrhage (ICH)
Mortality rates were similar between IVT monotherapy and bridging therapy, as well as EVT monotherapy and bridging therapy. Although there was a slight trend favoring bridging therapy, it was not statistically significant (OR =1.3; 95% CI, 0.92–1.84; P = 0.14) (Figure 6).
Comparison between bridging therapy and monotherapy regarding mortality
DISCUSSION
The objective of this study was to evaluate the efficacy and safety of monotherapy with either IVT or EVT in comparison to bridging therapy (IVT+EVT) for patients with minor ischemic stroke. In terms of efficacy, the results indicated no significant differences between the treatment approaches for mRS 0-1 and mRS 0-2. However, the incidence of sICH and ICH was significantly higher in the group receiving bridging therapy compared to those treated with either IVT or EVT alone. Although EVT was associated with an elevated risk of sICH compared to bridging therapy, this finding was based on a very small sample size from a single study. The meta-analysis revealed that bridging therapy may not provide the same benefits as IVT and poses a higher risk.
The optimal treatment strategy for mild strokes remains uncertain and lacks standardization. Most patients diagnosed with mild stroke receive IVT alone, while a small subset is excluded from IVT due to their condition being perceived as too favorable to receive treatment [33]. Additionally, recent RCT meta-analyses have shown that patients with an NIHSS score below 10 do not gain significant benefit from EVT [14]. Consequently, the use of EVT in patients with LVO and NIHSS ≤ 5 has only been documented in a limited number of case series [12]. Vessel recanalization appears to play a crucial role even in minor strokes, as failure to achieve acute recanalization may result in approximately one-third of minor stroke patients being unable to walk independently at hospital discharge and facing a higher likelihood of neurological decline and poor outcomes at the 90-day follow-up [34-40].
Feil et al. [32] analyzed data from patients enrolled between June 2015 and December 2019 in the Safe Implementation of Treatments in Stroke–International Stroke Thrombolysis Registry (SITS-ISTR) and the German Stroke Registry–Endovascular Treatment (GSR-ET). Their findings indicated that combining EVT with IVT did not significantly enhance functional outcomes compared to IVT alone in patients with minor strokes, specifically those with NIHSS scores ≤5. Although 81.6% of GSR-ET patients treated with EVT or IVT achieved successful reperfusion (mTICI scores 2b–3), follow-up imaging at 24 hours showed a higher point estimate of sICH in patients who underwent both EVT and IVT. Nevertheless, even when performed in extended time windows, thrombectomy was carried out safely, with favorable clinical outcomes of 64%, 75%, and 60%, respectively [15,16,41]. These retrospective single-center studies included 33 patients (NIHSS score ≤8, varying occlusion sites), 41 patients (NIHSS score ≤5, M1 occlusions), and 88 patients (NIHSS score ≤4, different occlusion sites) with LVO and mild stroke symptoms [15,16,41].
Feil et al. [32] further reported that patients who underwent thrombectomy had notably worse functional outcomes when comparing EVT, with or without IVT, to IVT alone. Additionally, those treated with EVT had a higher median NIHSS score at the 24-hour follow-up. Logistic regression analysis revealed that IVT, but not EVT, was a strong predictor of favorable outcomes. These results differ from earlier case series, one of which reported superior outcomes for EVT patients compared to those receiving only IVT, while another case series examined 24 IVT patients alongside 32 interventional cases (19 EVT only and 13 EVT plus IVT) [12,18,30]. In the latter study, a greater shift in NIHSS scores was observed in the group undergoing endovascular procedures compared to those receiving only medical therapy. However, the interpretation of these findings may be biased, as 40% of the thrombectomy patients were ineligible for IVT [30]. Another case series involving 32 thrombectomy patients showed a greater improvement in NIHSS scores, where 25% of those primarily managed with medical therapy did not reach functional independence at follow-up [12]. In a study of 169 patients with M2 occlusion and mild stroke symptoms, no significant difference in favorable outcomes was found among those treated with IVT alone, EVT alone, or a combination of EVT and IVT. However, when analyzing only patients treated after 2015, the shift in mRS scores was significantly better in the EVT group compared to the IVT-only group [17]. Another study involving 96 patients with mild stroke found no difference in favorable clinical outcomes between the IVT group and those receiving standard medical care, although early neurological improvement was observed in IVT patients [42].
A study based on the Swiss Stroke Registry indicated that patients with mild acute ischemic stroke and LVO who underwent either IVT or EVT achieved favorable functional outcomes at three months [43]. However, further research is required to clarify the necessity of both IVT and EVT in patients with acute LVO stroke. A meta-analysis of individual patient data from five randomized trials demonstrated that EVT was more effective than standard medical treatment in cases of acute ischemic stroke caused by proximal anterior circulation artery occlusion [14]. However, the SKIP Randomized Clinical Trial did not show functional differences between the EVT and bridging groups [44]. Subsequent trials suggested that EVT alone might yield similar results to bridging therapy for patients with acute ischemic stroke due to major artery occlusions [45-47]. Interestingly, improved functional outcomes were observed in patients with large vessel occlusion stroke who received adjunct intra-arterial thrombolysis after a successful angiographic thrombectomy [48]. Moreover, findings from the Italian registry on endovascular treatment for acute stroke suggest that bridging therapy may reduce the risk of death or severe disability three months after a stroke, particularly in cases of major artery occlusion [49]. A meta-analysis involving three RCTs and six observational studies concluded that direct EVT might be as effective as bridging therapy, with a lower likelihood of intracerebral hemorrhage (ICH) and clot migration in patients with acute ischemic stroke [50]. Likewise, another meta-analysis of five observational studies reported that bridging therapy and EVT might be equally effective in managing acute anterior circulation strokes [51]. In contrast, a single-center retrospective study of 90 consecutive patients found that bridging therapy was associated with substantially higher direct and overall hospital costs than EVT alone, without demonstrating superior clinical outcomes [52]. Furthermore, Qureshi et al. [53] suggested that EVT alone may be more cost-effective than bridging therapy for treating acute ischemic stroke patients within 4.5 hours of symptom onset, although the study did not establish the cost-effectiveness of bridging compared to direct thrombectomy.
The limitations of the study include the fact that all the articles were cohort studies, with some having small sample sizes. Additionally, certain outcomes were based on limited sample sizes, which may have reduced the statistical power to detect significant differences. Therefore, future large-scale randomized controlled trials and an updated systematic review in the next five to ten years are recommended.
CONCLUSION
The present results regarding efficacy outcomes revealed no statistically significant differences between the two treatment approaches in terms of mRs 0–1 and mRs 0–2. However, when bridging therapy was used instead of IVT, the safety outcomes, such as sICH and ICH, were statistically considerably higher. Furthermore, there were no discernible variations in the death rates between the two therapy modalities.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chao BH Yan F Hua Y Liu JM Yang Y Ji XM Stroke prevention and control system in China: CSPPC-Stroke Program Int J Stroke 2021 Apr 16326527210.1177/174749302091355732223541 · doi ↗ · pubmed ↗
- 2Wu S Wu B Liu M Chen Z Wang W Anderson CS Stroke in China: advances and challenges in epidemiology, prevention, and management Lancet Neurol 2019 Apr 18439440510.1016/S 1474-4422(18)30500-330878104 · doi ↗ · pubmed ↗
- 3Tu WJ Hua Y Yan F Bian H Yang Y Lou M Prevalence of stroke in China, 2013-2019: A population-based study Lancet Reg Health West Pac 2022 Jul 302810055010.1016/j.lanwpc.2022.10055036507089 PMC 9727498 · doi ↗ · pubmed ↗
- 4Santos-Gallego CG Bayón J Badimón JJ Thrombi of different pathologies: implications for diagnosis and treatment Curr Treat Options Cardiovasc Med 2010 Jun 1232749110.1007/s 11936-010-0075-820842548 · doi ↗ · pubmed ↗
- 5Zhuo Y Qu Y Wu J Huang X Yuan W Lee J Estimation of stroke severity with National Institutes of Health Stroke Scale grading and retinal features: A cross-sectional study Medicine (Baltimore)2021 Aug 610031 e 2684610.1097/MD.000000000002684634397858 PMC 8341321 · doi ↗ · pubmed ↗
- 6Khatri P Conaway MR Johnston KC Acute Stroke Accurate Prediction Study (ASAP) Investigators Ninety-day outcome rates of a prospective cohort of consecutive patients with mild ischemic stroke Stroke 2012 Feb 432560210.1161/STROKEAHA.110.59389722052513 PMC 3426999 · doi ↗ · pubmed ↗
- 7Romano JG Smith EE Liang L Gardener H Camp S Shuey L Outcomes in mild acute ischemic stroke treated with intravenous thrombolysis: a retrospective analysis of the Get With the Guidelines-Stroke registry JAMA Neurol 2015 Apr 7244233110.1001/jamaneurol.2014.435425642650 · doi ↗ · pubmed ↗
- 8Powers WJ Rabinstein AA Ackerson T Adeoye OM Bambakidis NC Becker K 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association Stroke 2018 Mar 493e 46e 11010.1161/STR.000000000000015829367334 · doi ↗ · pubmed ↗